constipation and Dyschezia
Constipation is a clinical sign characterized by absent, infrequent, or difficult defecation associated with retention of feces within the colon and rectum.When feces are retained in the colon for a prolonged period of time, the mucosa continues to absorb water from the fecal mass, which gradually results in impacted feces that become progressively harder and drier.
Obstipation is a condition of intractable constipation in which the colon and rectum become so impacted with excessively hard feces that defecation cannot occur. Megacolon is a term that refers to a disorder (not a sign) in which the colon becomes extremely dilated and hypo- motile, usually irreversibly so, and it is an important cause of chronic constipation/obstipation in cats.Dyschezia, a clinical sign often associated with constipation, is defined as difficult or painful evacuation of feces from the rectum and is usually associated with lesions in or near the anal region. Tenesmus is a clinical sign characterized by ineffective or painful straining to defecate; thus it usually accompanies dyschezia.
Etiology
Underlying causes or predisposing factors for constipation are listed in Table 8-3 and include (1) ingested foreign material, (2) environmental factors, (3) painful anorectal or orthopedic conditions, (4) anorectal or colonic obstruction, (5) neuromuscular diseases, (6) fluid and electrolyte disturbances, and (7) drug-related effects.
Ingested foreign material such as indigestible fibrous material (especially hair in cats from their grooming behavior) or abrasives (especially bones in dogs) may become incorporated into the fecal mass and result in the formation of hard fecal impactions that are difficult or painful to evacuate from the colon.
Environmental factors that are not conducive to defecation or that vary from the daily routine to which the patient is accustomed may cause the patient to inhibit the urge to defecate, leading to constipation.
This occurs, for example, when a patient is placed in strange surroundings such as a kennel or veterinary hospital or when the patient's daily outdoor exercise routine is changed. Indoor cats will often suppress the urge to defecate when their litter box is too dirty or there is territorial competition with other cats in the household.Painful defecation caused by anorectal diseases (e.g., anal sacculitis or perianal fistulae; see section on anorectal disease) or by orthopedic disorders that limit positioning for defecation (e.g., disorders of pelvis, spine, or hips) can result in voluntary inhibition of defecation and lead to constipation.
Rectocolonic obstructions that mechanically impede passage of feces may occur from intraluminal causes, such as foreign bodies, perineal hernia, or stenosing neoplastic or inflammatory lesions (i.e., strictures), and from extraluminal causes, such as prostatic enlargement, paraprostatic cysts, compressive pelvic fractures, perianal tumors, or pseudoco- prostasis (feces matted to the hair of the perianal area).
Neuromuscular disorders may lead to constipation by interfering with colonic innervation, colonic smooth muscle function, or simply the ability of the patient to assume the normal defecation stance—for example, disease or injury of the lumbosacral spinal cord (e.g., canine intervertebral disk disease), spinal deformity (as occurs in Manx cats), endocrine disease (hypothyroidism), or dysautono- mia, a progressively fatal autonomic polyneuropathy of young cats. When innervation of the anus is also impaired, fecal incontinence may be an associated clinical sign. The pathogenesis of idiopathic megacolon appears to involve smooth muscle dysfunction. Studies have demonstrated decreased
Classification and Causes of Constipation
| Classification | Cause |
| Dietary | Ingested foreign material mixed with feces (hair, bones, cloth, garbage, cat litter, rocks, plant material, etc.) Inadequate water intake |
| Environmental/psychologic | Dirty litter box Prolonged inactivity Confinement (hospitalization, boarding) Change in habitat or daily routine |
| Painful defecation | Anorectal disorders Anal sac impaction, infection, or abscess Anorectal stricture, tumor, or foreign body Myiasis Perianal fistulae Perianal bite wound cellulitis or abscess Pseudocoprostasis Orthopedic disorders Spinal disease or injury Injuries of the pelvis, hip joints, or pelvic limbs |
| Rectocolonic obstruction | Extramural Prostatic hypertrophy, prostatitis, abscess, or tumor Paraprostatic cyst Pelvic fracture (malunion) Pelvic collapse due to nutritional bone disease Perianal tumor Pseudocoprostasis Intramural or intraluminal Rectocolonic stricture, tumor, foreign body, or fecolith Rectal diverticulum or perineal hernia |
| Neuromuscular dysfunction | Lumbosacral spinal cord disease (injury, deformity, degeneration, neoplasia) Bilateral pelvic nerve injury Dysautonomia (Key-Gaskell syndrome) Hypothyroidism Idiopathic megacolon |
| Fluid and electrolyte abnormalities | Dehydration (e.g., chronic renal failure) Hypokalemia Hypercalcemia (hyperparathyroidism) |
| Drug-induced | Anticholinergics Adrenergic blockers Calcium channel blockers Phenothiazines and benzodiazepines Opiates and opioids Diuretics Antihistamines Aluminum hydroxide antacids Sucralfate Kaolin-pectin Barium sulfate Iron Laxatives (chronic overuse) |
active contraction (in vitro) of smooth muscle from cats with megacolon in response to neurotransmitters (acetylcholine, substance P, cholecystokinin), membrane depolarization (potassium), and electrical stimulation.
Innervation of the colon, however, appears to be normal in these cats.Fluid and electrolyte disorders may predispose to constipation, particularly dehydration, which can cause the feces to become excessively dry and hard, and hypokalemia or hypercalcemia, either of which can affect colonic smooth muscle function. A combination of these may explain the frequent constipation seen in chronic renal failure, especially in cats.
Drug-induced constipation may occur as a side effect of motility-modifying drugs (anticholinergics, opiates, opioids), antihistamines, barium sulfate, aluminum hydroxide, and diuretics.
Clinical Signs
Constipated patients are usually presented for failure to defecate over a period of days. The owner may notice tenesmus or frequent attempts to defecate with little or no passage of feces. Other signs may include anorexia, lethargy, vomiting, dehydration, and hunched-up appearance caused by abdominal discomfort. Dyschezia usually indicates anorectal disease (see section on anorectal disease). The patient first may cry out as it attempts to defecate, usually with straining (tenesmus) during the attempt, then it ceases the effort, walks around anxiously, and repeatedly tries again. Mucosal irritation caused by impacted feces may provoke a secretion of fluid and mucus that bypasses the retained fecal mass and is expelled paradoxically as diarrhea during attempts to defecate. Constipation tends to be a recurrent problem in some patients.
Megacolon mostly occurs in middle-age cats (mean age of 5.8 years in one case survey). The same study found a predilection in male cats (70%) over females (30%). The most frequently affected breeds were domestic short hair (46% of cases), domestic long hair (15%), and Siamese (12%). Megacolon in most cats is idiopathic; however, irreversible colonic dilation can also be caused by persistent mechanical obstruction (e.g., pelvic canal stenosis caused by malunion, anorectal stricture, anorectal neoplasia) or neuromuscular dysfunction caused by lumbosacral spinal cord disease.
Diagnosis
Constipation is generally established as a problem from the history and confirmed by rectal and abdominal palpation of a colon distended with hard feces. The goal of diagnosis is to identify predisposing factors (see Table 8-3). The owner should be carefully questioned to identify any of the potential dietary, environmental, behavioral, psychologic, or medication-related factors or predispositions listed in Table 8-3 that might be involved.
Physical examination may also reveal the cause or predisposition for constipation. Digital anorectal examination should be performed to detect painful or obstructive lesions of the anorectal area and pelvic canal (sedation may be required). The rear limbs, coxofemoral joints, pelvis, and lumbosacral spine should be evaluated for orthopedic problems that could cause either painful defecation or difficulty for the patient to maneuver into the defecation stance. In addition, a neurologic examination with emphasis on candal spinal cord function should be performed to identify neurologic causes of constipation. In cats with constipation due to dysautonomia (Key-Gaskell syndrome), additional manifestations of progressive autonomic failure that may be seen include uri- nary/fecal incontinence, megaesophagus, bradycardia, mydriasis, decreased lacrimation, and prolapse of the nictitating membranes.
A routine serum biochemistry profile, urinalysis, and CBC should be evaluated in patients with recurrent constipation or signs indicating the potential for underlying systemic conditions (e.g., chronic renal failure) that could cause dehydration and electrolyte disturbances. These laboratory evaluations are also helpful in patients that are severely constipated or obstipated, especially those that are vomiting or markedly depressed, to detect the metabolic consequences of prolonged fecal retention (e.g., fluid and electrolyte imbalances, endotoxemia, azotemia) and to guide supportive treatment. Thyroid function should be evaluated in dogs with recurrent constipation and other signs compatible with hypothyroidism.
Abdominal radiography can be used in the constipated patient to identify the following: (1) extent of colonic impaction with densely packed feces; (2) extreme dilation of the colon that would indicate megacolon; (3) radiopaque foreign material (e.g., bone chips) in the retained feces that would indicate a dietary cause of constipation; (4) pelvic, coxofemoral, or spinal lesions that may be predisposing causes of constipation; and (5) enlargement of the prostate that may be an underlying cause of constipation.
Additional specialized diagnostic studies may be indicated in selected patients. When intraluminal obstructive lesions are suspected, barium enema contrast radiography (see Chapter 2) or colonoscopy (see Chapter 3) may be used after the retained feces have been evacuated to evaluate the lumen of the colon. Myelographic and electrodiagnostic evaluations of the lumbosacral spinal cord and spinal nerves should be considered in patients with evidence of impaired anorectal innervation. When prostatic disease or paraprostatic cysts are suspected to be the cause of constipation, further evaluations might include caudal abdominal ultrasound examination, contrast cystourethrography, and cytology/culture studies of the prostate. Computed tomography (CT) and magnetic resonance imaging (MRI) scans can be useful for imaging pelvic canal structures and the lumbosacral spine.
Treatment
Mild constipation resolves spontaneously or is treated on an outpatient basis by dietary adjustment and oral or suppository laxatives. Severe constipation is treated initially by evacuation of impacted feces from the colon by means of enemas and/or manual extraction along with correction of complicating dehydration and electrolyte imbalances. Follow-up therapy is aimed at eliminating or controlling any of the underlying causes of constipation that are identified from Table 8-3 and at preventing recurrences by means of dietary adjustments and laxative therapy (Table 8-4). Surgical correction is required for obstructing neoplasms and strictures and many anorectal disorders.
Finally, long-term management of megacolon or
| MABSEkSM Treatments for Constipation** | ||
| Treatment | Product (Manufacturer) | Dosage |
| Oral Cathartics Bulk-Forming Laxatives | ||
| Coarse bran | All-Bran (Kellogg’s) and others | 1-5 tbsp daily with food |
| Canned pumpkin | Pie filling (Libby’s) | 1-5 tbsp daily with food |
| Psyllium | Metamucil (Procter & Gamble); Fiberall (CIBA) | 1-3 tbsp daily with food |
| Lubricant Laxatives | ||
| White petrolatum | Laxatone (Evsco) | 1-5 ml daily PO |
| Emollient Laxatives | ||
| Docusate sodium | Colace (Shire) | Dog: 50-200 mg daily PO Cat: 50 mg daily PO |
| Docusate calcium | Surfak (Geneva) | Dog: 100-240 mg daily PO Cat: 50-100 mg daily PO |
| Saline Laxatives | ||
| Magnesium hydroxide | Phillips’ Milk of Magnesia (Glenbrook) | Dog: 2-8 tablets daily PO |
| Osmotic Laxatives | ||
| Lactose | Milk | Add to diet to effect |
| Lactulose | Duphalac (Reid Rowell); Cephulac (Merrell Dow) | 0.25-0.5 ml/lb PO, q8-12h |
| Polyethylene glycol and | Colyte (Schwarz); Golytely (Braintree) | 12-20 ml/lb PO repeated |
| electrolytes* | in 2-4h (for bowel prep) | |
| Stimulant Laxatives | ||
| Bisacodyl | Dulcolax (Boehringer Ingelheim) | Dog: 5-20 mg daily PO Cat: 5 mg daily PO |
Continued
*Ancillary treatment measures:
1. Regular grooming to prevent ingestion of loose hair (especially cats).
2. Prevent ingestion of abrasive foreign materials.
3. Provide fresh drinking water.
4. Provide clean litter for cats.
5. Encourage regular exercise.
Tor severe recurrent or refractory cases: total or subtotal colectomy. *Used mainly to prepare the colon for radiography or endoscopy. §Should not be used in cats or small dogs.
recurrent obstipation that is unresponsive to medical therapy in the cat may involve colectomy surgery.
Initial Relief of Constipation
Simple constipation with mild to moderate impaction of feces and without accompanying systemic signs (depression, vomiting, dehydration) can often be managed on an outpatient basis using dietary adjustment, measures to increase water intake, and oral laxatives. Oral laxatives can be prescribed as discussed later in this chapter and the animal reevaluated in 48 hours. To promote initial evacuation of the distal colon when impaction is not severe, one to three pediatric suppositories consisting of docusate sodium, bisacodyl, or glycerin also can be used or a therapeutic enema can be administered.
In severe constipation/obstipation, fluid and electrolyte balance should initially be restored parenterally. The colon is then evacuated manually under general anesthesia with a combination of colonic irrigation with warm isotonic saline as an enema solution to soften the impacted feces and extraction of retained fecal masses by gentle transabdominal manipulation to milk the feces into the distal rectum for digital extraction or removal with sponge or whelping forceps. To avoid excessive bowel trauma in patients with extensive fecal impaction, it may be advisable to evacuate the colon manually in stages over a period of 2 to 3 days.
Enema Solutions
Enema solutions can be used to soften hard, impacted feces and promote evacuation. The enema solutions should be warmed prior to instillation, and the calculated dose administered slowly so as not to induce vomiting. The following are commonly used enema solutions:
1. Warm isotonic saline or tap water (2.5 to 5 ml/lb body weight), with or without the addition of a mild soap to stimulate defecation by an irritant effect (soap must not contain hexachlorophene because of its neurotoxicity if absorbed).
2. Docusate as an emollient (5 to 10 ml in cats and small dogs; 10 to 20 ml in medium-sized dogs; 20 to 30 ml in large dogs).
3. Mineral oil as a lubricant (5 to 10 ml in cats and small dogs; 10 to 20 ml in medium-sized dogs; 20 to 30 ml in large dogs).
4. Sodium phosphate solution (Fleet Children’s Enema), which has softening, bulk-producing, and irritant effects (use only in medium-sized or large dogs with normal renal function; not safe for use in cats or small dogs).
Mineral oil and docusate should not be mixed because docusate promotes mucosal absorption of mineral oil, and mineral oil coats the feces, reducing the emollient effect of docusate. Sodium phosphate enemas must never be used in cats and small dogs because they can cause dangerous hypernatremia, hyperosmolality, hyperphosphatemia, and hypocalcemia.
Measures to Prevent Recurrence of Constipation
Following evacuation of retained feces from the colon, measures are instituted to prevent and control recurrences of constipation. If underlying causes or predisposing factors (see Table 8-3) can be identified, they should be eliminated or corrected if at all possible. For example, ingestion of potential abrasive materials such as bones should be prevented. In cats, if hair ingestion is a potential contributing factor, the owner should be instructed to adopt a routine of regular grooming to remove loose hair from the cat’s hair coat before it can be ingested. A daily routine of exercise and frequent opportunities to defecate should be provided for dogs, and clean litter should be provided at all times for cats, to encourage regular defecation. Water intake should be encouraged by providing access to fresh water at all times. The use of any medications that promote constipation should be adjusted or discontinued. Predisposing prostatic, endocrine (e.g., thyroid), spinal, or orthopedic disorders should be treated. Whenever possible, painful or obstructing anorectal lesions (see section on anorectal diseases) should be corrected, even surgically if necessary.
Oral Laxatives
Oral laxative medications and dietary supplements can be prescribed as needed for control of constipation (see Table 8-4). Laxatives act through interrelated effects on both intestinal mucosal fluid transport and colonic motility and are classified by their properties and mechanisms of actions as (1) bulk-forming, (2) lubricant, (3) emollient, (4) osmotic, and (5) stimulant. The use of an oral laxative often needs to be individualized by adjusting the dose until the desired frequency of defecation and fecal consistency are obtained.
High-Fiber Bulk-Forming Laxatives. These should be added to the food to promote soft feces and normal colonic motility as the initial approach for prevention and control of constipation. Bulkforming agents consist of indigestible polysaccharides and cellulose that exhibit hydrophilic properties within the bowel. Insoluble fiber is derived principally from wheat bran or psyllium seed coat. Beneficial effects include increased fecal water content, increased fecal weight and frequency, softer fecal consistency, decreased intestinal transit time, and reduction of the intracolonic pressure required for normal defecation. Adequate water intake and patient hydration are required for these beneficial actions and to prevent impaction of fiber in the colon. For long-term control of constipation, a commercially prepared high-fiber diet can be fed, or the regular diet can be supplemented with unprocessed wheat bran, oat bran, or pumpkin (1 to 5 tbsp per meal) or commercial sources of psyllium (Metamucil or Fiberall, 1 to 5 tsp per meal). Dietary adjustments alone are not usually sufficient to control constipation in cats with megacolon.
Lubricant Laxatives. Mineral oil and flavored white petrolatum products can be used to soften and lubricate the feces to facilitate evacuation. These should be administered between meals so that they do not interfere with the absorption of fat-soluble vitamins. Mineral oil should be used only in enema form. Oral administration should be avoided because of the risk of aspiration lipid pneumonia.
Emollient Laxatives. Docusate sodium available in enema and oral forms (Colace), and docusate calcium (Surfak) are mild laxatives that promote water penetration into the feces, thereby softening the feces. Although relatively inert, docusate may increase intestinal loss of fluid; thus its use should be avoided in the presence of dehydration. For the reasons mentioned previously (see section on enema solutions), docusate and mineral oil should not be mixed.
Osmotic Laxatives. These consist of poorly absorbed disaccharides (such as lactose or lactulose), ions (such as magnesium hydroxide, magnesium citrate), or inert osmotic agents (polyethylene glycol) that osmotically retain water in the bowel lumen to produce soft or fluid feces. A mild osmotic laxative effect can be produced in some patients by the addition of milk (lactose) to the diet in a quantity that exceeds the digestive capacity of small intestinal lactase. The nonabsorbable disaccharide lactulose (Duphalac, Cephulac, 0.25 to 0.5 ml/lb orally three times a day) is an excellent choice as a safe and effective all-purpose laxative for short- or long-term use in both dogs and cats. Unabsorbed dissacharides such as lactulose are fermented by colonic bacteria to lactic acid and other organic anions, thereby producing an osmotic catharsis and acidification of the colon. The dosage of lactulose needs to be adjusted to effect. If the dosage is too high, abdominal discomfort, flatulence, and diarrhea may occur. These side effects resolve with lowering the dosage.
Magnesium hydroxide is available as an over- the-counter drug (Phillips' Milk of Magnesia). Magnesium is contraindicated in renal failure. Magnesium citrate and polyethylene glycol— electrolyte solutions (Colyte, GoLYTELY) are available commercially for preparation of the colon for endoscopy, but the large oral doses required are too impractical for therapeutic use.
Stimulant Laxatives. These increase propulsive motility of the bowel by a variety of mechanisms. They are generally contraindicated in the presence of an obstructive lesion and are less appropriate for long-term use than other categories of laxatives. A useful stimulant laxative for the dog and cat is bisacodyl (Dulcolax, daily dose of 5 mg for cats and small dogs, 10 mg for medium-sized dogs, and 15 to 20 mg for large dogs), which works by stimulating colonic smooth muscle and the myenteric plexus. Although beneficial on a short-term basis in conjunction with measures to soften the feces, long-term use of bisacodyl may damage the myenteric plexus. Castor oil, another stimulant laxative, is hydrolyzed in the intestines to ricinoleic acid, which stimulates colonic motility and secretion. Castor oil is not very useful for outpatient treatment because of poor patient acceptance, but it can be used effectively in hospitalized patients to prepare the bowel for radiographic or endoscopic procedures.
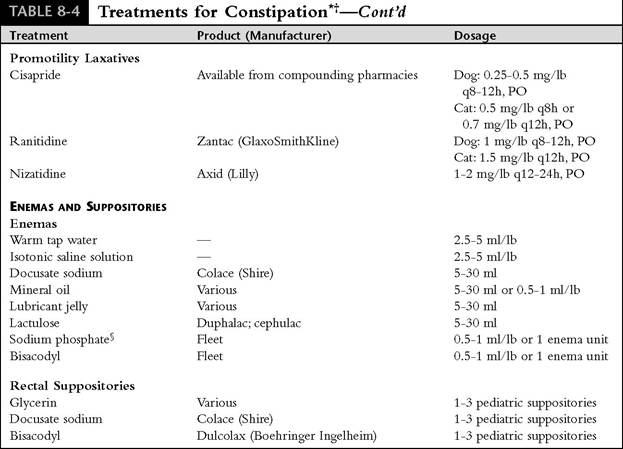
Promotility Therapy. Cisapride (Propulsid) is a benzamide derivative that promotes GI motility by stimulating colonic smooth muscle, increasing the physiologic release of acetylcholine from postganglionic nerve endings of the myenteric plexus, and acting as a 5-HT4-serotonergic agonist. These actions lead to improved propulsive motor activity of the esophagus, the stomach, and the small and large intestines. Cisapride is a highly effective laxative for both cats (0.5 mg/lb every 8 hours or 0.7 mg/lb every 12 hours orally) and dogs (0.25 to 0.5 mg/lb every 8 to 12 hours orally) (see Table 8-4). It can be administered alone or combined with stool-softening measures such as a fiber- augmented diet or lactulose. Cisapride is the most effective medical therapy for megacolon in cats. The colon in cats with megacolon may even resume normal diameter radiographically under treatment with cisapride. Unfortunately, megacolon commonly becomes refractory to cisapride after several months of therapy, necessitating increasing the dosage to 1 mg/lb every 8 hours or higher. Eventually after several months to years, many cats with megacolon become completely refractory to cisapride and require colectomy.
Cisapride is contraindicated in the presence of GI obstruction or perforation. It is ineffective if used with anticholinergics. Side effects are uncommon, but nausea, vomiting, diarrhea, flatulence, and abdominal discomfort are occasionally reported. Cisapride appears very safe for long-term use in animals; however, it is no longer approved for use in humans in the United States because of its association with serious arrhythmias. This side effect has not been a problem in animals. Cisapride can be obtained in the United States from compounding pharmacies for animal use.
Ranitidine (Zantac) and nizatidine (Axid) are H2-receptor antagonists that also stimulate GI and colonic motility at standard dosages (see Table 8-4). They increase acetylcholine by inhibiting synaptic acetylcholinesterase. These are not as potent as cisapride as promotility agents; however, they may be useful when a mild laxative effect is needed.
Colectomy
For megacolon and severe recurrent constipa- tion/obstipation that is unresponsive to medical management, especially in cats, subtotal colectomy is the most effective method of treatment. This procedure involves the removal of 95% or more of the colon. In cats with obstipation from pelvic fracture malunion, pelvic osteotomy or reconstructive surgery can allow return of normal colonic function if obstipation has been a problem for less than 6 months; otherwise, subtotal colectomy is recommended. After subtotal colectomy, diarrhea and frequent defecation are common; however, bowel function gradually improves during the 2 to 4 weeks following surgery in most cats. In dogs, diarrhea, frequent defecation, hema- tochezia, and tenesmus often persist after colon removal.