Diseases of the biliary system in cats
Hepatitis is a rare disease in cats. However, cholangitis, an inflammatory disease of the hepatobiliary system, is common in cats.2 In a recent retrospective study of inflammatory liver diseases in 78 cats, more than 80% of cats with cholangiohepati- tis also had histological evidence of IBD, and about half had changes consistent with mild pancreatitis, implying that there is a relationship between inflammatory diseases of the abdominal organs.112 However, this relationship needs further clarification.
Cats may have different forms of cholangitis, which have been referred to by different names in the literature. However, overall, there are three different forms of cholangitis in cats: neutrophilic cholangitis, lymphocytic cholangitis, and cholangitis due to liver flukes (see 7.6.3.1-7.6.3.3 below).
7.6.3.1 Neutrophilic cholangitis
Pathogenesis
Neutrophilic cholangitis is due to an ascending infection of the biliary tree from the intestinal tract. Histologically, neutrophilic cholangitis is characterized by neutrophils in the lumen of the bile ducts and in the epithelium of the walls of the biliary tree. There may also be a neutrophilic inflammatory reaction around the bile ducts in the portal area. Neutrophilic cholangitis is usually an acute disease, but when it becomes more chronic, the inflammatory infiltrate may show a mixture of neutrophils, lymphocytes, and plasma cells. The associated diffuse inflammation of the entire biliary tree often causes cholestasis. Most of these cats, but not all, are distinctly icteric. However, there is no obstruction at the opening of the common bile duct into the duodenum and hence, there is no distension of the bile ducts.112,113
Symptoms
The clinical signs of patients with neutrophilic cholangitis are those of acute or subacute (1-3 weeks) inflammation with general illness, often with fever and icterus.
However, the degree of icterus is variable.Diagnosis
Serum bile acids concentrations and, in many cases, serum activities of ALT are increased, but these findings are nonspe- cific.75 Serum liver enzyme activities are usually typical of a mixed pattern of parenchymal and biliary injury, with normal to twofold elevations of AP activity and as high as tenfold elevations of ALT activity. Ultrasonography usually reveals no changes, but there may be thickening of the gall bladder wall.
A diagnosis of neutrophilic cholangitis can only be made by examining the bile. Gall bladder puncture with a thin needle should be performed under ultrasonographic guidance. Bile should be evaluated cytologically and by bacterial culture, which also permits the determination of the sensitivity of the cultured organism. Bacterial culture most often yields enteric organisms, such as E. coli, or in some cases Pseudomonas spp., or Enterococcus spp. Histological evaluation of a liver biopsy is helpful, but examination of the bile is essential.
Management
The routine treatment for neutrophilic cholangitis is the administration of antibiotics that are excreted well into the bile. The author prefers a treatment period of 3-4 weeks with amoxicillin and clavulanic acid. It is advisable to objectively evaluate the therapy by re-examination of the bile after completion of the antibiotic treatment course. The prognosis of feline patients with neutrophilic cholangitis is usually very good if a diagnosis is made early in the disease process.
7.6.3.2 Lymphocytic cholangitis
Pathogenesis
The pathogenesis of the lymphocytic form of cholangitis is very different than that of the neutrophilic form. Lymphocytic cholangitis is a chronic disease that progresses slowly over many months or even years. The inflammatory cells involved in this disease process are lymphocytes and plasma cells. The inflammatory cells can be found in the lumen of the bile ducts and in the bile duct epithelium, but they also progress to around the bile ducts in the portal areas (Figure 7.19).2,113-116 The inflammatory response of this condition causes portal fibrosis, and in very chronic cases, bridging fibrosis between the portal areas of different lobules leading to severe fibrotic changes.
The chronic inflammation of the bile ducts causes irregular distension of the bile ducts in and outside the liver. Abdominal ultrasonography shows dilated bile ducts (Figure 7.20) and thickened walls of the bile ducts that are usually readily detectable during ultrasonography.101,113The differential diagnosis for a lymphocytic cholangitis is an extrahepatic bile duct obstruction. The latter condition is rare, whereas lymphocytic cholangitis occurs quite frequently in cats. Histologically, the two diseases appear distinctly different. Because most affected cats have hyperglobulinemia and in some cases abdominal effusion, they can easily be misdiagnosed as having the effusive form of FIP; therefore, a liver biopsy is essential in differentiating these two conditions. The lymphocytic inflammation suggests an autoimmune-mediated disease process. At the same time, there is some evidence that this condition may be associated with a chronic bacterial infection with spirochetal bacteria (i.e., Helicobacter-like organisms).115 The most prominent finding on blood work is an elevated gamma globulin concentration, similarly to what is usually seen in cats with FIP. The liver tends to be enlarged and is therefore palpable in many cases. The diffuse inflammation of the entire biliary tree causes cholestasis and affected cats are often, but not always, icteric.
The chronic deformation of the bile ducts due to inflammatory infiltration makes them prone to secondary infections, such as by intestinal E. coli. Such a superimposed infection may cause a more acute exacerbation of the disease. As a result, the typical lymphocytic inflammation may change to an infiltrate with a more mixed inflammatory cell infiltrate.
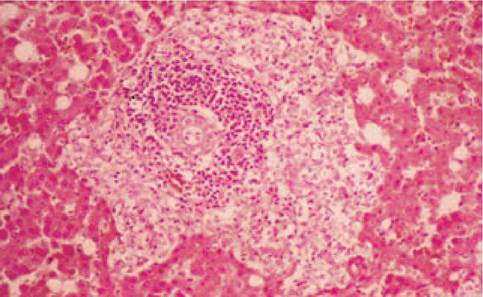
Figure 7.19:
Lymphocytic cholangitis. Histopathological image of a liver biopsy from a cat with lymphocytic cholangitis. The image is centered on a portal area and shows a large number of lymphocytes in and around the portal bile duct.
(H&E stain, 100 ?)
Figure 7.20:
Lymphocytic cholangitis. This figure shows an ultrasonographic image captured in a cat with lymphocytic cholangitis. Note the multiple dilated intra- and extrahepatic bile ducts.
Symptoms
As with other biliary diseases, the main clinical symptoms in cats with cholangitis are caused by nausea: decreased appetite, irregular eating, occasional vomiting, and chronic weight loss. Cholestasis may lead to icterus, which is present in most, but not all, cases of cholangitis.
Diagnosis
Lymphocytic cholangitis may be associated with a palpable enlargement of the liver. Blood work may reveal high serum bile acids concentrations with variable increases in serum ALT activity. The most consistent abnormal finding on blood work is an elevated serum gamma globulin concentration. Abdominal ultrasonography usually indicates a diffusely enlarged liver, often with an increased echodensity, which is, however, not specific either. In chronic cases, both intra- and extrahepatic bile ducts are irregularly distended. These ultrasonographic changes, in association with the typical histological findings of a liver biopsy, allow for a diagnosis.
Hepatic fluke infestation (i.e., Platynosomum concinnum), which is rather uncommon in cats, can also lead to cholangitis.116 However, the two diseases of the biliary system can be distinguished based on the clinical history and the type of inflammatory cells present.
Management
Lymphocytic cholangitis responds well to medication with ursodiol (ursodeoxycholic acid at 10-15 mg/kg PO q 24 h; can be divided into two doses),112-115 which suppresses the inflammatory response. Long-term treatment is mandatory at the same dosage. It is important to evaluate the response to therapy by repeat liver biopsy after 8 weeks of treatment. Medication must be continued until a complete resolution of the inflammation can be seen histologically.
It is advisable to concurrently treat these cats during the first four weeks of therapy with amoxicillin and clavulanic acid to treat any possible superimposed infections. Corticosteroids have often been recommended for the treatment of lymphocytic cholangitis, but evaluation of a series of cases seen at the University of Utrecht has revealed no beneficial effect for steroid administration.Nutritional support is an important component of medical therapy for cats with cholangiohepatitis. A balanced high-protein (i.e., 30% to 40% protein on a dry matter basis) maintenance diet is fed to cats that do not have signs of HE (see 7.6.1.1; recommendations for dietary management of hepatic lipidosis). Most cats that survive the initial period of treatment of 1 to 2 months have a good chance for cure and long-term survival. Cats with lymphocytic cholangiohepatitis appear to live comfortably for months to years. However, the dilation and fibrosis of the biliary system is permanent and these cats are predisposed to developing secondary bacterial infections (e.g., E. coli) of their abnormal bile ducts.
7.6.3.3 Extrahepatic bile duct obstruction (EBDO)
See 7.5.4.4 in the section on canine liver disease.
Extrahepatic bile duct obstruction in cats can be caused by infestation with liver flukes (e.g., Platynosomum spp., Am- phimeruspseudofelineus, Metametorchis intermedius).11^,,118 Hepatic fluke infestation has been reported most commonly in cats from areas with a warm, humid climate. Most cats are sub- clinical but hepatic fluke infestation may be responsible for EBDO in severely affected cats. Cats can acquire the infection by ingesting infected snails and lizards or freshwater fish. Histopathological changes of the hepatobiliary system induced by liver fluke infestation are mostly nonspecific. However, crosssections of flukes within bile ducts are occasionally seen histologically. The diagnosis is made by finding fluke ova in the feces of cats with compatible clinicopathological findings at abdominal exploratory.
Limited information concerning liver fluke infestation in cats suggests that praziquantel may be effective. Several dosage regimens have been used in reported clinical cases, although a regimen of 20 mg/kg praziquantel PO or SC q 24 h for 3 days is currently recommended. Because the use of praziquantel in this situation is an extra-label application, owner consent is recommended.
7.6.4