Clinical Manifestations and Diagnosis
Dermatophytosis can be located on any part of the animal body and usually manifests as a regular and circular focus generally accompanied with alopecia and desquamation. The lesion spread centrifugally from the site of inoculation; multiple lesions can merge into large foci with irregular margins.
The lesion can be erythematous over the entire surface but especially on the periphery. It can be covered by pustules and later by exudate and crusts. Other clinical signs may be present, such as pruritus accompanied by scratching and behavior change. Animal dermatophytosis has usually self-limiting nature, and spontaneous regrowth of hairs is generally observed. Infection is usually restricted to the dead cornified layers of the skin because of the inability of the dermatophytes to attack the deeper layers of the skin or organs of immunocompetent hosts. Naive, usually young, animals can be heavily infected with significant impact on health condition and growth. The increased susceptibility of young animals may also reflect differences in the biochemical properties of the skin and skin secretions (especially sebum), growth and replacement of hair, and the physiologic status of the host as related to age. Animals can exhibit subtle signs or act as “asymptomatic” carriers of dermatophytes without history of dermatophytosis as seen relatively commonly in cats infected by M. canis or guinea pigs infected by T. benhamiae. Regardless of the possibility of more virulent strain emergence, many factors related to the host play a critical role in determining the type of clinical lesions produced and terminating the infection. More comprehensive reviews and monographs are available on this topic (Donnelly et al. 2000; Chermette et al. 2008; Miller et al. 2013; Moretti et al. 2013).In companion animals (cats, dogs, or small mammals like rabbits, guinea pigs, and chinchillas) as well as in large animals (horses and cattle), dermatophytes are frequently responsible for skin diseases including alopecia and crusts.
Dermatophytosis is a contagious disease, and cases are regularly reported in breeding facilities and farms. Human contamination is also indicative. However, experimental diagnosis is systematically required. The use of the Wood's lamp is recommended when M. canis infection is suspected in companion animals. The microscopic examination of hairs and scales can be performed from skin scrapings (Fig. 3.2). According to the dermatophytes species, arthroconidia have different dimensions and disposition on the hairs: M. canis produces clusters of very small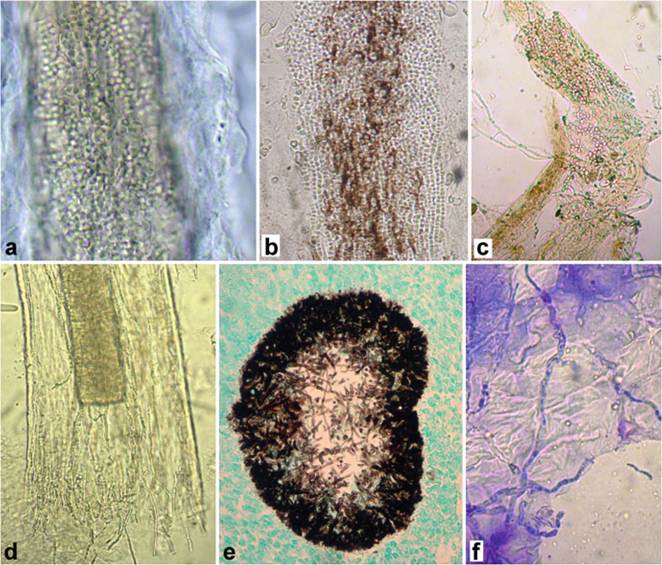
Fig. 3.2 Laboratory diagnosis of dermatophytosis by using direct microscopic examination or histology. (a) Arthroconidia of Microsporum canis at direct hair examination (digestion in 20% NaOH). (b) Arthroconidia of Trichophyton benhamiae at direct hair examination (digestion in 20% NaOH). (c-d) Arthroconidia of Trichophyton verrucosum at direct hair examination (digestion in 20% NaOH). (e) Histopathological examination (Gomori-Grocott staining) of pseudomycetoma in a cat due to M. canis. (f) Cytological examination in case of human dermatophytosis due to zoophilic Trichophyton mentagrophytes (scotch tape technique)
(2-4 μm) arthroconidia, whereas members of the genus Trichophyton form chains of arthroconidia (Chermette et al. 2008). Fungal culture is still considered as the golden standard for diagnosis. Samples of hairs, crusts, scales, or even cutaneous tissue (in the specific case of pseudomycetoma) should be collected for culture. When a large number of colonies of dermatophyte develop on the culture medium, active infection is demonstrated. When only a few colonies develop on the culture medium, subclinical infection or mechanical carriage (especially in cats or guinea pigs) should be suspected. When unusual clinical presentations are observed, histological examination is recommended (Fig. 3.2).
Sensitivity of both direct microscopic examination and cultivation depends on the combination of host and pathogen.
Microscopic examination fails to provide the identification of the agent, whereas culture has usually several weeks turnaround time and the requirement of mycological expertise. The reliance on culture, which may be often unsuccessful for some dermatophyte species, can be substituted by PCR-based tests that are now available for the direct diagnosis of dermatophytosis from clinical samples and significantly reduces the time of diagnosis (hours to days). These methods can suitably supplement or even replace classical diagnostic schemes thanks to their high sensitivity and specificity. They are represented by conventional PCR, RT-PCR, or more complex methodologies (PCR-ELISA, PCR-RLB, microarrays) and usually offer opportunity to detect DNA of any dermatophyte without species identification, but some more recently developed assays are able to identify relatively broad spectrum of species including major zoophilic species (Jensen and Arendrup 2012; Cafarchia et al. 2013b; D¾browska et al. 2014; Mehlig et al. 2014; Kupsch et al. 2016).3.4