Common principles of IBD
9.2.5.1 Etiology and pathogenesis
The underlying etiology of idiopathic IBD in small animals is, by definition, unknown. However, analogies have been drawn to IBD in humans and the breakdown of immunological tolerance to luminal antigens (bacteria and dietary components) is thought to be crucial in the pathogenesis of this disorder.3
Table 9.4: Histopathological classification of idiopathic inflammatory bowel disease
Histopathological description Comment
Lymphoplasmacytic enteritis (LPE)
Basenji enteropathy
Familial PLE and PLN in Soft-coated Wheaten Terriers
Lymphoplasmacytic colitis
Eosinophilic enteritis (EE); eosinophilic gastroenteritis (EGE); eosinophilic enterocolitis (EEC); eosinophilic gastroenterocolitis (EGEC)
Granulomatous enteritis
Regional enteritis
Neutrophilic enteritis
Histiocytic ulcerative colitis
Most common form
Possibly a variant of LPE
Possibly a variant of LPE
May occur in isolation or with LPE
Marked increase in eosinophils noted
Rare as idiopathic disease, but reported as a sequel of FIP infection in cats
Possibly the same as granulomatous enteritis
Rare in dogs, uncommon in cats
Most common in Boxers
Potential infectious etiology
The loss of tolerance probably results from disruption of the mucosal barrier, dysregulation of the immune system, disturbances in the intestinal microflora, or a combination of these events.
Although the clinical benefit of dietary therapy in some patients with IBD suggests a role for diet-related factors, extrapolation from experimental rodent models of IBD and natural IBD in humans, suggest that antigens derived from the endogenous microflora are more important in the disease pathogenesis. In contrast to a specific, active immune response against an enteropathogen, the default response of the healthy mucosa to luminal antigens is tolerance. As the majority of antigens are derived from innocent dietary components or the GI microflora, the mounting of an active response to such ubiquitous antigens would be both wasteful and potentially harmful, since it could lead to uncontrolled inflammation.Genetic factors are likely to contribute to the pathogenesis of IBD and in humans there are strong associations with the human major histocompatibility complex (human leukocyte antigen; HLA) genes.4,5 In addition, a mutation of the NOD2 gene is present in some human patients with CD.6,7 The product of the NOD2 gene detects bacterial lipopolysaccharide and can activate the pro-inflammatory nuclear transcription factor NF-κB. Aberrant immune responses to bacteria may therefore develop in affected individuals. Similar genetic factors predisposing to IBD are also likely to play a role in canine and feline IBD, given the recognized breed predispositions, although studies are lacking.
Whilst the mechanisms by which mucosal tolerance occurs have been well characterized, a fundamental question that remains unresolved is how the gut-associated lymphoid tissue (GALT) decides when to and when not to become tolerant. If idiopathic IBD does indeed represent a breakdown in mucosal tolerance to the endogenous bacterial flora, the reason why this occurs is also unresolved. Hence, in order to begin to understand the etiology and pathogenesis of IBD, an understanding of the normal small intestinal (SI) bacterial flora and its interaction with the intestinal immune system is essential.
Bacterial flora
The normal SI microflora is a diverse mixture of aerobic, anaerobic, and facultatively anaerobic bacteria, and plays an integral part in SI health. It influences a wide variety of functional parameters such as villus size, enterocyte turnover, brush border enzyme turnover, and intestinal motility. The digestion and absorption of fats, carbohydrates, amino acids (such as taurine), and vitamins (such as cobalamin and folate) are also affected by intestinal bacteria.
Bacterial numbers increase from duodenum to colon, but there is no consensus as to what constitutes a “normal” number of organisms in healthy animals. Some studies suggest that the proximal SI of healthy dogs can harbor up to 109 colonyforming units (CFU)∕ml total bacteria, and these numbers are considerably higher than the numbers (production, suggesting roles in epithelial surveillance and maintenance of mucosal immune homeostasis.
The CD4+ T-cell population is a major cytokine-producing cell population, but different populations exist with different patterns of cytokine secretion, by which they can regulate the humoral and cell-mediated arms of the immune system. Two principal populations are postulated: a T-helper 1 (Th1) population that produces interleukin 2 (IL-2), interferon γ (IFN-γ), and tumor necrosis factor β (TNF-β), and a T-helper 2 (Th2) population producing IL-4, IL-5, IL-6, and IL-10.15 Other populations with down-regulatory functions, which predominantly secrete tranforming growth factor β (TGF-β) or IL-10 respectively, have also been proposed.16
Although lymphocytes and plasma cells predominate in the intestinal mucosa, other immune cells are also present. Macrophages have functions including phagocytosis, antigen presentation, and immunoregulatory roles, mediated by the secretion of cytokines, chemokines, and inflammatory mediators including TNF-α, eicosanoids, and leukotrienes. Neutrophils are present in smaller numbers, although their numbers do increase during mucosal inflammation. Both mast cells and eosinophils can be found and actively produce chemical mediators (e. g., histamine, heparin, eicosanoids, and cytokines).
In addition to digestive functions, enterocytes have important immune functions. First, they are an important component of the mucosal barrier, controlling the uptake of antigens. Second, they may be capable of antigen presentation, through the expression of MHC II, and non-classical antigen-presenting molecules.17 Finally, enterocytes can produce inflammatory mediators, chemokines and cytokines, and may regulate immune responses in both the epithelial and LP compartments.
Mucosal tolerance
Acquired immune responses develop after a series of steps involving antigen uptake, presentation to naive lymphocytes, co-stimulation by helper cells, clonal expansion, homing to effector sites, and performance of effector functions. The specific mechanisms involved are described in detail elsewhere.18 In the SI, a large array of cytokines is present, and can be grouped into pro-inflammatory, immunoregulatory, and chemokinetic cytokines. Many other cell types may also produce cytokines (see above), and consequently an overall cytokine environment exists, which determines the predominant type of immune response that develops.
Mucosal tolerance can result either from anergy/deletion (by apoptosis) of antigen-specific T-cells, or by active suppression through antigen-specific suppressor cells.19 The CD4+ αβ T- cell subset that mediates active suppression either produces down-regulatory cytokines (e.g., TGF-β or IL-10) or functions through cell-cell interactions.16 Furthermore, since TGF-β and IL-10 are also important in IgA production, generation of mucosal tolerance could potentially occur in parallel to a specific IgA response, which helps to maintain tolerance by immune exclusion.
As mentioned previously, the mucosal immune system must determine when to generate a specific immune response (e. g., towards a pathogen), and when to remain tolerant (e.g., to commensal bacteria or food components). The most workable hypothesis currently is the “danger theory”, which is based on the supposition that the type of response depends upon the context in which the antigen is presented.19 When the mucosa is invaded by a pathogen, cell damage leads to release of “danger signals” (i.e., inflammatory mediators, such as pro-inflammatory cytokines and chemokines). Hence the nature of the immune response generated changes from tolerance to active immune response and can either be Th1-dominated (i.e., cytotoxicity and IgG response) or Th2-dominated (i.e., IgE response).
Such an immune response is aimed at eliminating the pathogen completely, but by-stander damage to host cells can occur, particularly if the danger persists, either because the mucosal barrier remains breached and the pathogenic insult continues unabated or because there is an inherent abnormality of the GALT. A state of chronic inflammation develops, which may lead to a breakdown in tolerance to harmless antigens (i.e., food components and commensal bacteria). The chronic inflammation ultimately leads to histological changes, which are generally similar regardless of the inciting cause.Mucosal inflammation
A number of inciting causes (including infection, ischemia, trauma, toxins, neoplasia, and immune-mediated reactions) can cause a cellular and vascular response, collectively known as inflammation. The normal mucosa is usually tolerant of endogenous bacteria and food antigens, but can be considered to be in a state of “controlled inflammation”. As postulated above, disruption of the mucosal barrier, dysregulation of the immune system, disturbances in the intestinal microflora, or a combination of these events can destabilize the system and may trigger uncontrolled inflammation.
Experimental rodent models of GI inflammation have permitted a better understanding of the pathogenesis of mucosal inflammation, and the mechanisms that trigger it.3 These genetically engineered animals possess a variety of spontaneously arising or induced disruptions of the mucosal barrier, the mucosal immune system, or the endogenous microflora, all leading to chronic inflammation with a similar histological appearance. Whatever the model, the presence of an enteric flora is essential for the expression of disease and intestinal inflammation does not develop when the rodents are reared in a germ-free environment.20 This final point demonstrates the importance of the endogenous flora in the pathogenesis of uncontrolled mucosal inflammation. This has been confirmed by studies showing that normal humans are tolerant to their own intestinal microflora, but that this tolerance is broken in patients with IBD.21
9.2.5.2 Clinical presentation
Idiopathic IBD is generally considered the most common cause of chronic vomiting and diarrhea in dogs and cats, but its true prevalence is unknown.
In reality, the condition is most likely overdiagnosed, due to the ease of getting endoscopic intestinal biopsies, the difficulties in interpretation of histopathological specimens (particularly if collected endoscopi-Table 9.5: Clinical signs associated with inflammatory bowel disease
Vomiting
■ bile and/or food
■ hair in cats
■ grass in dogs
■ hematemesis
Small intestinal-type diarrhea
■ large volume
■ watery
■ melena
Large intestinal-type diarrhea
■ hematochezia
■ mucoid stool
■ frequency and tenesmus
Abdominal discomfort/pain
Excessive borborygmus and flatus
Thickened bowel loops
Weight loss
Altered appetite or anorexia
Polyphagia
Eating grass or pica
Hypoproteinemia and/or ascites
cally), and the failure to adequately rule out other causes of mucosal inflammation. No apparent gender predisposition has been reported in dogs or cats, but in both species IBD is considered to be more common in middle-aged animals. IBD is uncommon in animals less than 6 months of age, when anatomical, infectious, and dietary causes of diarrhea are much more prevalent.
Although idiopathic IBD can potentially occur in any dog or cat breed, certain breed predispositions have been recognized. Examples include LPE in German Shepherd dogs and Siamese cats, EGE in German Shepherds, and lymphoproliferative enteropathy in Basenjis. A concurrent PLE and PLN has been reported in Soft-coated Wheaten Terriers. Shar Pei dogs often have severe LPE with hypoproteinemia and extremely low serum cobalamin concentrations. In cats, a syndrome, termed “triaditis”, has been reported that is characterized by concurrent lymphoplasmacytic IBD, lymphocytic cholangitis, and chronic lymphocytic pancreatitis.22
Vomiting and diarrhea are the most common clinical signs in patients with IBD, but an individual patient may show some or all of the signs listed in Table 9.5. The clinical signs may wax and wane, and an obvious precipitating event may be evident (e. g., stress, acute GI infection, or dietary change). The appetite is often variable. Polyphagia may be present in the face of significant weight loss, whilst anorexia occurs with severe inflammation. Milder inflammation may not affect the appetite, although post-prandial pain can be significant even without other signs.
The nature of the GI signs can be correlated approximately with the region of the GI tract that is affected: vomiting and hematemesis are more common if gastric or upper SI inflammation is present, and in cats vomiting is often the predominant sign of SI IBD. Large intestinal (LI)-type diarrhea may be the result of colonic inflammation, or may result from prolonged SI diarrhea or the presence of agents that stimulate colonic secretion (e. g., bacteria, bacterial toxins, deconjugated bile acids, or hydroxylated fatty acids). Blood in the vomit or diarrhea is usually associated with more severe disease and, most often, eosinophilic inflammatory infiltrates.
Severe, chronic disease is associated with weight loss and PLE, even leading to hypoproteinemia and ascites. The measurement of fecal loss of alpha1-proteinase inhibitor appears to be a sensitive test for PLE before hypoproteinemia develops. The serum concentrations of both albumin and globulin are reduced in most patients with PLE. Exceptions to the typical panhypoproteinemia are due to increased globulin production caused by immune system stimulation (e. g., immunoprolifera- tive SI disease in the Basenji, see 9.2.5). Renal and hepatic causes of hypoalbuminemia can be eliminated by assay of serum bile acids concentrations and the urinary protein /creatinine ratio. Hypocholesterolemia and lymphopenia can also be seen in patients with PLE. Ionized hypocalcemia and hypomagnesemia have also been reported.
Physical examination findings may include edema, ascites, emaciation, thickened intestines, melena, and hematochezia (Figure 9.6). Thrombo-embolism and remote organ failure is a feature seen in some patients with PLE. Other systemic consequences of IBD, such as thrombocytopenia, can occur although reports are sparse.23
9.2.5.3 Diagnosis
Although the clinical signs and physical examination findings may be suggestive of IBD, ultimately intestinal biopsy is necessary for a definitive diagnosis. Since the term idiopathic IBD is restricted to cases in which intestinal inflammation is found without any obvious underlying cause, all other etiologies must be excluded before a diagnosis of IBD can be made. Therefore, before intestinal biopsies are collected, laboratory
evaluation and diagnostic imaging must be performed. Such investigations are not intended to provide a definitive diagnosis of IBD, but to help eliminate the possibility of extra-intestinal disease (e. g., pancreatitis, hypoadrenocorticism, renal failure, and hepatic failure), anatomic intestinal disease (e.g., tumor or intussusception), or known causes of intestinal inflammation. Furthermore, by determining whether focal or diffuse intestinal disease is present, the most appropriate method of intestinal biopsy can be chosen.
Laboratory testing - Hematology
It is not unusual for the hematological examination to be completely unremarkable in animals with IBD. Occasionally, neutrophilia, with or without a left shift, is noted, and reactive atypical lymphocytes may be seen in patients with LPE. It has been suggested that eosinophilia is indicative of EGE, but it is not pathognomonic. If anemia is present, it may be a reflection of chronic inflammation or chronic blood loss. Anemia due to blood loss is usually strongly regenerative in nature and is initially, normocytic, normochromic. However, an iron deficiency anemia, characterized by microcytosis, hypochromasia, and thrombocytosis, may eventually develop.

Figure 9.6:
Cocker Spaniel with PLE. An eight-year-old female Cocker Spaniel with a proteinlosing enteropathy and signs of diarrhea, weight loss, and ascites associated with hypoalbuminemia (1.2 g/dl). The dog initially responded well to treatment with immunosuppressive doses of steroids, but after 3 months, as the dose of steroids was tapered, hypoproteinemia recurred and the dog was euthanized after developing severe dyspnea, suspected to be a result of pulmonary thromboembolism.
Laboratory testing - Serum biochemistry profile
In many patients with IBD, the serum biochemistry profile is within normal limits. However, testing allows diseases of other organ systems to be recognized or excluded. Hypoalbumin- emia and Eypoglobulinemia are characteristic of a PLE, whilst hypocholesterolemia may suggest malabsorption. Furthermore, intestinal inflammation in dogs may cause a reactive hepatopathy with mild to moderate (2-4 fold) increases in liver enzyme (ALT, ALP) activities. In contrast, due to their shorter half-lives, any liver enzyme increases in cats are more likely to be the result of primary liver disease, although concurrent IBD and cholangitis are commonly seen in cats.
Laboratory testing - Fecal examination
Fecal examination by flotation techniques is very important in eliminating known parasitic causes of mucosal inflammation. For example, nematodes (e.g., Trichuris, Uncinaria, or Ancylos- toma) and Giardia can be diagnosed by fecal smear and/or flotation. However, given that fecal examination and even a fecal ELISA for Giardia antigen may not always detect the presence of these important causes of intestinal inflammation and diarrhea, empirical treatment with fenbendazole is recommended in all cases.
Culture for bacterial pathogens such as Salmonella spp., Campylobacter spp., or Clostridium spp. is more problematic, as these organisms can be found in the stools of healthy animals, and their presence in patients with IBD does not necessarily prove a causal relationship.
Significant intestinal protein loss probably develops in patients with IBD before hypoproteinemia occurs. Increased fecal α1- proteinase inhibitor concentrations would be expected before PLE can be recognized clinically.
Laboratory testing - Serum folate and cobalamin concentrations
The measurement of serum folate and cobalamin concentrations is now commercially available for dogs and cats, and folate and cobalamin deficiency associated with IBD has been documented. As the serum concentrations of both of these water-soluble vitamins are affected by intestinal malabsorption, proximal, distal, or diffuse SI inflammation can result in decreased folate concentration, decreased cobalamin concentration, or both. Although such alterations are not pathognomonic, such deficiencies in IBD may require therapeutic correction. In particular, cobalamin deficiency may in itself have systemic metabolic consequences and may also cause intestinal dysfunction.24 Also, anecdotal evidence suggests that the response to immunosuppressive therapy for IBD may be subop- timal until cobalamin deficiency is resolved.
Diagnostic imaging
Radiographic and ultrasonographic studies are performed to document whether focal or diffuse disease is present, to document any anatomical GI disease, and to show any involvement of other abdominal organs. Used in conjunction with specific clinical signs and laboratory testing, the information from imaging studies enables an appropriate choice of a biopsy method (i.e., upper or lower GI endoscopy, or exploratory laparotomy) that will most likely lead to a definitive diagnosis.
Survey radiographs may be useful for identifying anatomical disease, whilst contrast studies rarely add further information. Ultrasonographic examination is superior to radiography for documenting focal intestinal disease. In addition, ultrasound- guided fine-needle aspiration can provide samples for cytological analysis.
Abdominal ultrasonography in IBD patients permits the evaluation of intestinal wall thickness, and can help document mesenteric lymphadenopathy.25,26 It has been suggested that IBD is associated with increased intestinal wall thickness; however, this was not found to be true in a large case series.27 In that case series, the intestinal wall thickness was only markedly increased if hypoproteinemia in a patient with PLE caused bowel wall edema. Furthermore, loss of the normal intestinal layering is indicative of neoplasia rather than IBD.
Intestinal biopsy
Intestinal biopsy is essential to prove the presence of intestinal inflammation and thus to confirm a diagnosis of IBD. Endoscopic biopsy is the simplest and least invasive method of specimen collection, although numerous limitations exist, including small sample size, superficial and often fragmented samples, and the fact that tissue can only be collected from the stomach, proximal SI, distal ileum, and colon. In some cases, exploratory celiotomy and full-thickness biopsy are necessary, although this is more invasive and wound healing can be problematic if severe hypoproteinemia is present and corticosteroids need to be given urgently. However, it may be more suitable for cats, given the tendency for concurrent hepatic and pancreatic involvement and the small size of endoscopic biopsies that can be achieved in this species.
The endoscopic appearance of the intestinal mucosa can give some clue as to the presence of intestinal inflammation. Increased granularity, irregularity, and friability with the presence of erosion, ulceration, and spontaneous hemorrhage are all potential markers of IBD (Figure 9.7). However, interpretation of the gross appearance of the mucosa is quite subjective, and obvious macroscopic changes are not invariably present despite histological evidence of even quite marked inflammation. Furthermore, similar changes are seen in other intestinal conditions, especially intestinal neoplasia.
The pattern of histopathological changes in biopsy specimens that is reported depends upon the type of IBD present (see above).Yet, while the histopathological assessment of intestinal biopsies remains the gold standard for the diagnosis of many intestinal diseases, it has marked limitations. For example, biopsy specimens can be normal by light microscopy in almost half of cats and dogs with chronic GI disease and suspected IBD. This suggests that either many patients do not have IBD and their disease is caused by functional rather than morphological abnormalities, or that sampling and interpretive problems occur.
A major problem of histopathological diagnosis is the poor agreement between histopathologists. This may be due to poor quality endoscopic biopsies, the subjective nature of interpretation of the degree of inflammation, the patchiness of inflammation, or the presence of edema (due to hypoproteinemia) leading to difficulties in assessing cell density.28 In a recent study, even an incorrect diagnosis of lymphoma was made by a histopathologist assessing tissues from a healthy dog.29
The distinction of severe LPE from lymphoma can be difficult, particularly with endoscopic biopsies as the histological confirmation of lymphoma is made most readily when lymphocytic infiltration of muscle layers is seen on full-thickness surgical biopsy specimens.
Histopathological scoring schemes and standardized criteria (Table 9.6) have been suggested as a means of improving agreement, but marked variability in interpretation still exists. A WSAVA-sponsored GI Standardization Group has been established to try to resolve these inconsistencies, and a standard grading scheme that assesses architectural abnormalities in conjunction with changes in cellularity is being developed.23
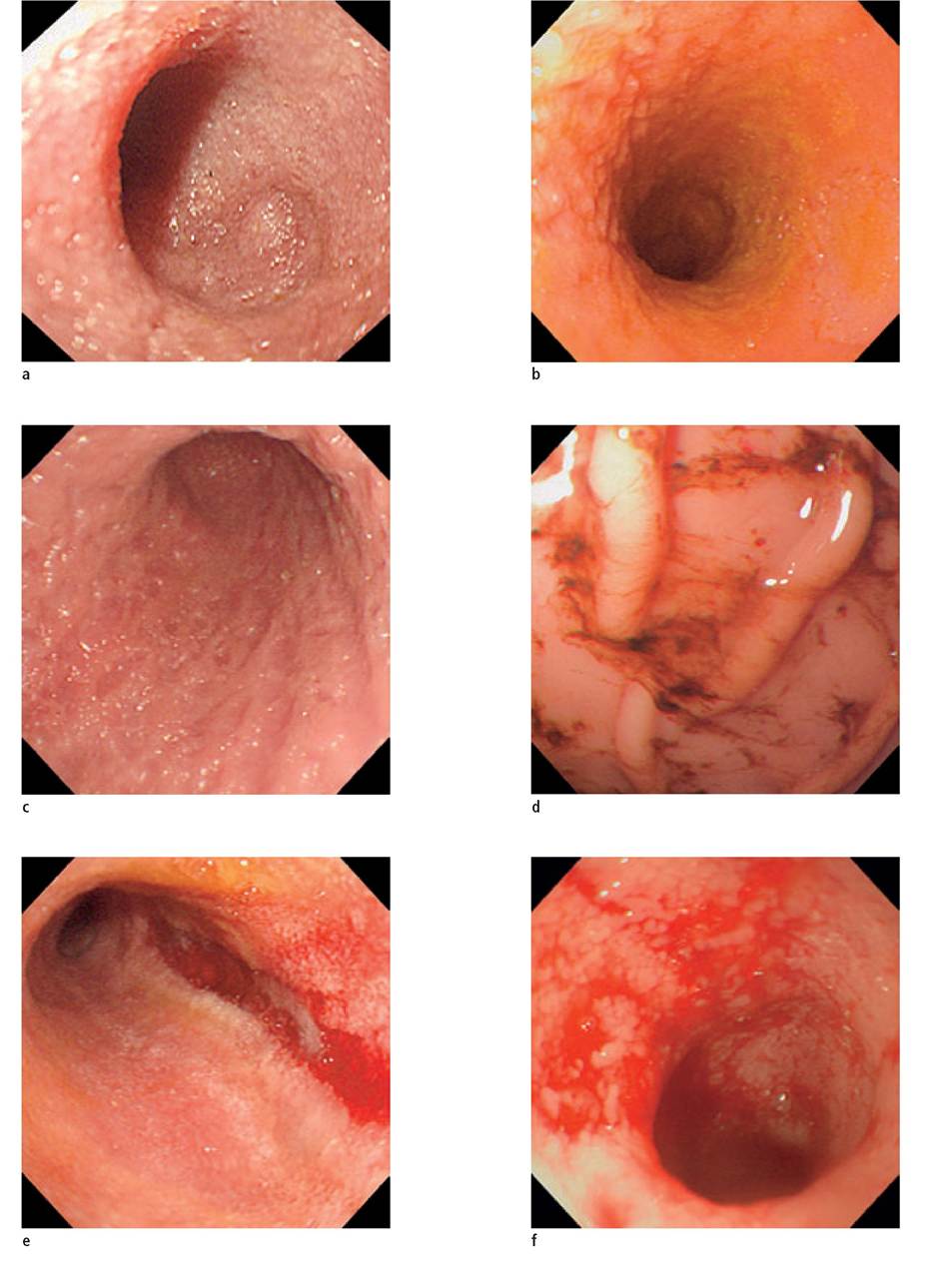
Figure 9.7:
Endoscopic appearance of the intestine of patients with varying degrees of inflammatory bowel disease.
(a) Mild lymphoplasmacytic enteritis in a dog, showing increased granularity.
(b) Moderate lymphoplasmacytic enteritis in a cat, showing a classical “cobblestone” appearance.
(c) Severe lymphoplasmacytic enteritis in a dog, showing erosions and ulcers.
(d) Eosinophilic gastritis in a dog.
(e) Eosinophilic enteritis in the same dog as shown in d.
(f) Histiocytic ulcerative colitis in a Boxer, showing severe ulceration and hemorrhage.
Table 9.6: Criteria for the histological assessment of intestinal biopsies
Epithelium Crypts and villi
■ enterocyte height
■ erosions
■ goblet cell number and size
■ intraepithelial lymphocyte density
Lamina propria
■ immune cell density
■ lymphangiectasia
■ predominant cell type
■ crypt abscessation
■ crypt depth
■ crypt-villus ratio
■ mitotic index
■ villus clubbing and fusion
■ villus height and width
Miscellaneous
■ edema
■ fibrosis
■ hyperemia or congestion
■ infectious agents
■ neoplasia
Alternate examinations of biopsy specimens are largely experimental, but can provide significant information. Examinations available in some institutions include electron microscopy, biochemical assays for brush border enzyme activities, immunocytochemical characterization of B-cells, T-cells, and their subsets (CD4, CD8, etc.) by histology and flow cytometry, immunocytochemical localization of MHC expression, assays for cytokine mRNA expression, and assessment ofT-cell clonality.11-13,30,31
Ultimately, the primary clinician should interpret histopathology results cautiously and try to relate them to the clinical presentation. The results should be questioned if the histopathological diagnosis does not fit the clinical picture or the response to apparently appropriate therapy is poor. In some cases, repeat biopsy (e. g., by exploratory laparotomy) may be required.
In humans, activity indices are used to quantify disease severity in IBD patients, aiding the assessment of the response to treatment and allowing comparisons between published studies in the literature. Recently, an activity index has been suggested for canine IBD patients (Table 9.7) that may aid in disease classification in the future.32
9.2.5.4 Treatment
The treatment of IBD usually involves a combination of dietary modification, antibacterials, and immunosuppressive therapy, regardless of the histological type diagnosed. Most recommendations are based upon individual experience as objective information on efficacy is generally lacking. The authors recommend a staged approach to therapy whenever possible, except in seriously ill patients where immediate intervention with immunosuppressive medication may be essential. Such a logical, staged approach involves initial treatment with antiparasitic agents to eliminate any occult endoparasite infestation. Sequential therapeutic trials with an exclusion diet and antibacterials should also be undertaken. Immunosuppressive medication is used only as a final resort. If the clinical signs are intermittent, the owners should keep a diary to provide objective information as to whether treatments produce genuine improvement. In addition, changes in the IBD activity index may provide objective evidence of treatment success or failure.
Intravenous fluid therapy should be given if the patient is dehydrated, but most patients with IBD have chronic disease and have reached a compensatory state, and so do not need fluid support. If PLE and hypoproteinemia are present, plasma transfusion may be indicated during the peri-operative period associated with intestinal biopsy. Diuretics may reduce ascites: spironolactone at 1-2 mg/kg PO q 12 h may be more effective than furosemide for treating ascites. Thromboembolism is present in some patients with PLE, and prophylactic low-dose aspirin at 0.5 mg/kg PO q 12 h has been advocated in dogs with PLE.
Diet and dietary supplements
The diets recommended for patients with IBD are either based on an easily digestible diet or on a single-source protein, single-source carbohydrate diet. Single-protein, single-carbo- hydrate source diets may be considered antigen-limited. Ideally, they contain a protein source that is novel to the patient and are true exclusion diets. An alternative approach is to use a diet containing hydrolyzed protein. The authors recommend that a full dietary trial should be employed in all cases of unexplained intestinal inflammation to exclude the possibility of an adverse food reaction. Most clients are willing to try this first, given concerns over the side-effects of immunosuppressive drugs, but in severely ill animals it may be necessary to give concurrent immunosuppressive therapy with the dietary trial, and then see if remission is maintained when the drug therapy is gradually withdrawn.
A novel, highly digestible diet will decrease intestinal antigenic load, and thus decrease mucosal inflammation. Such diets may also help to resolve any sensitivity to dietary components that may have arisen secondary to disruption of the mucosal barrier. After resolution of the inflammation, the original diet can be re-introduced without the fear of an acquired sensitivity. Well-cooked rice is the preferred carbohydrate source because of its high digestibility, but potato, corn starch, and tapioca are alternative options. It is probably appropriate that they are also gluten-free, although the prevalence of gluten-sensitivity in dogs and cats is unclear. If severe malabsorption is evident, fat restriction may reduce clinical signs. However, fat restriction is
rarely necessary and may make it more difficult to resolve weight loss. Modification of the n3:n6 fatty acid ratio may also modulate the inflammatory response and have some benefit in treatment and maintenance of remission.33,34 However, there have been no studies to prove a benefit of such modification in canine or feline IBD.
Prebiotics and probiotics
The modulation of the enteric flora with probiotics or prebi- otics included in the diet may have benefits in targeting the pathogenesis of IBD. Prebiotics are substrates selectively used by a limited number of beneficial bacterial species, resulting in alterations in the luminal microflora. Non-digestible carbohydrates, such as lactulose, inulin, fructo-oligosaccharides (FOS), and mannanoligosaccharides are the most frequently used prebiotic agents.
A probiotic is an orally-administered living organism that exerts health benefits beyond those of basic nutrition.35 Probiotics can directly antagonize pathogenic bacteria, but they also modulate mucosal immune responses, by stimulating either innate, phagocytic activity or a specific secretory IgA immune response.36 At present, the most appropriate organisms to select are unknown, but are likely to vary between host species.
Vitamin supplementation
Folate malabsorption may accompany severe and prolonged IBD, and oral supplementation is easily achieved, with administration of approximately 1 mg folic acid per day.
Malabsorption of cobalamin is more common than that of folate in patients with IBD, and can have significant metabolic consequences. Cobalamin deficiency causes methylmalonic acidemia, which may, in part, cause the ill-thrift and poor appetite seen in many patients. In addition, experimental cobalamin deficiency causes intestinal mucosal pathology, and it seems logical that correction of a deficiency is necessary before an optimal response to therapy can be achieved. There are a number of anecdotal reports, particularly in cats, where significant improvement was only seen after cobalamin supplementation. Oral administration of vitamin B12 is ineffective and it must be given by parenteral injection. Weekly subcutaneous injections of between 250 μg (cats and small dogs) to 1 mg (large breed dogs) are given for 6 weeks, then every other week for 6 weeks, and another dose after a month. Serum cobalamin concentration is rechecked a month after the last dose and should be supranormal at that time, indicating that cobalamin supplementation can be discontinued. If serum cobalamin concentration is only within the reference range, or even subnormal, cobalamin supplementation should be continued.
Table 9.7: Criteria for assessment of the canine inflammatory bowel disease activity index (CIBDAI), as proposed by Jergens et al (2003)32
A. Attitude/activity
0 = normal
1 = slightly decreased
2 = moderately decreased
3 = severely decreased
B. Appetite
0 = normal
1 = slightly decreased
2 = moderately decreased
3 = severely decreased
C. Vomiting
0 = none
1 = mild (1 episode/week)
2 = moderate (2-3 episodes/week)
3 = severe (>3 episodes/week)
D. Stool consistency
0 = normal
1 = slightly soft feces or fecal blood, mucus, or both
2 = very soft feces
3 = watery diarrhea
E. Stool frequency
0 = normal
1 = slightly increased (2-3 times/day)
2 = moderately increased (4-5 times/day)
3 = severely increased (>5 times/day)
F. Weight loss
0 = none
1 = mild (10% loss)
The scores for each of the six variables are added and a CIBDAI assigned as follows:
0-3 = clinically insignificant disease
4-5 = mild IBD
6-8 = moderate IBD
9 or greater = severe IBD
Antibacterial therapy
The use of antimicrobials in patients with IBD is justified, in part, by the potential to treat any undiagnosed enteropathogens or secondary SI bacterial overgrowth, and in part by the perceived importance of bacterial antigens in the pathogenesis of IBD (see above). In the authors’ experience, metronidazole is the preferred antibacterial for small animals. Its efficacy may not just be related to its antibacterial activity, since there may be immunomodulatory effects on cell-mediated immunity. Other authors prefer other antibacterials, such as oxytetracycline and tylosin, that may also have immunomodulatory effects and have some efficacy in canine IBD. There have been recent reports that HUC in Boxers (see 9.2.9) is responsive to enrofloxacin.37,38 This raises the possibility that this condition is not a variant of idiopathic IBD, but the consequence of a specific infection.
5-Aminosalicylic acid derivatives
Colitis can be treated with derivatives of 5-aminosalicylic acid (5-ASA) administered in a form that is only active in the colon, as long as the colitis is neither secondary to SI disease nor part of generalized IBD. Native 5-ASA is termed mesalazine, and slow-release enteric formulations are available for human patients. Premature release in the SI is likely to cause absorption and nephrotoxicity, but at the intraluminal pH in humans the majority of the 5-ASA is released in the colon. The safety of oral formulations of mesalazine in dogs and cats is unclear and they cannot be recommended for routine use. Mesalazine enemas and suppositories are safe, but not popular.
Sulfasalazine is the most commonly used preparation and is used at dosages of 10-30 mg/kg PO q 8-12 h in dogs and 10-20 mg/kg PO q 24 h in cats. It is a pro-drug with a diazo bond binding sulfapyridine to 5-ASA, which is cleaved by colonic bacteria to release free 5-ASA that acts locally in high concentrations in the colon as an anti-inflammatory agent. Hepatotoxicity can occur, but its major side-effect is keratoconjunctivitis sicca (KCS), and Schirmer tear tests should be performed on a regular basis. KCS is believed to be a complication of the sulfonamide-moiety, although it has also been seen with olsalazine, which contains no sulfonamide-moiety.
Olsalazine is a compound containing two 5-ASA molecules joined by a diazo bond. Again, free 5-ASA is released by colonic bacteria. Olsalazine was developed in an attempt to reduce the frequency of KCS, although occasional KCS is still reported with this drug. The dose is one half the dose of sulfasalazine as it contains twice the amount of active ingredient. Balsalazide is the newest pro-drug (4-aminobenzoyl-β- alanine-mesalamine), and is activated by the same mechanism as sulfasalazine, but its safety and efficacy have not been evaluated in small animals.
Immunosuppressive drugs
Undoubtedly, the most important therapy for idiopathic IBD is immunosuppression, although it should only be considered as a last resort. In human IBD, glucocorticoids and thiopurines (azathioprine, 6-mercaptopurine, etc.) are used most widely.39
Traditional glucocorticoid therapy
In dogs and cats, glucocorticoids are used most frequently, and prednisolone (or more commonly prednisone in the USA) is the drug of choice. Dexamethasone should probably be avoided since it has been shown to have a deleterious effect on entero- cyte brush border enzyme expression in other species. In severe IBD, when oral absorption may be inadequate, prednisolone can be administered parenterally. The standard initial dosage of 12 mg/kg PO q 12 h, is given for 2 to 4 weeks, and then tapered slowly over the subsequent months. In most cases, the therapy can only be reduced to a low maintenance dose given q 48 h, but in the minority of cases it can be completely withdrawn.
In some cases, an initial response to steroids is followed by a relapse and lack of further response, even when the dosages are increased. Some of these cases probably represent either transformation to lymphoma, or an incorrect initial diagnosis. However, resistance to steroids may perhaps develop because of induction of the multiple drug resistance gene and expression of P glycoprotein.
Novel glucocorticoid therapy
When the highest glucocorticoid dose is administered, signs of iatrogenic hyperadrenocorticism (polyphagia, polydipsia / polyuria, pot-bellied appearance, and /or muscle wastage) are commonly observed, especially in dogs. However, most of these signs are transient and resolve as the dosage is reduced. If a relapse consistently occurs when the dosage is reduced, alternative drugs can be added to provide a “steroid-sparing” effect (see below). Alternatively, novel steroids with fewer side effects can be used.
An enteric-coated formulation of budesonide, a locally active steroid, has been used successfully in maintaining remission in human patients with IBD with minimal hypothalamic-pituitary-adrenal suppression, as 90% of the drug is metabolized during its first-pass through the liver after absorption. A preliminary study has shown an apparent efficacy of budesonide in dogs and cats with IBD, but limited information on the use of this drug is available.40 Anecdotally, oral doses no greater than 3 mg/day in dogs and 1 mg/day in cats, or 1 mg/m2/day have been recommended. However, induction ofALP and development of a steroid hepatopathy have been seen, and hypothalamic-pituitary-adrenal suppression has been demon
strated in dogs.41 Furthermore, the optimal dose of this drug has not yet been determined.
Azathioprine
Azathioprine at 2 mg/kg PO q 24 h is commonly used in dogs, in combination with prednisolone /prednisone, when the initial response to steroid therapy is poor or the side effects are marked and a steroid-sparing drug is required. However, its activity may show a delayed onset (up to 3 weeks) and, given its myelosuppressive potential, regular monitoring of the hemogram is necessary. Idiosyncratic bone marrow toxicity has been linked to the activity of the enzyme thiopurine methyltransferase (TPMT), the major enzyme involved in the degradation of 6-mercaptopurine (6MP), the active metabolite of azathioprine. However, there are other pathways of 6MP metabolism, and the correlation between toxicity and TPMT activity is not clear.42 Azathioprine is not recommended for cats, partly because cats have very low activities of TPMT, and partly because the coated tablets cannot be split and need reformulation to a suitable size.
Other cytotoxic agents
Chlorambucil (2-6 mg/m2 PO q 24 h until remission, then tapering) is a better choice of a cytotoxic immunosuppressive agent in cats. Other immunosuppressive cytotoxic drugs include methotrexate, cyclophosphamide, and cyclosporine (ciclosporin). Methotrexate is effective in the treatment of human CD, but it is not widely used in companion animals.43 In dogs it often causes diarrhea when used for the treatment of lymphoma, but it is better tolerated in cats. Cyclophosphamide has few advantages over azathioprine and is rarely used. However, cyclosporine therapy may show promise for the future, given its T-lymphocyte specific effects and efficacy in canine anal furunculosis.44,45 Unfortunately, it is expensive. Preliminary studies in dogs with IBD have shown variable efficacy (E. Hall, personal observation 2005).46
Novel therapies
New drugs are being used increasingly for human IBD patients, in an attempt to target the underlying pathogenetic mecha- nisms.47 Novel immunosuppressive drugs, monoclonal antibody therapy, cytokines, transcription factors, and dietary manipulation are being trialed in human IBD patients (Table 9.8) and may be suitable for small animals with IBD in the future.
Mycophenolate mofetil has been used to treat human IBD, although its efficacy is variable.48 Drugs that target TNF-α, (e. g., thalidomide and oxpentifylline) may be suitable for the treatment of canine IBD, because of the importance of this
Table 9.8: Novel therapies for human IBD10
| Drug therapy | Proposed mechanism of action |
| Anti-rejection drugs | |
| Tacrolimus | Immunosuppressant macrolide |
| Mycophenolate | Inhibits lymphocyte proliferation, decreases IFN-γ production |
| Leukotriene antagonist | |
| Zileuton | Orally active inhibitor of 5-lipoxygenase |
| Thromoboxane synthesis inhibitors | |
| Ridogrel | Inhibits thromboxane A2 synthase |
| Picotamide | Inhibits thromboxane A2 synthase and antagonizes TxA2 receptors. |
| Inhibitors of TNF-α expression Oxpentifylline | Inhibits TNF-α expression |
| Thalidomide | Inhibits TNF-α and IL-12 expression, reduces leukocyte migration, impairs angiogenesis |
| Bone marrow and stem cell transplantation | |
| Bone marrow grafts | Unknown; possibly immunomodulation |
| Cytokine manipulation Systemic IL-10 therapy | Down-modulatory cytokine |
| IL-10 production by genetically engineered probiotic | Down-modulatory cytokine |
| Anti-IL-2 monoclonal antibody (MAb) | Counteracts pro-inflammatory effects |
| Anti-IL-2R (CD25) MAb | Inhibits IL-2 effects |
| Anti-IL-12 MAb | Counteracts pro-inflammatory effects |
| Anti-IL-11 MAb | Down-regulates TNF-α and IL-1β |
| Recombinant IFN-α therapy | Anti-inflammatory, antiviral? |
| Anti-IFN-γ MAb | Immunomodulatory effect on Th1 cells |
| Anti-TNF-α MAb | Counteracts pro-inflammatory effects, induces inflammatory cell apoptosis |
| Manipulation of endothelial cell adhesion molecules | |
| ICAM-1 (antisense oligonucleotide) | Reduces immune cell trafficking |
| Anti-α4β7 MAb | Reduces immune cell trafficking |
| Transcription factor blockade NF-κB anti-sense oligonucleotide | Inhibits pro-inflammatory cytokine expression |
| ICAM-1 antisense oligonucleotide | Reduces immune cell trafficking |
| Other immune system modulations | |
| Anti-CD4 antibodies | Immunomodulation |
| Intravenous immunoglobulin | Saturates Fc receptors; possibly other mechanisms |
| T-cell apheresis | Immunomodulation |
| Verapamil | Inhibitor of P-glycoprotein (P-gp) and may reduce IL-2 production and T-lymphocyte proliferation |
cytokine in disease pathogenesis. However, anti TNF-α monoclonal antibody therapy will only be suitable for canine and feline IBD if species-specific monoclonal antibodies can be made available.49-51
While some of these newer therapies hold promise for the future, the current treatment of idiopathic IBD in dogs and cats remains based on immunosuppression and its prognosis remains guarded.
9.2.6