Diagnosis
Hallmark clinical signs of vestibular disease include a head tilt, abnormal resting nystagmus, and vestibular ataxia. However, a complete neurological examination is necessary to be able to make a neurolocalization and appropriate list of differential diagnoses.
The first, critical step with vestibular disease is to distinguish a central from a peripheral lesion.Box 7.1
Differentiation of a central lesion from a peripheral lesion is the first critical step in determining the cause of vestibular symptoms
Diagnostic testing will give you the information necessary to make a more definitive diagnosis and appropriately determine prognosis. Watchful monitoring is really only a good option in the mildly affected patient. Medical management of the moderate to severely vestibular patient is labor intensive and difficult.
Diagnostic testing is of crucial importance in central vestibular cases. Once your list of differential diagnoses has been made, it is important to consider advanced imaging to determine prognosis. Magnetic resonance imaging (MRI) is the test of choice for diseases affecting the caudal fossa (brainstem and cerebellum). Computed tomography (CT) does not allow for good visualization of the brainstem and cerebellum due to artifact (beam hardening) from all the bone in the area. If you believe the disease to truly be peripheral, then CT is a very good test for visualization of the ear canals and tympanic bullae. If you have any concern that there may be central involvement, then MRI is your test of choice (Figure 7.1).
Peripheral Vestibular Structures
The peripheral vestibular structures include the receptors, the ganglion, and the peripheral axons of the vestibular portion of CN VIII. Dysfunction of the peripheral vestibular system can cause loss of balance, vestibular ataxia, head tilt toward the affected side,
Chronic Disease Managementfor Small Animals, First Edition.
Edited by W. Dunbar Gram, Rowan J. Milner and Remo Lobetti.© 2018 John Wiley & Sons, Inc. Published 2018 by John Wiley & Sons, Inc.
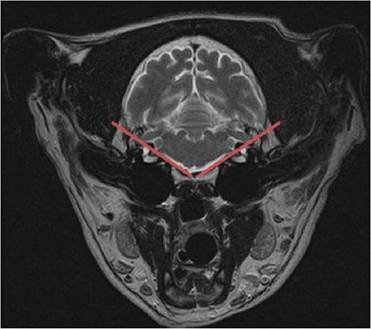
Figure 7.1 Magnetic resonance image of a brain with lines. Inside the lines is central vestibular (brainstem and cerebellum) while outside are peripheral vestibular structures (ear canals, tympanum, tympanic bulla and CN VIII).
horizontal or rotary nystagmus, and positional strabismus. Typically, dogs with peripheral vestibular dysfunction have more rapid nystagmus (>60 beats per second) than dogs with central disease. Both Horner's syndrome and facial nerve paralysis can be seen with peripheral vestibular disease as those nerves travel in the vicinity of the tympanic bulla.
Central Vestibular Structures
The central vestibular structures include the nuclei in the medulla of the brainstem and their projections to the cerebellum, spinal cord, and rostral brainstem. Animals with central vestibular dysfunction can show all the clinical signs of those with peripheral vestibular dysfunction as well as many others. Important findings to definitively localize a vestibular lesion as central are proprioceptive deficits and paresis (motor deficits) - if deficits are noted, the lesion is located centrally, in the brainstem. This is because the lesion is affecting those ascending sensory or descending motor tracts. However, the converse is not always true; a lack of proprioceptive deficits does not rule out a central lesion. Other signs, including vertical nystagmus, nystagmus for which the fast phase changes direction, cerebellar signs (hypermetria), altered mental status, spinal ataxia, dysme- tria, upper motor neuron paresis, intention tremors, and any cranial nerve deficit other than VII, are consistent with central vestibular disease.
Paradoxical Vestibular Disease
Paradoxical vestibular disease is always central! In this case, the head usually tilts away from the side of the lesion while all the other abnormalities (nystagmus, falling, proprioceptive deficits, hypermetria) are on the affected side.
The lists of differential diagnoses are vastly different for central and peripheral lesions, so it is very important to make this distinction. Generally speaking, peripheral diseases have a better prognosis and are easier to definitively diagnose than central disorders. Central vestibular disorders can have a more guarded prognosis and require more advanced and expensive diagnostic tests.
Box 7.2
Peripheral vestibular disorders tend to have a better prognosis and are easier to definitively diagnose than central disorders
Peripheral Vestibular Disease
Differentials include idiopathic geriatric ve stibular disease, otitis media/interna, inflammatory polyps, cholesteatomas, aural neoplasia, toxicosis, hypothyroidism, and polyneuropathy. Idiopathic geriatric vestibular disease, “old dog vestibular disease,” typically occurs in geriatric large breed dogs, though any breed can be affected.
A note about bilateral peripheral disease. There is the scenario where you have disease affecting both left and right inner ears. Because both receptors are nonfunctional, you lose ALL perception of gravity and movement. This means physiologic nystagmus is lost and animals' gait typically becomes very low, crouched and wide-based.
Central Vestibular Disease
Differentials include CNS neoplasia, inflammatory CNS disease, otogenic intracranial infections, trauma, toxicoses, vascular and infectious disease. Dogs with central vestibular lesions are more likely to be non-ambulatory than those with peripheral dysfunction. Primary CNS neoplasia typically has a chronic, progressive history, though metastatic lesions can have a peracute onset. Inflammatory, immune-mediated CNS disease is very common and mostly affects young to middle-aged small-breed terrier and toy breed dogs. Otogenic intracranial infections, expansion of otitis media/interna into the cranial vault, are rare. They typically occur in dogs with a history of chronic ear disease, though it is possible to have disease in the bulla without disease in the ear canals.
Metronidazole Toxicity
Metronidazole can cause central vestibular dysfunction at doses of 60mg∕kg∕day in as little as 3 days. The clinical signs will improve once the medication is discontinued, and diazepam at 1 mg/kg PO TID in dogs can be used to hasten recovery.
Diagnostic Conundrum
It's too vestibular to tell! Occasionally, the animal can be so severely affected, for example, alligator rolling, that you cannot determine if the lesion is central or peripheral. In this situation there are two choices: you can medically manage the patient for 24 hours and monitor for improvement or refer for workup. If this is a geriatric large-breed dog, the chances are good this is idiopathic geriatric vestibular disease and you will see improvement in 24-48 hours.