Diagnosis
Clinical evaluation and patient history are the first tools used for diagnosis. Sporotrichosis can be diagnosed by direct examination of tissue biopsies or lesion pus. Sporothrix from pus presents as gram-positive bacilliform corpuscles, phagocytized by giant and polymorphonuclear cells.
Typically, 10% potassium hydroxide is used for the observation of yeast in human tissue; however, the cells are small and sparse, making detection in direct examination difficult. By contrast, in samples from infected felines, yeast can be easily found due to the large fungal load in the lesions (Barros et al. 2011). Feline sporotrichosis is often diagnosed by cytological evaluation of samples collected from abscess aspirates. Advantages include convenience, low cost, and high sensitivity of the technique (Pereira et al. 2011; Sanchotene et al. 2015). In disseminated sporotrichosis, sputum, urine, blood, and cerebrospinal and synovial fluids samples can be used in the diagnosis.Isolation of the fungus is obtained after spreading clinical specimens on Sabouraud agar with chloramphenicol or cycloheximide. For species identification, dimorphism must be confirmed by the mycelium-yeast transition by subculturing the fungus on enriched media such as BHI agar at 37 °C for 5-7 days (Morris-Jones 2002). In 89% of cases, the fungus can be isolated in 8 days, but it may take up to 4 weeks.
In the typical histopathology of the disease, a mixed, granulomatous, and pyogenic inflammatory process can be observed, in which the characteristic structures are cigar-shaped or oval yeast cells (Fig. 10.9). Mycelium or asteroid bodies are not commonly observed in the tissue (Zhang et al. 2011). Asteroid bodies occur due to intense deposit formation in vivo of eosinophilic material around the microorganism, known as the Splendore-Hoeppli phenomenon. In sporotrichosis, asteroid bodies are characterized by the presence of radial, star-shaped deposition and are more frequent in lesions of humans with the lymphocutaneous form (Hussein 2008; Zhang et al.
2011). The origin of the events leading to the formation of asteroid bodies is not clear, but the deposition of antibodies and the incorporation of calcite and apatite crystals, which form the crystallized spicules, are known to occur. Moreover, the asteroid body serves as a resistance structure and plays an important role in fungus survival in the host (da Rosa et al. 2008).Noninvasive methods are available for diagnosis of sporotrichosis. Techniques using fluorescent antibodies or immunohistochemistry are quick but are not
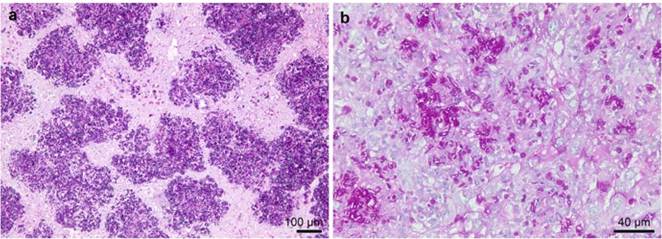
Fig. 10.9 (a) Histopathological aspects of Sporothrix brasiliensis during infection in a warmblooded host (murine model of infection; magnification of 10 x). (b) A mixed inflammatory process, granulomatous, with many cigar-shaped or oval yeast cells, is observed in the tissue (magnification of 40x). Staining: Schiff periodic acid
available in most laboratories (Davis 1996). Blumer et al. (1973) compared several serological methods, including latex agglutination, tube agglutination, complement fixation, immunodiffusion, and immunofluorescence, using crude fungal culture filtrate as the antigen. The latex agglutination technique was the most sensitive and specific, and immunodiffusion was also considered specific. However, Welsh and Dolan (1973) observed nonspecific reactions with the sera of normal individuals and heterologous sera using the agglutination technique.
The ELISA test has been extensively studied as a tool for sporotrichosis diagnosis and serologic follow-up of the patient. The antigens used include mycelium or yeastculture filtrates, as well as partially purified molecules. The literature shows that the tests have the same sensitivity and specificity, which range from 80 to 100% in humans (Almeida-Paes et al. 2007a; Almeida-Paes et al. 2007b; Bernardes- Engemann et al. 2005, 2009) and felines (Fernandes et al. 2011; Rodrigues et al.
2015b).Regarding the humoral immune response of patients with sporotrichosis, Scott and Muchmore (1989), using Western blot, observed that 100% of patient sera recognize the 40 and 70 kDa molecules and mostly also those of 22 and 36 kDa. However, Mendoza et al. (2002) reported that positive sera recognize additional molecules such as 40, 55, 74, 90, and 147 kDa, depending on the culture medium used for the production of the protein/glycoprotein extract. In contrast, in experimental murine sporotrichosis, antibodies recognize 67 kDa (Carlos et al. 1998) and 70 kDa molecules (Nascimento and Almeida 2005).
A well-known component of the Sporothrix cell wall is peptido-rhamnomannan. This glycopeptide or glycoconjugate is a complex of molecules with different molecular weights that are difficult to purify. The fraction of the peptido- rhamnomannan extract able to bind to concanavalin-A (ConA) has antigenic characteristics, and molecules of 84, 70, and 58 kDa were observed when probed with anti-S. schenckii rabbit serum (Lima and Bezerra 1997). This fraction was called SsCBF (S. schenckii ConA-binding fraction), and O-glycosylated chains of peptido-rhamnomannan from the cell wall are responsible for binding lectin ConA. In addition, this fraction was recognized by sera from patients with sporotrichosis when tested by ELISA, suggesting that the fraction SsCBF may be an important tool for the complementary and/or differential diagnosis of the mycosis (Bernardes- Engemann et al. 2005).
Another important antigen is gp60-70 (3-carboxymuconate cyclase), which is present in the culture filtrate. All BALB/c mice infected with S. schenckii were able to produce antibodies (IgG1 and IgG3) against this molecule in ELISA (Nascimento and Almeida 2005). This glycoprotein is also recognized by circulating IgG in 100% of cats with sporotrichosis in the main endemic areas of Brazil (Rodrigues et al. 2015b).
The study of antigenic molecules for diagnosis is important, and the use of antigens such as the cell-free antigen (CFA) preparation is simple and requires no special equipment.
Mycelial and yeast CFA preparations of S. brasiliensis have 14 and 23 reactive bands, respectively, against sera from immunized rabbits (Almeida-Paes et al. 2012). Antigens from yeast can be successfully used in the diagnosis of human sporotrichosis.The use of one type of antigen or another depends on the structure of each laboratory. The use of SsCBF allows for better test standardization because it is more specific; however, the culture filtrate is easier to produce because it does not require expensive equipment. The disadvantage lies in the production, which takes time and requires that strains, culture media, cultivation time, and preparation methods be standardized among laboratories.
Methods based on molecular biology are still scarce in the diagnosis of sporotrichosis. The regions of the ribosomal RNA gene can be used to establish phylogenetic relations among the different species. The ITS regions, which are the regions between the genes encoding the rRNA regions 18S, 5.8S, and 28S, are particularly useful for identifying S. brasiliensis, S. schenckii, S. globosa, and S. luriei (Zhou et al. 2014) using the primers ITS1 and ITS4 (White et al. 1990). Phylogenetic analysis based on protein-encoding genes such as beta-tubulin (de Meyer et al. 2008), calmodulin (Marimon et al. 2006, 2007), and elongation factor 1α (Rodrigues et al. 2013b) is also important for the molecular identification of etiological agents of human and animal sporotrichosis.
New techniques to identify the newly described species are in progress. Such methods include polymerase chain reaction (PCR) fingerprinting with the T3B oligonucleotide (de Oliveira et al. 2012) and PCR-restriction fragment length polymorphism (RFLP) with calmodulin amplification followed by digestion with the enzyme HhaI (Rodrigues et al. 2014b). A comparison of these techniques with analysis of the partial sequence of the calmodulin gene showed that both were able to identify the majority of the isolates studied and were very useful in the identification of isolates with atypical phenotype.
Only a few methods are available for the direct molecular diagnosis of sporotrichosis. Unlike the methods described above, these methods are sensitive and specific for the detection and identification of all Sporothrix species of clinical interest (Rodrigues et al. 2015a). For direct molecular diagnosis of complex samples
Table 10.1 Comparison of the different molecular methods for identification and/or detection of etiological agents of human and animal sporotrichosis
| Method | Samples | In silica analysisf | Time ID (h)g | Equipment11 | Reference | ||||
| Culturea | Biopsyb | Soile | Plantd | Fecese | |||||
| DNA sequencing | X | X | X | X | X | Yes | 10-12 | Thermocycler Electrophoresis system Sequencer | Marimon et al. (2007) |
| Amplified fragment length polymorphism (AFLP) | X | Yes | 10-12 | Thermocycler Sequencer | Neyra et al. (2005); Zhang et al. (2015) | ||||
| Random amplified polymorphic DNA (RAPD) | X | Yes | 6-7 | Thermocycler Electrophoresis system | de Oliveira et al. (2012) | ||||
| PCR-restriction fragment length polymorphism (PCR-RFLP) | X | No | 6-20 | Thermocycler Electrophoresis system | Rodrigues et al. (2014b) | ||||
| Species-specific PCR | X | X | X | X | X | No | 6 | Thermocycler Electrophoresis system | Rodrigues et al. (2015a) |
| Rolling circle amplification (RCA) | X | X | X | X | X | No | 5 | Thermocycler Electrophoresis system | Rodrigues et al. (2015e) |
| MALDI-ToF | X | Yes | 2 | Mass spectrometer | Oliveira et al. (2015) | ||||
aMaterial isolated in pure culture bClinical sample, fresh tissue ^Environmental soil sample dPlant debris or decaying organic matter eAnimal feces fBioinformatics of the generated data gAverage execution time in hours, ID identification hEquipment necessary to perform the method
218 A. M. Rodrigues et al.
(target plus exogenous DNA, e.g., host DNA), species-specific PCR is used for the selective detection of Sporothrix DNA using primer pairs for S. brasiliensis, S. schenckii, S. globosa, S. mexicana, S. pallida, and S. Stenoceras (Rodrigues et al. 2015a). Molecular diagnosis using species-specific PCR was validated using a murine model (BALB/c) of disseminated sporotrichosis. The infections caused by S. brasiliensis and S. schenckii were successfully detected in different organs such as the spleen, lungs, liver, kidneys, heart, brain, and tail using species-specific PCR (Rodrigues et al. 2015a). PCR was also useful for the detection of Sporothrix DNA in feces of infected animals, suggesting the use of species-specific PCR in ecoepidemiological studies (Rodrigues et al. 2015a).
The identification and specific detection of Sporothrix using rolling circle amplification (RCA) were recently proposed (Rodrigues et al. 2015e). Bioinformatics analysis revealed six candidate probes specific for S. brasiliensis, S. schenckii, S. globosa, S. luriei, S. mexicana, and S. pallida, with no significant homology to sequences of the genomes of humans, mice, or microorganisms outside members of Sporothrix. The accuracy of RCA was demonstrated in vitro by the binding specificity (probe DNA) in various isolates with no cross-reactivity and high detection sensitivity (up to 3 x 106 target copies). RCA-based identification is consistent with the phylogenetic analysis results of the major loci used in the S. schenckii complex, reinforcing the use of RCA as a reliable identification method alternative to DNA sequencing. The method also provides a powerful tool for the rapid and specific detection of clinically relevant Sporothrix in biopsies, soil, feces, and plant debris. Due to the robustness of RCA, the technique has potential for ecological studies (Rodrigues et al. 2015e).
In general, molecular methods may be useful for the diagnosis of sporotrichosis. A small amount of sample is typically required, and the method is sensitive and specific, taking less time than the traditional methods. Table 10.1 shows a comparative summary of the main methods available for the identification and/or detection of Sporothrix spp. in different biological samples.
10.8
More on the topic Diagnosis:
- Diagnosis
- Diagnosis
- SelectiveIgM Deficiency
- Main Influences on Thyroid Function Tests
- Remission
- Quality ofLife
- Inherited and Congenital Diseases
- Narcolepsy-Cataplexy
- Management