DISEASES OF THE COLON WITH DIARRHEA AS THE PRINCIPAL SIGN
Diarrhea is the most common sign associated with colonic disease in the dog and cat. Inflammatory diseases (colitis), which may be dietary, traumatic, parasitic, infectious, immune, or idiopathic, are the most important causes of large bowel diarrhea.
Other causes include neoplastic (lymphoma, adenocarcinoma), obstructive (intussusception, volvulus), and functional (irritable bowel syndrome) disorders. The principal causes and categories of large bowel diarrhea are summarized in Box 8-1.
Clinical Signs of Large Bowel Diarrhea
The first step in the recognition and diagnosis of large bowel diarrhea is the anatomic localization of the disease process to the colon based on the evaluation of the patient's defecation pattern and fecal characteristics (frequency, volume, consistency, color, odor, and composition). Large bowel diarrhea is characterized by frequent urges to defecate (usually greater than three times normal frequency), with each defecation producing small quantities of feces that often contain excessive mucus and sometimes fresh red blood. Urgency, resulting from irritability or inflammation of the distal colon, causes frequent premature expulsions of small quantities of feces that would otherwise be insufficient to trigger the defecation reflex. In addition, lapses in house training (“accidents”) may be caused by urgency and inability to control urges to defecate. The owner may also notice straining (tenesmus) as the patient remains in a squatting posture for an extended period of time after defecation or makes repeated attempts to defecate within a period of a few minutes. These attempts may produce little or no feces, or sometimes a small amount of feces composed almost entirely of mucus, exudate, and blood.
Because many colonic diseases are associated with mucosal injury, inflammation, or ulceration, abnormal fecal constituents are frequently found in large bowel diarrhea.
These include (1) fresh red blood (hematochezia), which originates from sites of erosion or ulceration; (2) mucus, which originates from the abundant goblet cells in the colon that respond to mucosal injury by an outpouring of mucus; and (3) exudate (leukocytes), which originates from sites of inflammation. Blood may coat the feces, streaks of blood may be mixed within the feces, or drops of blood may be passed at the end of defecation. Excessive mucus may give the feces a glistening or jellylike appearance. Exudates are detected by the positive identification of fecal leukocytes on conventional cytology stains. These abnormal constituents—red blood, mucus,
| Causes of Large Bowel Diarrhea | |
| Dietary factors | Mycobacteria |
| Abrasive colitis (ingestion of foreign material—e.g., | Enteropathogenic Escherichia coli (?) |
| bones, hair) | Fungi |
| Dietary hypersensitivity (food allergy?) | Histoplasma capsulatum |
| Fiber-responsive diarrhea | Others (pythiosis, Candida albicans, Aspergillus sp.) |
| Helminths | Algae (Prototheca sp.) |
| Whipworms (Trichuris vulpis) | Idiopathic inflammatory bowel disease |
| Hookworms (Ancylostoma caninum) | Lymphocytic-plasmacytic colitis |
| Strongyloides tumefaciens | Eosinophilic colitis |
| Protozoa | Suppurative (neutrophilic) colitis |
| Entamoeba histolytica | Granulomatous colitis |
| Balantidium coli | Histiocytic (PAS+) ulcerative colitis of boxer dogs |
| Trichomonas sp. | Drug-induced colonic ulceration |
| Giardia sp. (?) | Steroidal and nonsteroidal antiinflammatory drugs |
| Viruses | Pancreatitis-associated colitis |
| FIP coronavirus (pyogranulomatous colitis) | Ischemia |
| Retroviruses (FeLV; FIV) | Trauma, infarction, volvulus, strangulation |
| Bacteria | Intussusception |
| Salmonella sp. | Cecocolonic, ileocolonic |
| Campylobacter jej un i | Neoplasia |
| Clostridium perfringens, Clostridium difficile (?) | Benign (adenomatous polyp) |
| Yersinia enterocolitica,Yersinia pseudotuberculosis | Malignant (adenocarcinoma, lymphoma, others) |
| Bacillus piliformis (Tyzzer's disease) | Motility dysfunction—irritable bowel syndrome |
FIP, Feline infectious peritonitis; FeLV, feline leukemia virus; FIV, feline immunodeficiency virus; PAS, periodic acid-Schiff.
and leukocytes—are localizing signs indicative of colonic disease.
Because the principal function of the colon is absorption of water and electrolytes rather than digestion and absorption of nutrients, nutrient malabsorption and steatorrhea are absent in large bowel diarrhea. Thus dramatic weight loss and wasting are unlikely if the patient is eating, and the daily fecal output (volume or weight of feces) is usually only minimally increased. This contrasts with the substantial increase in fecal output of dogs with small intestinal disease. The characteristics of small bowel diarrhea are discussed in Chapter 1. Diffuse diseases of the GI tract may produce concurrent small and large bowel signs and sometimes gastric signs as well.
It has been estimated that vomiting is an associated sign in about 30% of patients with colitis.Diagnostic Approach for Large Bowel Diarrhea
Diarrhea as a clinical sign is relatively nonspecific; however, once it is localized to a disorder of the large bowel, a logical diagnostic approach can be followed. Specific treatment or intervention is usually necessary, and this generally requires either a specific diagnosis or at least a histopathologic characterization. Initial evaluations should be aimed at diagnosis of dietary, parasitic, and infectious causes of diarrhea. This should include multiple fecal examinations for whipworm ova and protozoa, therapeutic deworming trials (fenbenda- zole, 22 mg/lb orally daily for 3 days), fecal examinations for Clostridium perfringens spores and toxin, and a 4-week dietary trial using a highly digestible commercial or homemade GI diet alone and with fiber added (psyllium). If diarrhea persists and the cause is not apparent, the next phase of diagnostic evaluations should include a complete blood count (CBC), serum chemistry profile, urinalysis, additional fecal examinations for infectious agents (cytologic examination, toxin assay, cultures), and abdominal imaging (radiography and ultrasonography). Finally, complete colonoscopic examination and biopsy are performed. The various diagnostic procedures for animals with large bowel diarrhea are summarized in Table 8-1.
Physical Examination
A complete physical examination may reveal important clues about the severity, nature, and cause of diarrhea, although in many patients the findings are nonspecific. An effort should be made to identify underlying extraintestinal diseases that may be a cause or consequence of diarrhea. The colon and rectum should be thoroughly examined by palpation, and if abnormalities are identified, additional diagnostic studies, such as colonoscopy, radiography, or ultrasonography, are usually indicated. For example, abdominal palpation of the colon (and small intestines as well) may reveal masses, thickenings, intussusception, distention, fecal impaction, pain, or associated changes in abdominal lymph nodes and other abdominal organs.
Digital palpation of the rectum may reveal foreign objects, intramural or extramural masses, strictures, or abnormalities of mucosal texture. In addition, the fecal material obtained on the palpation glove can be inspected for abrasive particles (such as bone chips), blood, or mucus. Fecal material also can be examined microscopically for parasites and inflammatory cells and submitted for culture if indicated.Consideration of Dietary, Parasitic, and Infectious Causes
Before hospitalizing a patient with large bowel diarrhea for an in-depth diagnostic work-up, the possibilities of dietary, parasitic, or infectious causes should initially be considered. Ingestion of abrasive materials such as bones or chew toys can injure the rectocolonic mucosa, producing abrasive colitis and signs of diarrhea and hematochezia that typically last 2 to 3 days. The diagnosis can usually be made from a thorough dietary history and inspection of the feces for abrasive particles.
Acute nonspecific large bowel diarrhea often resolves with restriction of food intake for 24 to 48 hours followed by gradual resumption of feeding using a bland digestible diet. Chronic nonspecific diet-responsive diarrhea can be resolved in many cases by strict feeding of a balanced, highly digestible diet using one of the commercially available “GI diets,” such as Low Residue Formula (Iams), Select Care Sensitive (IVD), Prescription i/d (Hill's), EN (Purina), or Low Fat (Waltham), or using a comparable homemade diet following published recipes. In dogs if diarrhea persists after a 4-week feeding trial, then add fermentable soluble fiber in the form of psyllium (Metamucil, 1 to 3 tbsp/day) or oat bran (1 to 3 tbsp/day) to determine if the patient has fiber-responsive large bowel diarrhea.
In dogs, whipworms are the most common cause of colitis in many practice areas and should be ruled out by fecal flotation or, if occult infection is
Diagnosis of Large Bowel Diarrhea
| Procedures | Diagnostic Findings |
| Dietary history | Ingestion of bones or other foreign materials, which may cause abrasive colitis Dietary hypersensitivity as a potential cause of inflammatory bowel disease |
| Abdominal palpation Rectal palpation Fecal examinations Gross inspection Flotation Saline smear Cytologic examination | Intestinal masses, thickenings, distention, pain, or associated lymphadenopathy Foreign objects, masses, strictures, or abnormalities of mucosal texture Blood, mucus, ingested foreign material Trichuris ova Protozoan trophozoites Inflammatory cells, Histoplasma organisms, clostridial endospores, Campylobacter organisms |
| Bacteoriologic examination Enterotoxin assays Hemogram Serum biochemistry studies | Campylobacter, Salmonella, etc. Clostridium perfringens enterotoxin Anemia, eosinophilia, neutrophilia, neutropenia Hyperkalemia/hyponatremia of whipworm (pseudo-Addison’s syndrome) Hypoproteinemia (enteric protein loss) Underlying renal failure or pancreatitis Other metabolic and systemic alterations that could cause or result from colonic disease |
| Serologic examination Barium enema radiography | Histoplasma titer (in endemic areas) Intussusceptions, neoplasms, polyps, strictures, and inflammatory lesions (colonoscopy is generally preferred over barium enema) |
| Abdominal ultrasonography | Intestinal and abdominal masses, intussusception, mesenteric lymphadenopathy, pancreatitis |
| Colonoscopy | Visual examination and biopsy for definitive or histopathologic diagnosis in most neoplastic or inflammatory diseases of the colon |
| Therapeutic trials | Response to fenbendazole suggests occult whipworm infection Response to dietary trials with novel protein diets suggests dietary hypersensitivity as a cause of lymphocytic-plasmacytic colitis Response to dietary fiber supplementation indicates fiber-responsive enteropathy |
suspected, by a therapeutic trial of an effective anthelmintic such as fenbendazole (Panacur). Hookworms can also cause colitis. Although less common, protozoan causes of colitis (e.g., Trichomonas) can be detected rapidly by examination of saline fecal smears for the presence of motile trophozoites. In warm, humid regions endemic for Strongyloides tumefaciens in cats (e.g., parts of the southern United States), sedimentation or Baermann techniques can be used to identify larvae in the feces.
Campylobacter, Salmonella, and C. perfringens are becoming recognized as important bacterial causes of enterocolitis. Campylobacter and Salmonella can be diagnosed by specialized fecal cultures. Such cultures are particularly indicated when examination of fecal cytologic preparations reveals the presence of numerous fecal leukocytes or when there is an outbreak of diarrhea in groups of animals. C. perfringens enterotoxigenic diarrhea is suggested by the presence of large numbers of endospores (more than five spores per high-power oil immersion field) with a “safety pin” or “tennis racket” configuration in fecal cytologic preparations stained with Diff-Quik; however, fecal assays for C. perfringens enterotoxin are probably a more reliable means of diagnosing clostridial diarrhea (see section on C. perfringens).
Histoplasmosis is an important cause of chronic colitis in areas endemic for this mycotic infection. The diagnosis is usually based on either positive serologic study (immunodiffusion or complement fixation) or identification of the organisms in exfoliative cytology specimens from rectocolonic mucosa. Sabourauds medium can be used to culture feces for Histoplasma and other fungi or for Prototheca, a rare cause of colitis, but culture growth is slow (up to 2 weeks) and the isolation rate is low.
Hematology and Serum Biochemistry
In addition to fecal examinations, the initial database for undiagnosed chronic large bowel diarrhea should include a complete hemogram (CBC) and serum biochemistry profile. Significant CBC findings may include (1) anemia, which could result from enteric blood loss or depressed erythropoiesis due to chronic disease; (2) eosinophilia, which could suggest parasitism, eosinophilic enterocolitis, or sometimes other inflammatory or neoplastic intestinal diseases; (3) regenerative neutrophilia, which could suggest bowel inflammation (particularly involving the deeper layers), necrosis, or neoplasia; and (4) degenerative or toxic neutropenia, which could suggest overwhelming sepsis or endotoxemia, such as occurs with bowel ischemia, necrosis, or perforation.
A serum biochemistry profile and urinalysis should be considered to identify metabolic or extraintestinal disorders that could cause or result from diarrhea. For example, underlying systemic diseases that can cause diarrhea may be detected, such as renal failure (increased levels of blood urea nitrogen and creatinine), pancreatitis (increased amylase and lipase levels), liver disease (e.g., abnormal serum liver enzymes levels), or hypoadrenocorticism (hyperkalemia and hyponatremia). In addition, serum chemistry findings can be used to evaluate potential complications of large bowel diarrhea, such as dehydration, electrolyte abnormalities, and hypoproteinemia. Because of the high incidence of hyperthyroidism in cats older than 5 years of age and because this disorder is occasionally manifested as unexplained diarrhea, cats in this age-group with diarrhea should have a screening serum thyroxine (T4) level measured.
Colonoscopy and Biopsy
Most cases of chronic large bowel diarrhea in which extraintestinal, dietary, parasitic, and infectious causes have been excluded require colonoscopic examination and mucosal biopsy for definitive diagnosis or accurate characterization of the disease. Colonoscopy allows direct visualization of the lumen of the colon, sampling of luminal content, and directed forceps biopsy of the mucosa. Suitable rigid colonoscopes are relatively inexpensive and easy to use. Because colonic diseases are often diffuse, examination of the descending colon with a rigid instrument is sufficient for diagnosis in many patients. However, when lesions are located predominantly in the ascending or transverse colon, areas that are inaccessible with a rigid colonoscope, a flexible fiberoptic colonoscope must be used. The normal colonic mucosa through a colonoscope appears pale pink and reflects light uniformly. The mucosa should be nonfriable, thin enough that the submucosal vessels are visible, and free of ulcers, thickened folds, masses, or strictures. Cultures, exfoliative cytology specimens, and biopsy specimens of the colonic mucosa are easily obtained through the instrument.
There are occasions when colonoscopy cannot be used to evaluate adequately or to perform deep enough biopsies of lesions in the proximal colon, especially when deep inflammatory or neoplastic lesions involve the region of the ileocecocolic junction. Under these circumstances, examination and biopsy by laparotomy are required for accurate diagnosis.
Radiography and Ultrasonography
Plain abdominal radiography is indicated for detection of foreign material in the colon, intestinal masses, intussusception, or an abnormal gas-fluid pattern that would suggest obstruction or volvulus. Barium enema contrast radiography is useful in selected cases of large bowel diarrhea for detection of ileocolonic intussusceptions, cecal inversions, neoplasms, polyps, strictures, colonic displacement, colonic shortening, and chronic inflammatory lesions. Some of these lesions can also be detected in the latter phases of an upper GI barium contrast radiographic series; however, the lower bowel is generally evaluated better by a barium enema study. (See Chapter 2 for a more detailed discussion of contrast radiography.) However, it must be emphasized that if flexible fiberoptic colonoscopy is available, it is generally preferred over barium radiography for evaluation of the proximal colon because it is easier to perform and yields more definitive diagnostic information.
Abdominal ultrasonography can be a useful diagnostic aid in selected cases of unexplained diarrhea for noninvasively defining intestinal and other abdominal or perirectal masses, for diagnosis of intussusceptions, and for evaluating the mesenteric lymph nodes, pancreas, liver, and prostate (see Chapter 2).
Therapeutic Trials
Therapeutic trials can sometimes support a tentative diagnosis when accompanied by other supportive clinical evidence. For example, occult whipworm infection is often diagnosed circumstantially by rapid resolution of signs in response to fenbenda- zole therapy. In some patients, nonspecific diet- responsive large bowel diarrhea is resolved by feeding a highly digestible diet or a diet supplemented with fiber as described previously in this section. Similarly, the response to trial-and-error test diets plays an important role in establishing dietary hypersensitivity as a cause of lymphocytic- plasmacytic colitis.
Abrasive Colitis
Ingested bone particles, pieces of chew toys, or other indigestible abrasive foreign materials (stones, hair, plants, wood, cloth, carpeting, foil, plastic), when incorporated into the fecal mass, may cause abrasive colitis because of a traumatizing sandpaper-like effect on the rectocolonic mucosa during transit. Abrasive injury is usually transient and self-limiting after 2 to 3 days, although repeated episodes in patients that have frequent dietary indiscretions may mimic other causes of chronic intermittent colitis. Dietary history and examination of the feces for abrasive particles are usually sufficient to establish the diagnosis. Management is based on eliminating the source of ingested abrasive material.
Diet-Responsive and Fiber- Responsive Large Bowel Diarrhea
These conditions are characterized by chronic nonspecific large bowel diarrhea. The diagnosis is based on a complete absence of abnormal findings on diagnostic evaluations, minimal abnormalities on colonoscopy, and complete response to dietary manipulation. A 4-week feeding trial of a new diet is usually adequate to determine response. Some of these patients respond simply to feeding of a balanced, highly digestible diet (i.e., moderate to restricted fat level with digestible protein and carbohydrate) using one of the commercially available “GI diets,” such as Low Residue Formula (Iams), Select Care Sensitive (IVD), Prescription i/d (Hill’s),EN (Purina), or Low Fat (Waltham), or using a comparable homemade diet. One example of a homemade diet combines turkey, rice, and safflower oil. Other acceptable recipes for homemade “GI diets”are published elsewhere. The advantage of a highly digestible diet would be less undigested “residue” presented to the colon from the small intestines. This helps to prevent unabsorbed fat from reaching the colon, where it can be metabolized to hydroxy fatty acids that produce diarrhea.
In dogs the diagnosis of fiber-responsive large bowel diarrhea is based on an absence of abnormal diagnostic findings, minimal abnormalities on colonoscopy, and responsiveness to supplementation of a digestible diet with fermentable soluble fiber in the form of psyllium (Metamucil, 1 to 3 tbsp/day) or oat bran (1 to 3 tbsp/day). Some of these patients may actually have so-called irritable bowel syndrome (see later section). Fermentable soluble fiber is fermented by colonic bacteria to short-chain fatty acids (SCFAs) that provide an energy source for colonic epithelium, protect against mucosal injury, and acidify bowel contents, which may reduce proliferation and sporulation of enteropathogenic bacteria such as C. perfringens. Fiber also has other beneficial effects on fecal water content, fecal bulk, and colonic myoelectrical function.
Novel protein diets are used in diagnostic trials and treatment for chronic colitis related to dietary hypersensitivity. This is discussed in the section on lymphocytic-plasmacytic colitis.
Parasitic Colitis
Whipworm Colitis
Whipworm (Trichuris vulpis) infection is a common cause of acute, chronic, or intermittent signs of large bowel diarrhea in dogs in many practice areas. The adult nematode has a predilection for the proximal colon and cecum, where its distinctive thread like head end or “whip” firmly embeds deep within the mucosa to feed on blood and tissue fluids, thereby resulting in colitis and typhlitis.
Whipworms infect dogs of all ages. Although there may be minimal clinical signs in light infestations, trichuriasis frequently causes mucoid large bowel type of diarrhea with urgency and sometimes hematochezia. Because of these signs, whipworm infection is often mistaken for other, more serious forms of colitis or colonic neoplasia. In addition, a condition of pseudohypoadrenocorticism characterized by hyperkalemia and hyponatremia in the presence of normal adrenal function has been associated with severe whipworm diarrhea in several dogs. The feline whipworms, Trichuris campanula and Trichuris serrata, are considered to be very rare and usually are not associated with clinical signs.
Whipworm infections occur by ingestion of infective ova, and the life cycle is direct. The prepatent period is approximately 3 months. Because ova may survive and remain infectious in the environment for 4 to 5 years, contaminated ground is probably the major reservoir of infection.
Definitive diagnosis of whipworm infection necessitates identification of the characteristic brown, bipolar-operculated, football-shaped ova by routine fecal flotation. Repeated fecal examinations may be necessary to identify ova because of the unusually long prepatent period and also because it is not uncommon for active infection to be characterized by prolonged periods when ova are not shed in the feces. It is estimated that up to 50% of dogs presenting with whipworm diarrhea have ova-negative or so-called occult infections. Alternative means of diagnosis are directly by colonoscopic observation of adult whipworms in the bowel lumen or indirectly by observing resolution of signs in response to a therapeutic trial of an effective anthelmintic.
Whipworms are treated with fenbendazole (22 mg/lb orally for 3 consecutive days). Treatment should be routinely repeated at 3 weeks and 3 months because whipworms are difficult to eradicate. In refractory cases, a 5-day course of fenben- dazole is recommended. Febantel is an alternative treatment for whipworms. Regular use of milbe- mycin (Interceptor, Sentinel) for heartworm prevention also helps to control whipworm infections. Because whipworm ova survive so well in the environment, frequent reinfection is a common problem. Therefore feces should be collected and disposed of properly whenever possible. In dogs with frequent access to ground that has been heavily contaminated with whipworm ova, a common situation in many public parks and backyards, reinfection is so frequent that retreatment every 2 to 3 months may be necessary. It is virtually impossible to eradicate the parasite from infected ground; however, concrete runs can be disinfected with dilute sodium hypochlorite solution or by flaming.
Rarely trichuriasis has been associated with severe transmural granulomatous typhlitis, which may be palpable as a tender right midabdominal mass. This lesion may be refractory to anthelmintics and require typhlectomy.
Hookworm Colitis
Although the common canine hookworm, Ancylostoma caninum, is primarily a small intestinal parasite, it occasionally parasitizes the colon in large numbers. Hookworms embed their mouthparts in the mucosa to suck blood, leaving bleeding punctiform ulcers as they “graze.”When they involve the colon, they produce a bloody mucoid diarrhea characteristic of colitis.
Young dogs are most often affected, and the diagnosis is usually readily established by identification of the characteristic hookworm ova by routine fecal flotation. Eosinophilia is a common ancillary finding on CBC.
There are many anthelmintics that are effective for eradicating hookworms, including the standard recommended dosages (4.5 mg/lb for patients under 5 lb; 2.25 mg/lb for patients over 5 lb) of pyrantel pamoate (Nemex), fenbendazole, or febantel. Most heartworm preventatives also control hookworms.
Strongyloides Colitis
S. tumefaciens is a tiny nematode parasite of cats in warm, humid tropical regions such as the Gulf region of the United States. The adult parasites burrow within the mucosa of the large intestine. Infection is usually asymptomatic, but in some cats the parasite causes peculiar tumorlike, white, 2- to 3-mm nodular proliferations in the colonic mucosa and submucosa that are associated with signs of chronic diarrhea and debilitation.
Ova that contain first-stage Strongyloides larvae can be identified in feces by flotation techniques, and free larvae may be identified by direct microscopic examination of feces or by a Baermann technique. In addition, the diagnosis can be established by colonoscopic observation and biopsy of the mucosal nodules, which are filled with adult worms.
Strongyloidiasis can be treated with a 5-day course of fenbendazole (23 mg/lb/day orally).
Protozoan Colitis
Pentatrichomonas hominis, Entamoeba histolytica, and Balantidium coli are large bowel protozoal parasites that are occasionally associated with colitis and large bowel diarrhea in animals. In addition, Giardia, which is primarily a small bowel parasite (see Chapter 6), has been associated with bloody- mucoid large bowel diarrhea on very rare occasions. All of these protozoa are responsive to treatment with metronidazole (Flagyl).
Trichomoniasis
Trichomonas spp. are motile, pear-shaped, flagellated protozoa that inhabit the colon and cecum of dogs and cats and have been found in both normal and diarrheic feces. The pathogenicity of these protozoa in dogs has not been conclusively established, but massive numbers of trichomonads are sometimes found in diarrheic feces of puppies and are especially associated with unsanitary overcrowded kennel conditions and coinfection with other parasites. Tritrichomonas foetus has recently been identified as a frequent cause of chronic large intestinal diarrhea in young cats, especially cats confined in crowded cattery conditions. The diarrhea may wax and wane, may be malodorous, and may contain blood or mucus. The diagnosis of trichomoniasis is based on identification in saline fecal smears or in fecal culture (Modified Diamond's Media or InPouch TF kit) of motile, pear-shaped, flagellated trophozoites with characteristic wavelike motion of an undulating membrane and a constant erratic turning and rolling motion. Feces for detecting trichomonads should be taken directly from the rectum or examined within minutes of defecation, while trophozoites are still motile. Trichomonads lack a cyst stage. Fecal polymerase chain reaction (PCR) testing has also been used in cats. Trichomonas are extremely difficult to eradicate in cats. Numerous antibiotic agents have been evaluated without success. Treatment can reduce the number of organisms and improve clinical signs, but it usually does not eliminate the infection. The patient should also be evaluated and treated for concurrent infection with other parasites and enteropathogens. Proper sanitation measures should be instituted to control infection in animals housed in groups.
Amebic Colitis
E. histolytica, primarily a human pathogen, may rarely cause amebic colitis in dogs and cats. Amebic invasion of the colonic mucosa and submucosa results in ulceration and signs of bloody- mucoid large bowel diarrhea with tenesmus. Diarrhea is usually severe and may simulate other forms of chronic colitis or is manifested as an acute dysentery. Both forms of Entamoeba, the trophozoite and cyst, are infectious for animals. Infection is most likely acquired from ingestion of food or water contaminated with human feces, such as drinking from polluted water sources (free- roaming animals) or toilets (house pets). The diagnosis is based on identification of ameboid trophozoites with pseudopodial movement in saline smears of fresh diarrheic feces, amebiccysts in zinc sulfate flotation of formed feces, or trophozoites in colon biopsy specimens. Amebic colitis responds to metronidazole (12 to 15 mg/lb orally two times a day for 5 to 10 days) or furazolidone (1 mg/lb orally three times a day for 7 days).
Balantidiasis
B. coli, a ciliated protozoan that primarily infects swine, is a rare cause of chronic ulcerative colitis in dogs. Rural dogs in contact with swine feces are most at risk for the disease. Humans can also be infected. Dogs with balantidiasis are usually coinfected with whipworms, and thus it has been suggested that whipworm-induced damage to the colonic mucosa may be a predisposing factor. The diagnosis is based on identification of extremely large (40-80 ? 25-45 μm), oval, brown, rapidly swimming ciliated trophozoites with prominent macronuclei in saline smears of fresh feces or on identification of protozoal cysts in zinc sulfate or sedimentation preparations of feces.As with Entamoeba and Giardia, the trophozoite stage of Balantidium can be seen in diarrheic feces, whereas cysts are more likely to be found in formed feces. Balantidiasis is treated with metronidazole (10 to 15 mg/lb orally twice a day for 5 to 10 days).
Viral Colitis
The colon may be significantly involved in generalized viral infections of the intestinal tract. Lesions of acute colitis are especially common in parvovi- ral infections of both the dog and the cat. In addition, the colon may be involved in some of the multisystemic viral diseases. For example, in dogs the epitheliotropic attack of canine distemper virus may involve the colon, whereas cats infected with feline leukemia virus (FeLV), feline immunodeficiency virus (FIV), or feline infectious peritonitis (FIP) virus sometimes have diarrhea associated with enterocolitis that varies from necrotizing to ulcerative to pyogranulomatous. (See Chapter 6 for further discussion of viral infections of the GI tract.)
Bacterial Colitis
Invasive enteropathogenic bacteria primarily invade the colon and distal small bowel, where the mucosal damage they cause leads to inflammation, exudation, mucus secretion, and bleeding. Thus typical signs of large bowel diarrhea and hematochezia are characteristic of these infections. Bacterial enterotoxins may also play a role in the pathogenesis of diarrhea. Although the clinical importance of the various enteropathogenic bacteria in animals has not yet been fully defined, Salmonella sp., Campylobacter jejuni, Yersinia sp., Bacillus piliformis, and Clostridium sp. may be associated with colitis and large bowel diarrhea in dogs and cats.
Salmonellosis
Manifestations of Salmonella infection may be categorized into three syndromes: (1) the subclinical carrier state, (2) enterocolitis, and (3) enterocolitis with bacteremia. Clinical salmonellosis is relatively uncommon compared with the prevalence of the subclinical carrier state. When it does occur, Salmonella enterocolitis is characterized by acute watery or mucoid diarrhea (containing blood in severe cases), vomiting, tenesmus, fever, anorexia, lethargy, abdominal pain, and dehydration. Most patients recover within 3 to 4 weeks, although shedding of organisms often persists for up to 6 weeks, sometimes longer. Salmonella also appears to cause chronic or intermittent diarrhea in some patients. Rarely, acute enterocolitis may develop into a potentially fatal bacteremia or endotoxemia with signs of endotoxic shock and even disseminated intravascular coagulation (DIC).
The diagnosis of salmonellosis should be suspected in patients that develop acute diarrhea and have identifiable risk factors, such as known or probable exposure, young age, immune deficiency, debilitating illness, or housing in overcrowded or unsanitary conditions. A severe acute febrile illness with hemorrhagic diarrhea in cats has been linked to a highly fatal Salmonella outbreak in songbirds and transmission to cats via ingestion of dead birds. In addition, nosocomial outbreaks with high morbidity and mortality have been recorded in hospitalized patients, with the greatest risk occurring in those patients with severe illness, those undergoing major surgery, those hospitalized for 5 or more days, and those receiving glucocorticosteroids, anticancer chemotherapy, or oral antibiotics (such as ampicillin) that upset the normal flora. Routine diagnostics are usually noncontributory, except that in severe cases with bacteremia and endotoxemia a degenerative neutropenia may be found. Confirmation of the diagnosis depends on isolation of Salmonella sp. from properly cultured fecal specimens or from blood cultures in bacteremic animals.
The use of antibiotics in the treatment of salmonellosis is controversial. Salmonella invasion that is confined locally to the mucosa produces enterocolitis that is both self-limiting and not likely to be affected by antibiotics. In fact, antibacterial therapy, especially oral nonabsorbable antibiotics that alter the flora, may actually prolong shedding of organisms and encourage development of a prolonged convalescent carrier state. However, antibiotics are indicated whenever Salmonella invasion becomes severe or complicated by bacteremia and endotoxemia, as indicated by signs such as shock, dehydration, high fever or hypothermia, and extreme depression, or by laboratory findings such as azotemia, electrolyte imbalances, neutropenia, hypoglycemia, hypoproteinemia, or coagulopathy. Peracute onset and severe hematochezia also may be indications of impending systemic invasion and should prompt antibiotic therapy. The choice of an antibiotic may be based on culture and sensitivity, although most isolates are susceptible to enrofloxacin (Baytril, 2.5 mg/lb two times a day) or trimethoprim-sulfadiazine (7 mg/lb two times a day). Fluoroquinolones such as enrofloxacin can be effective for treating both active disease and the carrier state. In addition to antibiotics, fluid and electrolyte replacement and identification and correction of underlying predisposing conditions are important aspects of therapy. Antibiotics should be continued for 7 to 10 days, and feces should be recultured 1 and 4 weeks after treatment. The prognosis for most patients with salmonellosis is good, although the mortality rate can be high in outbreaks in extremely susceptible populations (e.g., hospital patients, neonates). Proper hygiene in handling infected patients is necessary to prevent feco-oral or fomite transmission of infection to other animals or to humans.
Campylobacteriosis
C. jejuni are fastidious, microaerophilic, gramnegative, motile, slender, curved bacteria that have emerged as important pathogens of animals and humans worldwide. In dogs and cats the full spectrum of clinical manifestations remains to be defined because it is known that the number of clinically normal animals that shed Campylobacter in their feces is comparable to the incidence of shedding by diarrheic animals. Isolation rates vary widely, from less than 1% in confined pet populations to 50% or more in some animal pounds and shelters. Thus conditions of close confinement or poor sanitation apparently provide the greatest opportunity for exposure.
Because it is difficult to produce enteritis with Campylobacter experimentally in dogs and cats and because many of the animals that harbor these organisms are asymptomatic, it has been debated whether Campylobacter by itself even causes diarrhea in the dog and cat unless superimposed on other enteropathogenic infections, such as viruses, other bacteria, Giardia, or helminths. Nevertheless, clinical signs that have been associated with Campylobacter infection in dogs and cats have been attributed to superficial erosive enterocolitis or enterotoxin-mediated secretory diarrhea and are characterized by a 5- to 15-day course of watery- mucoid diarrhea that occasionally contains blood and may be accompanied by vomiting or tenesmus. Fever is usually mild or absent. In some patients the diarrhea appears to be chronic or intermittent.
A presumptive diagnosis of campylobacteriosis can be made by identification of slender, curved, gram-negative rods that have a characteristic W shape in stained fecal smears. The presence of fecal leukocytes may also be noted. In fresh saline smears, an experienced examiner may be able to tentatively identify Campylobacter with darkfield or phase-contrast microscopy as highly motile, darting, spiral or S-shaped bacteria; however, they should not be confused with spirochetes and other motile bacteria that are part of the normal flora. Definitive diagnosis requires isolation of Campylobacter from fresh feces with special selective media. Because Campylobacter are microaerophilic and difficult to isolate, fecal specimens should be obtained directly from the rectum and cultured or placed in transport media immediately after collection.
The antibiotic of choice for treating campy- lobacteriosis is erythromycin (5 to 7 mg/lb orally three times a day for 7 days); however, resistant strains have occasionally been isolated. Anorexia and vomiting are frequent side effects of erythromycin. Other effective oral antibiotics include neomycin (Biosol, 5 to 10 mg/lb orally three times a day), enrofloxacin (2.5 mg/lb orally two times a day), chloramphenicol, furazolidone, and doxycycline. Although fatalities in dogs and cats have been reported, the prognosis is considered good, and antibiotics are rapidly effective for eliminating fecal shedding of the organisms. Fecal cultures should be repeated 1 and 4 weeks after treatment. Because contact with feces from infected animals is a potential source of infection for humans as well as other animals, owners of infected pets should be advised to take standard precautions, such as proper disposal of potentially infectious feces, hand washing after handling infected animals, and separating infected animals from infants and small children until posttreatment cultures confirm that infection has been eliminated.
Yersiniosis
Yersinia enterocolitica, a motile, gram-negative rod, is recognized as a cause of acute and chronic enterocolitis in humans and has been isolated from small numbers of dogs and cats, mostly in Japan and Scandinavia. The majority of positive fecal isolations from dogs and cats have been from clinically healthy animals. On rare occasions in young dogs, Y. enterocolitica has been associated with enterocolitis characterized by bloody-mucoid large bowel diarrhea, tenesmus, and an absence of fever or systemic signs. An association with clinical disease in cats has not been established.
Y. enterocolitica grows best at colder temperatures, and special isolation methods are needed to culture the organism from feces. It also may be cultured from infected tissues or blood if the patient is bacteremic. Treatment for 7 to 10 days with trimethoprim-sulfadiazine (7 mg/lb two times a day), tetracycline, chloramphenicol, or an aminoglycoside is usually effective; however, antibiotic sensitivity testing is recommended. Yersinia infection of pets may be a public health concern.
In cats Yersinia pseudotuberculosis infection is a disseminated pyogranulomatous disease that is acquired from ingestion of infected rodent and avian prey and that primarily involves the GI tract, abdominal lymph nodes, and liver. Consequently the clinical signs are vomiting, diarrhea, weight loss, depression, fever, and icterus. Feline pseudotuberculosis is usually progressive and fatal, although clinically healthy carriers of the organism also have been found. Treatment consists of a prolonged course of an antibiotic such as trimethoprimsulfadiazine, tetracycline, or chloramphenicol, but the prognosis is guarded.
Bacillus Piliformis
Tyzzer's disease, caused by a pleomorphic, gramnegative, spore-forming, obligate intracellular bacillus called B. piliformis, is a rare but fatal disease characterized by hemorrhagic-necrotizing enterocolitis and hepatic necrosis. The principal reservoirs of infection are rodents. Puppies and kittens are most often affected, and the disease may complicate parasitism and viral infections such as parvovirus, FeLV, and canine distemper virus. The progression ofTyzzer's disease is rapid; most patients die within 48 hours after the initial onset of signs of anorexia, depression, and diarrhea. Successful therapy has not been reported.
Definitive diagnosis of Tyzzers disease is difficult because B. piliformis cannot be cultured on artificial media. Instead, mouse inoculation or embryonated egg culture techniques must be used to isolate the organisms. Most cases have been diagnosed at necropsy by the histologic identification of typical-appearing bundles of intracellular filamentous bacilli at the margins of necrotic foci within liver and intestinal lesions with special stains such as methenamine silver, Giemsa, or periodic acid-Schiff (PAS).
Clostridial Diarrhea
Enterotoxigenic C. perfringens is an important cause of acute and chronic large bowel diarrhea in dogs and cats. In addition, Clostridium difficile, the primary cause of antibiotic-associated pseudomembranous colitis in humans, is also found in dogs and cats and may occasionally be associated with diarrhea.
Diarrhea Associated With Clostridium
Perfringens
C. perfringens is a large anaerobic gram-positive bacillus that normally exists in the intestinal tract of most dogs and cats. Enterotoxin-producing strains of C. perfringens can be associated with nonspecific episodes of diarrhea, acute hemorrhagic diarrhea, chronic or recurrent diarrhea, and outbreaks of diarrhea in animal groups. These bacteria normally reside in the bowel in the vegetative form, but they can release their toxin during sporulation endogenously within the bowel or exogenously in contaminated food. The cpe gene that regulates production of C. perfringens enterotoxin (CPE) is up-regulated by factors that activate sporulation; thus the presence of clostridial endospores in feces or food has been suggested as an indirect marker for the presence of CPE.Whether derived endogenously or ingested, CPE causes diarrhea by binding to intestinal epithelium and causing increased permeability, hypersecretion, and cell damage (cytotoxicity). Endogenous sporulation and the production of CPE can be associated with alteration of the intraluminal environment caused by sudden changes in diet, antibiotic administration, alkaline conditions, immunosuppression, inflammatory bowel disease (IBD), or concurrent intestinal infections.
Clinical Signs
Enterotoxigenic C. perfringens infection is associated with large bowel diarrhea that varies from watery to soft and may contain mucus or blood. Increased frequency is common, and tenesmus may be seen. In dogs enterotoxigenic C. perfringens has also been associated with a syndrome of acute hemorrhagic gastroenteritis (HGE) accompanied by severe hemoconcentration. Infection can also cause diarrhea in groups of animals confined together and nosocomial outbreaks in hospitalized patients. Clostridial diarrhea is usually self-limiting after a few days, but in some patients diarrhea can persist chronically for weeks to months. Some patients have recurrent episodes of diarrhea.
Diagnosis
Routine hematologic and serum chemistry evaluations are usually normal in patients with clostridial diarrhea. Colonoscopy is not routinely necessary in these cases, but endoscopic findings are usually nonspecific (diffuse hyperemia, increased friability, fresh bleeding, and increased mucus). Biopsy results range from minimal abnormalities to catarrhal, lymphocytic-plasmacytic, or suppurative colitis.
A definitive diagnostic test for C. perfringens- induced diarrhea is lacking. Further work is needed to determine the role of CPE in canine and feline diarrhea and to define the optimal diagnostic parameters for clostridial diarrhea. Fecal spore counts in stained fecal smears are commonly used for routine cage-side screening; however, studies have not shown a correlation between spore counts and positive assays for CPE or a correlation between either of these diagnostic procedures and the presence or absence of diarrhea. In humans, fecal assays for CPE are considered more accurate than spore counts; however, the commercially available CPE assays used in humans need to be validated for dogs and cats. In principle, CPE assays should be valid across species.
The identification of more than five clostridial endospores per oil immersion field (identified by their “safety-pin” appearance with Diff-Quik or Wright's staining, see Chapter 6) is considered by many to be presumptive evidence for a diagnosis of enterotoxigenic diarrhea caused by C. perfrin- gens. Clostridial spores are generally larger than other bacilli found in feces. Malachite green can be used as a special stain for endospores. Fecal leukocytes also may be present. Unfortunately, the appearance or absence of clostridial spores in the feces does not correlate well with CPE assays or signs; thus it might be advisable to take into account spore counts, CPE assays, and clinical information before making a diagnosis of clostridial diarrhea.
Commercial fecal assays for C. perfringens enterotoxin are available in kit form as either an enzyme-linked immunosorbent assay (ELISA) or reverse passive latex agglutination (RPLA Kit).[§§§§] The ELISA assay is recommended as easier to use and interpret than the RPLA assay, and possibly more sensitive. It is recommended that fresh feces be used whenever possible and transported without delay to the laboratory in prechilled diluent at 4° C (but freezing should be avoided). Assays for CPE are generally considered to be more specific than fecal spore counts.
Cultures are not helpful because C. perfringens are normally found in the feces of most normal dogs and cats, and cultures do not reliably distinguish toxigenic and nontoxigenic strains. Assays using molecular probes and polymerase chain reaction are currently being evaluated as improved diagnostic procedures for enterotoxigenic C. per- fringens.
Treatment
Diarrhea caused by enterotoxigenic C. perfringens can be effectively treated with ampicillin (10 mg/lb orally every 8 hours), amoxicillin-clavulanate (6 to 12.5 mg/lb orally every 12 hours),tylosin (10 to 20 mg/lb orally every 12 hours), or clindamycin (2.5 to 5 mg/lb orally every 12 hours) for 5 to 7 days. Metronidazole (5 to 10 mg/lb orally every 12 hours) can also be effective but seems to work less consistently. Clostridial diarrhea is usually selflimiting or responsive to antibiotics in 2 to 3 days; however, chronic or recurrent clostridial diarrhea may require long-term antibiotics (e.g., tylosin once daily or every other day) and a fiber- supplemented diet to prevent relapses. Commercial fiber-containing diets or regular diets supplemented with psyllium (Metamucil; dogs: 1 to 2 tbsp/day) may help to reduce bacterial proliferation and sporulation because fiber is fermented to SCFAs that acidify bowel contents. Alkaline rather than acid conditions are most favorable for C. per- fringens. In addition, SCFAs nourish colonic epithelium and protect against injury.
Diarrhea Associated With Clostridium
Difficile
A severe form of pseudomembranous colitis in humans is caused by colonic overgrowth of cytotoxin-producing C. difficile, usually subsequent to suppression of the normal flora by antimicrobials or anticancer agents. Toxigenic C. difficile and its toxin have been isolated from normal dogs and cats and from a few patients with mild diarrhea; however, this organism does not appear to be significant as an enteropathogen in dogs and cats. C. difficile can be cultured using selective medium; however, infection can be established more rapidly by fecal PCR assay for the toxin gene or by latex agglutination assay of feces for toxin.
Mycotic Colitis
Histoplasma Colitis
Histoplasma capsulatum, a dimorphic soilborne fungus endemic to regions bordering the Mississippi River and its tributaries, primarily causes pulmonary and macrophage-monocyte system infection and occasionally intestinal tract infection. Widespread dissemination to virtually any tissue or organ system also can occur. The intestinal form of histoplasmosis occurs most often in young dogs and cats and is characterized by extensive transmural granulomatous inflammation of the bowel with mucosal ulceration and involvement of associated lymph nodes. The macrophages in these lesions contain Histoplasma organisms.
Intestinal histoplasmosis may be manifested as either small or large bowel diarrhea, or a combination of both when the disease is diffuse. Small bowel involvement is characterized by malabsorption syndrome and sometimes protein-losing enteropathy (see Chapter 7). When the colon is affected, severe bloody-mucoid large bowel diarrhea and tenesmus are seen. The disease is usually chronic, and associated signs may include fever, pallor, inappetence, lethargy, and progressive weight loss. Abdominal palpation may reveal diffuse thickening of the colon or small intestines, focal tumorlike (granulomatous) thickenings in the intestinal tract or mesentery, mesenteric lymphadenopathy, or abdominal effusions. When the rectum is involved, mucosal proliferations may be detected by digital palpation. Physical examination may also detect other extraintestinal sites of dissemination (e.g., liver, spleen, or eyes).
Histoplasmosis should be suspected in young patients in endemic areas with chronic intractable diarrhea. The results of diagnostics are variable but may reveal nonregenerative anemia, regenerative neutrophilia, monocytosis, and hypoproteinemia. Contrast radiography may demonstrate an irregular mucosal pattern indicative of a diffuse infiltrative lesion. Ultrasonography may reveal diffuse or focal thickening of the colon with associated lymphadenopathy. Colonoscopy usually reveals severe granulomatous ulcerative colitis. Definitive diagnosis depends on identification of Histoplasma organisms in cytologic preparations (rectal mucosal smears, colonic biopsy impressions, aspirates of lympħ nodes or abdominal masses), colonoscopic biopsy specimens, or cultures of feces or affected tissues on Sabourauds medium. In addition, serologic tests (immunodiffusion, complement fixation) tħat detect anti-Histoplasma antibodies can be used to establish a presumptive diagnosis; however, reliability of these tests is questionable because false-negative results are frequent.
Histoplasma colitis is progressive without treatment. Oral itraconazole (2.5 mg/lb orally every 12 hours) is the treatment of choice for histoplasmosis. Ketoconazole (5 mg/lb every 12 hours with food) can also be used as a more economical alternative, but it has less consistent efficacy and greater risk of side effects. Treatment with either of these antifungal drugs is continued for at least 2 to 3 months beyond remission, usually for a total of 4 to 6 months, while monitoring for hepatotoxicity. For symptomatic relief of colonic inflammation and tenesmus, 5-aminosalicylates (5-ASA) (e.g., sulfasalazine, olsalazine, mesalamine) can be administered as described later under treatment of idiopathic IBD.
Other Mycoses
Other than histoplasmosis, mycotic infections of the colon are rare; however, opportunistic fungi sometimes invade devitalized tissue (such as mucosa traumatized by passage of a foreign body) or infect young patients already compromised by predisposing factors such as immunodeficiency, malnutrition, preexisting debilitating illnesses (such as parasitism or parvovirus), or prolonged therapy with antimicrobials or corticosteroids. Opportunistic fungi can infect any portion of the intestinal tract of the dog and cat, and they include Candida albicans, Aspergillus sp., Pythium sp., and various fungi of the Zygomycetes class.
Both Aspergillus and Candida cause chronic diarrhea with mucosal ulceration and necrotizing lesions that extend into the deeper layers of the bowel wall. Pseudomembrane formation and vascular invasion by hyphae have been seen in cats with aspergillosis.
The term pythiosis is often used to designate GI infections caused by Pythium sp. and Zygomycetes. Pythiosis is most prevalent in the Gulf region of the United States, especially in young large-breed dogs, and it is characterized by extensive necrotizing transmural granulomatous inflammation of the bowel. The lesions may result in tumorlike thickening of the affected segment of the GI tract. The stomach, small intestines, and mesentery are most often affected; however, the colon is occasionally involved and may result in chronic bloody-mucoid large bowel diarrhea.
The antemortem diagnosis of any of these intestinal mycoses is difficult, usually requiring histologic identification of the fungi in colonic biopsy specimens. The branching hyphae of Aspergillus sp. or the sparsely septate hyphae of Pythium sp. and Zygomycetes are best demonstrated in tissue specimens by Gridley's or methenamine silver stains. Candida may form yeastlike cells or septate mycelia (pseudohyphae), which can be seen with fungal stains or Gram stain (gram-positive). Feces or biopsy specimens can be cultured on Sabouraud's medium for fungi, but this is slow and often unrewarding.
Most cases of intestinal aspergillosis and candidiasis have been diagnosed at necropsy; thus information on which to base treatment is limited. Treatment with oral itraconazole is suggested. Successful treatment of pythiosis is rare; thus the prognosis must be considered poor.When feasible, surgical excision of the severely involved segments of bowel with follow-up therapy using oral itraconazole or intravenous (IV) lipid-complexed amphotericin B is suggested.
Protothecal Colitis
Prototheca sp. are ubiquitous unicellular algae that may rarely colonize the lamina propria and submucosa of the intestinal tract of dogs and cause severe necrotizing or ulcerating enterocolitis. These algae appear to have a predilection for initially invading the colon, resulting in signs of chronic large bowel diarrhea with hematochezia. Typically the protothecal organisms then disseminate widely throughout the body and most frequently involve other visceral organs, the eyes, and the central nervous system (CNS). Only a cutaneous form has been described in cats.
Colonoscopy reveals thickened, corrugated mucosal folds, and the mucosa may be friable or ulcerated. Prototheca organisms can be identified in feces, cytologic preparations (Wright's or Gram stain), and biopsy specimens (Gomori's or PAS stain) as clusters of endosporulated ovoid structures (5 to 16 μm in length). Prototheca can also be cultured on Sabourauds cycloheximide-free dextrose medium. Successful treatment of systemic protothecosis in animals is rare. A combination of IV lipid-complexed amphotericin B with either itraconazole, ketoconazole, or tetracycline is suggested.
Chronic Idiopathic Colitis (Inflammatory Bowel Disease)
The terms chronic idiopathic colitis and inflammatory bowel disease (IBD) are generally used interchangeably to refer to a diverse group of chronic disorders characterized by diffuse infiltration of the colonic mucosa and sometimes submucosa with inflammatory cells. The types of colitis are classified histopathologically on the basis of the predominant infiltrating cells as lymphocytic-plasmacytic colitis, eosinophilic colitis, neutrophilic colitis, granulomatous colitis, and histiocytic ulcerative colitis. Thus definitive diagnosis depends on colonoscopic biopsy in conjunction with establishing the idiopathic nature of the condition. Sometimes there is a mixture of inflammatory cells in the lesion that makes classification difficult. The most common form of IBD in dogs and cats is lymphocytic- plasmacytic colitis. In some animals with IBD, infiltrative lesions may also involve the small intestines and/or stomach. It is unclear whether these are variants of the same disease process or not. Chronic idiopathic inflammatory diseases of the stomach and small bowel are discussed in Chapter 5 and 7, respectively.
The etiology of colitis (IBD) in dogs and cats is not determined in most cases, but genetic, dietary, bacterial, immunologic, and mucosal permeability factors have been implicated. The pathogenesis may involve altered mucosal permeability and a hypersensitivity response to antigens derived from food, intestinal bacteria, or the intestine itself. This may result either from a primary disorder of the intestinal immune system or its regulation or from immune events that occur secondary to mucosal injury and permeability. It has been suggested that chronic inflammation of the bowel becomes selfperpetuating when loss of mucosal integrity allows bacterial or dietary proteins to enter the lamina propria, where they act as antigens (or cross-react with self-antigens) that incite ongoing immune- mediated recruitment of inflammatory cells.
Most animals with IBD involving predominantly the colon have chronic or recurrent large bowel diarrhea; thus IBD must be differentiated from parasitic and infectious causes of colitis. Even though the cause of IBD is unknown, dietary manipulation and medical treatment are often effective in controlling the disease.
Lymphocytic-Plasmacytic Colitis
The most common form of IBD in both dogs and cats is characterized by diffuse infiltration of the lamina propria by lymphocytes and plasma cells in association with mucosal damage and abnormalities of mucosal epithelium and permeability. Idiopathic lymphocytic-plasmacytic IBD is generally considered to be the most common finding in dogs and cats evaluated for chronic vomiting and diarrhea. The stomach, small intestines, and colon may be involved separately or together. This discussion will focus on lymphocytic-plasmacytic colitis; the reader is referred to other chapters in this book for further information regarding IBD of the stomach and small intestine.
Etiology
The etiology of lymphocytic-plasmacytic IBD is unknown, but genetic, dietary, bacterial, immunologic, and mucosal permeability factors have been suggested to play a role. The disease involves either a primary disorder of the intestinal immune system or its regulation, or immune responses that occur secondary to mucosal injury and permeability. Chronic inflammation of the bowel may become self-perpetuating when loss of mucosal integrity and increased permeability allow bacterial or dietary proteins to enter the lamina propria, where they incite further immune reaction and inflammation.
In some cases this lesion can be associated with dietary hypersensitivity, enteric pathogens, or lymphoma. Some patients with lesions of lymphocytic-plasmacytic enterocolitis respond to protein elimination diets or antibiotics such as metronidazole or tylosin; however, in most patients lymphocytic-plasmacytic colitis is idiopathic.
Clinical Signs
The most frequent presenting clinical signs of lymphocytic-plasmacytic IBD are vomiting, diarrhea, and weight loss. The signs vary with the regions of the GI tract that are involved and the severity of mucosal infiltration and damage. The typical historical pattern is one of GI problems that wax and wane over periods ranging from a few weeks to several years. Animals of all ages are susceptible. Chronic intermittent vomiting is the most frequent sign of lymphocytic-plasmacytic IBD in cats. Colitis usually causes large bowel diarrhea characterized by increased frequency of defecation, urgency, tenesmus, increased fecal mucus, and hematochezia. Fecal consistency varies. Intermittent hematochezia without diarrhea may be the only sign of IBD. A change in defecation habits or loss of litter training without diarrhea can also occur. Physical examination is usually unremarkable, except for cachexia in severe cases. Intestinal loops can occasionally be palpably thickened and firm when the small intestine is involved. The literature reports some patients with concurrent food allergic dermatopathy, but this has been extremely rare in my experience.
Diagnosis
Precise criteria for the diagnosis of idiopathic lymphocytic-plasmacytic colitis have not yet been established. In general the clinical criteria for diagnosis are (1) chronic signs of colonic disease, (2) characteristic mucosal lesions of IBD in colonoscopic biopsy specimens, (3) failure to respond to dietary trials, and (4) exclusion of known causes of chronic inflammation of the intestinal tract based on thorough diagnostic evaluation. This last criterion emphasizes that IBD is a diagnosis of exclusion and not a catch-all label to be used as a substitute for diagnostic evaluation. Because lymphocytic-plasmacytic inflammation is a nonspecific lesion, only a thorough diagnostic work-up can establish that it is truly idiopathic and not merely an inflammatory response to an undiagnosed condition. A well-planned diagnostic approach could include routine fecal examinations (for parasites, C. perfrin- gens spores, Campylobacter, and fecal leukocytes), a therapeutic trial of fenbendazole for occult whipworm infection, elimination dietary trials, routine screening for extraintestinal disease (CBC, serum chemistry profile, urinalysis, retrovirus tests in cats, and baseline serum T4 level in cats over 5 years of age), abdominal imaging (radiography, ultrasonography), and colonoscopy with biopsy under anesthesia.
Laboratory Evaluations
Routine hematologic and serum biochemical parameters are normal in most patients with lymphocytic-plasmacytic colitis; however, some are found to have mild nonspecific laboratory abnormalities such as mild anemia, stress leuko- gram (mature neutrophilia, lymphopenia), stress hyperglycemia, mild hypoproteinemia (hypoal- buminemia, hypoglobulinemia, or both), and hypokalemia. Unexplained thrombocytopenia has been observed occasionally. Eosinophilia is occasionally found in cats. Cats with IBD often have mild-to-moderate elevations of serum liver enzymes (especially alanine aminotransferase), which in some cases is due to associated cholangiohepatitis and/or pancreatitis. Hypoproteinemia related to proteinlosing enteropathy sometimes is noted in dogs with small intestinal involvement but is rare in cats.
Radiography and Ultrasonography
In most cases radiographic and ultrasonographic findings are unremarkable and do not aid in diagnosis. Some patients have a nonspecific finding of fluid- and gas-distended bowel loops on plain abdominal radiography. Barium-contrast radiography occasionally demonstrates diffuse mucosal irregularity, and ultrasonography may reveal intestinal thickening, but these are nonspecific findings that merely suggest an infiltrative lesion. In selected cases contrast radiography and ultrasonography can be helpful nonetheless, because they may discover an unexpected diagnosis other than IBD, for example, pancreatitis, hepatobiliary disease, or intestinal tumors, polyps, granulomas, or malformations (e.g., diverticulum, short colon).
Endoscopic Examination
In patients with GI disease, the spectrum of clinical signs usually suggests the most appropriate region of the GI tract for endoscopic examination. In IBD, however, signs do not always correlate with the region of greatest cellular infiltration, especially in cats. It is not uncommon to find significant involvement of the colon in cats that present for vomiting. Conversely, cats with hematochezia or other colonic signs may have unexpected gastroduodenal lesions. Therefore it may be advisable in many cases to obtain biopsy specimens from the stomach, duodenum, jejunum (if possible), colon, and ileum (if the ileocolic sphincter can be navigated during colonoscopy).
Endoscopically the mucosa in colitis may appear to be normal or it may have any of the following abnormalities: erythema, petechiae, increased mucus, increased friability, increased surface granularity, decreased visibility of the submucosal vessels, thickened or increased folds, erosions/ulcers, or decreased distensibility. The mucosal lesions may be apparent only microscopically; thus a normal endoscopic appearance does not rule out IBD, and multiple biopsy specimens should be taken even if there are no endoscopically visible abnormalities.
Mucosal Histopathologic Examination
The histopathologic lesion of lymphocytic- plasmacytic IBD is characterized by diffuse infiltration of the lamina propria with mature lymphocytes and plasma cells in association with mucosal damage. In some cases the inflammation is mostly lymphocytic; in others the infiltrate also contains a mixture of other types of inflammatory cells (neutrophils, eosinophils, macrophages). The cellular infiltrate is usually confined to the mucosa but occasionally may extend to the submucosa. Additional findings indicative of mucosal damage include architectural distortion, fibrosis, and epithelial abnormalities (hyperplasia, degeneration, necrosis, erosion, ulceration, glandular dilation, loss of globlet cells). Pathologists may differ in their interpretation of endoscopic biopsy specimens and in their definition of how many lymphocytes and plasma cells within the lamina propria are too many. Infiltrates assessed to be minimal or mild by an inexperienced pathologist may not be truly abnormal. For definitive diagnosis of lymphocytic- plasmacytic colitis there must be abnormal infiltration of lymphocytes and plasma cells, as well as evidence of mucosal damage. Various grading systems have been proposed, but these have not correlated well with clinical disease activity. A severe infiltration of lymphocytes that extends beyond the mucosa into the submucosa and muscularis should raise the suspicion of early lymphoma mimicking IBD, and further diagnostics should be recommended.
Evaluation for Dietary Hypersensitivity
Dietary hypersensitivity or food allergy is an immunologically mediated adverse reaction to a protein component in food. A well-controlled dietary trial using a protein elimination diet is the basis for diagnosis of dietary hypersensitivity as a cause of IBD. The diet is changed to a well- defined, additive-free, highly digestible diet that contains a single source of protein not found in the patient's normal diet. Intake of all other foods or sources of antigen must be completely eliminated throughout the feeding trial, including table scraps, treats, and flavored medications such as vitamin supplements. The goal is to feed a single protein source to which the patient is not yet sensitized. Although many commercial hypoallergenic diets are available (see the section on treatment), home-prepared single-protein diets are preferred for diagnostic testing purposes. Examples of novel protein sources not likely found in the patient's regular diet might include turkey, duck, lamb, rabbit, venison, fish, or soybean (tofu). Once dietary hypersensitivity is confirmed with a home- prepared diet, commercial hypoallergenic diets can be substituted for more convenience for longterm management.
A cooperative and patient owner is required for a successful elimination diet trial. A minimum of 3 to 4 weeks should be allowed for initial response to an elimination diet. If no improvement has occurred during this time, then dietary hypersensitivity is unlikely and medical therapy should be instituted. If some improvement has been observed, then the trial should continue, because it may require 6 to 10 weeks before improvement is complete.
If there is a substantial improvement with the elimination diet, then the patient can be rechallenged with its original diet. Recurrence of clinical signs confirms dietary intolerance or hypersensitivity. In addition, once remission is restored with the controlled diet, the patient can then be challenged sequentially with individual dietary components to identify the specific offenders. To do this, individual components of the original diet are added one at a time to the controlled diet while the patient is in remission. With each challenge the patient is monitored for recurrence of signs for 7 to 10 days. If signs recur, then that substance is implicated as an offender.
After several weeks of remission of the controlled diet, some patients can be returned to their original diet and remain asymptomatic; but in most cases specially formulated or hypoallergenic diets may need to be continued indefinitely to prevent relapse. If there is no response to dietary management within 4 to 6 weeks, the patient can be returned to its original diet and medical therapy instituted.
Treatment
Well-controlled therapeutic trials for chronic colitis in animals are lacking; thus treatment is largely empirical and based on clinical experience. Because dietary hypersensitivity, parasites (see previous section), and bacterial enteropathogens (see previous section) may cause lymphocytic- plasmacytic colitis, it is appropriate to first consider evaluation and treatment for these possibilities. In most cases of lymphocytic-plasmacytic colitis an underlying cause cannot be identified and the most effective treatment is an antiinflammatory regimen of either a corticosteroid or mesalamine (5- aminosalicylate derivative) combined with dietary modification (e.g., novel protein diet or fiber- enriched diet). If diet and antiinflammatory drugs fail to control the disease, metronidazole is added for its antibacterial and immunomodulatory properties. Metronidazole can also be used as a single drug to induce or maintain remission in less severe cases. For the most refractory cases a cytotoxic immunosuppressive agent such as azathioprine is added to the corticosteroid regimen.
Dietary Therapy
Various strategies for dietary modification have been used for treatment of chronic colitis, including novel protein diets, fiber-enriched diets, and diets with adjusted omega-6 and omega-3 fatty acid levels. In some patients with IBD, dietary modification produces a complete or partial resolution of the signs and sometimes regression of the lesions. Potential explanations for a beneficial response to dietary modification include the effects of the diet on bowel motility, composition of the microflora, mucosal structure and function, and exposure to foodborne antigens or additives.
The treatment of IBD associated with dietary hypersensitivity is based on the controlled feeding of a well-defined, additive-free, highly digestible diet that contains a single source of protein not found in the patient's normal diet (i.e., a novel protein to which the patient is not yet sensitized). Home-prepared diets (turkey, duck, lamb, rabbit, venison, whitefish, or tofu) are most suitable for diagnostic testing purposes (see previous section on diagnosis); however, if the home-prepared diet suggests diet-responsive disease, then a commercial “hypoallergenic” novel protein diet can be substituted and is more convenient and balanced for long-term feeding. Many commercial diets that contain novel protein sources are now marketed for dietary hypersensitivity. A relapse rate of approximately 15% to 20% is to be expected when switching from a home-prepared to a commercial hypoallergenic diet. For long-term feeding of a home-prepared diet, recipes for balanced diets containing novel protein sources can be found in standard veterinary therapy and nutrition textbooks, or various reliable websites under supervision of Diplomates of the American College of Veterinary Nutrition.
In cases in which hypoallergenic novel protein diets have not been effective, other dietary adjustments may be beneficial as an adjunct to medical therapy for IBD. This includes fiber supplementation (psyllium, bran, canned pumpkin) of the regular diet or switching to a commercial diet enriched with fermentable fiber (e.g., beet pulp) marketed for improving colonic function and ameliorating diarrhea in patients with colitis. Fiber has many beneficial effects on colonic function and helps to keep enteropathogens in check. Colonic bacteria metabolize fermentable fiber to SCFAs that nourish colonic epithelium and protect against mucosal injury. Adjustment of the levels of omega-6 and omega-3 fatty acids in the diet has been proposed to manage bowel inflammation through decreasing inflammatory mediators, although evidence for this is lacking.
Corticosteroids
Oral prednisolone is the most consistently effective medical therapy (dogs: 0.5 to 1 mg/lb/day; cats: 1 to 2 mg/lb/day or 5 mg total dose every 12 hours) for inducing remission of idiopathic lymphocytic- plasmacytic colitis. Clinical improvement using this dosage should be noted within 1 to 2 weeks. After 2 weeks of remission, the dosage is tapered in 2- to 4-week increments to the lowest effective alternate-day dosage. In cats that are too difficult to medicate orally, periodic injections of methylprednisolone acetate (20 mg intramuscularly or subcutaneously every 2 to 4 weeks) may be substituted for oral treatment, or dermal preparations formulated by a compounding pharmacist may be applied topically. Corticosteroid therapy may be discontinued on a trial basis after 6 to 12 weeks of remission; however, continuous alternate-day therapy is often required to prevent relapse. In refractory cases metronidazole or mesalamine (see following sections) should be added to the prednisolone regimen. If this fails to control the disease, then the combination of azathioprine (see later section) and prednisolone may be more effective in achieving remission of the disease.
5-Aminosalicylic Acid
Derivatives of 5-ASA, also known as mesalamine, exert an antiinflammatory effect in colitis through local inhibition of mucosal leukotrienes and prostaglandins. Many gastroenterologists regard these as the initial drugs of choice for treatment of colitis, particularly in dogs. Orally administered 5-ASA derivatives are designed to be minimally absorbed during passage through the small intestine so that they reach the colon. These drugs should be used cautiously in cats because some salicylate absorption occurs and cats metabolize salicylates very slowly.
In sulfasalazine (Azulfidine), 5-ASA is combined with sulfapyridine by an azo bond that prevents significant absorption of the drug so that 75% of it reaches the colon, where colonic bacteria split the bond and release the 5-ASA for its local effect in the colon. Sulfasalazine dosages of 10 to 20 mg/lb (maximum of 1 g per dose) every 8 hours are used in dogs; 5 to 10 mg/lb every 12 hours or 250 mg total dose every 24 hours have been effective and relatively well tolerated in cats. The most common adverse side effect of sulfasalazine is keratoconjunctivitis sicca, which can be irreversible. For this reason it is recommended that a baseline Schirmer’s tear test be performed at the start of therapy and then monitored subsequently at monthly intervals if treatment is longterm. Less common side effects include allergic dermatitis, nausea and vomiting, and cholestatic jaundice. Rarely cats may develop anemia.
Newer formulations of 5-ASA include olsalazine (Dipentum) and polymer-coated mesalamine tablets (Asacol) and capsules (Pentasa). The advantages of these newer formulations over sulfasalazine are that a greater percentage of the drug (80% to 90%) reaches the colon and these formulations do not contain sulfapyridine so they have fewer side effects. Unfortunately, these products are much more expensive than sulfasalazine and they are not available in convenient dosage sizes for most patients. Safe and effective dosages remain to be determined. Sulfasalazine, olsalazine, or mesalamine can also be combined with corticosteroids or metronidazole to treat refractory colitis.
Metronidazole and Other Antibiotics
Low-dose metronidazole therapy (Flagyl, 5 to 7 mg/lb every 12 hours) is often beneficial either alone or in combination with prednisolone to treat IBD. The beneficial effects of metronidazole in any patient with diarrhea might be attributable to an antibacterial effect on enteropathogens (e.g., enterotoxigenic C. perfringens), an antiprotozoal effect (e.g., Giardia), a reduction of bacterial- derived antigens that could be involved in the immunopathogenesis of IBD, or the immunomodulating effect of the drug on cell-mediated immunity and neutrophil chemotaxis. Metronidazole tablets have an unpleasant taste and provoke salivation in most cats and sometimes vomiting. For ease of administration and accurate dosing, a liquid suspension can be formulated on request by many pharmacists or the tablets can be split and placed in gel capsules. Dosages of metronidazole exceeding 25 mg/lb/day for prolonged periods (weeks) occasionally cause signs of reversible CNS toxicity (ataxia, weakness, seizures). Other antibiotics that might be helpful to control intestinal microflora include tylosin or doxycycline (2.5 mg/lb every 12 hours).
Azathioprine
In IBD patients refractory to prednisone alone or in combination with metronidazole or mesalamine, the combination of azathioprine (Imuran) with prednisolone may be a more effective immunosuppressive regimen for producing remission of the disease. In addition to treating refractory IBD, the addition of azathioprine may enable use of a lower dose of corticosteroid to control the disease and thereby minimize steroidal side effects. Azathioprine is usually given as an alternate-day treatment (alternating with every-other-day prednisolone) at a dosage of 0.5 to 1 mg/lb orally in dogs and 0.15 to 0.25 mg/lb orally in cats. Azathioprine should be prepared as an oral suspension to facilitate accurate and safe dosing for cats. Because of its myelosup- pressive toxicity (leukopenia), the CBC should be monitored periodically, every 2 to 3 weeks for the first 2 months.
Future Possibilities for Immune Modulation in Colitis
Cyclosporine is a potent immunosuppressive drug (inhibits interleukin-2 and T-cell recruitment) and has shown promise in treating human IBD. New types of antiinflammatory drugs used to treat airway inflammation in asthmatics might find use in treating chronic GI inflammation as well. Zileuton (Zyflo) inhibits the formation of leukotrienes by inhibiting 5-lipoxygenase. Zafirlukast (Accolate) and montelukast (Singulair) are leukotriene receptor antagonists that reduce inflammatory cell influx. The effects of these so-called leukotriene blockers are comparable to steroids without steroidal side effects.
Eosinophilic Colitis
Eosinophilic colitis is an uncommon form of IBD that may occur alone or as part of a generalized syndrome of eosinophilic gastroenterocolitis. The lesion is characterized by segmental or diffuse infiltration of one or more layers of the colon with mature eosinophils, often accompanied by peripheral eosinophilia but not in all cases. Allergy and parasitism have been proposed as causes, but in most patients evidence for these is lacking and the disease must be considered idiopathic.
The colon may also be involved in the feline hypereosinophilic syndrome, in which there is widespread infiltration of eosinophils throughout the GI tract and in numerous extraintestinal tissues (see Chapter 7). Associated findings in cats with hypereosinophilic syndrome can include palpation of thickened intestinal loops, hepatosplenomegaly, lymphadenopathy, pulmonary infiltration, and bone marrow infiltration.
Transmural eosinophilic granulomas in the colon occasionally produce focal tumorlike thickenings or masses that can bleed and cause partial intestinal obstruction. Surgical excision is usually advisable.
Diagnosis
The clinical signs of eosinophilic colitis are typical of acute or chronic large bowel diarrhea. Hematochezia is common due to bleeding from mucosal ulceration. If the stomach and small intestine also are involved, vomiting and small bowel diarrhea also may be seen. The history may indicate dramatic responsiveness to prior corticosteroid therapy. The diagnosis is based on peripheral eosinophilia (although not present in all cases), lesions of eosinophilic inflammation in colonoscopic mucosal biopsy specimens, and the exclusion of underlying parasitism. The endoscopic appearance of the colon is similar to that described for lymphocytic-plasmacytic colitis, except mucosal ulceration is found more often in eosinophilic colitis.
Treatment
It is especially important to rule out occult whipworm or hookworm infection as a cause of eosinophilic colitis in dogs with a therapeutic trial of fenbendazole (22 mg/lb orally daily for 3 days). A larvacidal dose of ivermectin (100 mg/lb subcutaneously once) has been suggested to empirically treat for migrating larvae of Toxocara canis as a potential cause; however, the usual precautions for ivermectin should be taken, including avoidance of use in collies and related breeds.
Because eosinophilic gastroenteritis may potentially be due to food allergy, a feeding trial using an elimination or hypoallergenic diet (as described for lymphocytic-plasmacytic colitis) may be considered initially; however, dietary therapy alone has seldom been effective for eosinophilic colitis in my experience.
Most dogs and cats with idiopathic eosinophilic colitis respond rapidly to oral prednisolone at an initial dosage of 0.5 to 1 mg/lb/day for dogs and 1 to 2 mg/lb/day for cats. Once remission has been maintained for 2 weeks, this dosage is gradually tapered over an additional 2 to 4 weeks to the lowest effective maintenance dose. In some patients the treatment can eventually be discontinued, whereas in others alternate-day maintenance therapy is required. In some patients it may be necessary to add azathioprine to the corticosteroid regimen as described for lymphocytic-plasmacytic colitis to facilitate reduction of corticosteroid dosage and side effects or to provide more effective control of the disease.
Obstructing transmural eosinophilic granulomas involving a localized area of bowel should be surgically excised and treated with follow-up corticosteroid therapy. The prognosis for this atypical form of the disease is less favorable than for diffuse eosinophilic enterocolitis.
Neutrophilic (Suppurative)
Colitis
Some patients with signs of acute or chronic colitis have been found by colonoscopic biopsy to have an infiltrate of predominantly neutrophils without evidence of an infectious cause. Associated findings in some cases may include mucosal ulceration, necrosis, or crypt abscesses. These lesions should prompt an evaluation for the presence of bacterial enteropathogens. Too few patients with neutrophilic colitis have been characterized to draw conclusions; however, antibiotics (e.g., metronidazole and enrofloxacin or regimens consisting of sulfasalazine, mesalamine, or antiinflammatory-immunosuppressive drugs as discussed for lymphocytic-plasmacytic colitis (see Table 8-2) appear to be effective for controlling the disease.
Regional Granulomatous Colitis
Regional granulomatous colitis is a rare form of IBD characterized by transmural granulomatous inflammation that usually involves the ileum and colon and results in a stenosing, masslike thickening of a region of the bowel wall. In some dogs the granulomatous lesion also contains numerous eosinophils (eosinophilic granuloma). Regional granulomatous enterocolitis of animals is idiopathic and has been compared with human regional enteritis known as Crohn's disease; however, despite the resemblance, it is not known if these are related.
The principal clinical sign of regional granulomatous enteritis is chronic large bowel diarrhea containing mucus and fresh blood, sometimes accompanied by tenesmus and abdominal pain. Additional signs may include weight loss, anorexia, and depression. The diseased segment of bowel may be palpable as a firm mass in the midabdomen. The adjacent intestinal loops and mesentery also may be thickened, and regional lymph nodes may be enlarged. Rectal masses may be
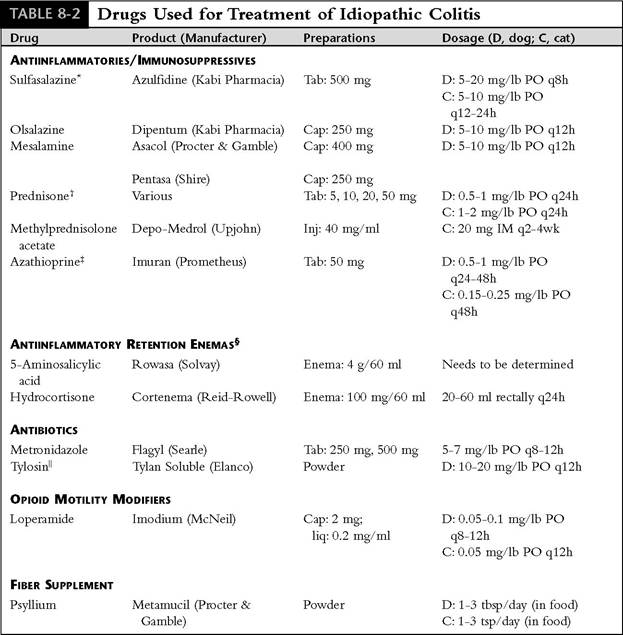
Tab, tablets; PO, orally; cap, capsules; inj, injectable.
*Sulfasalazine dosage may need to be increased to 25 mg/lb q8h to achieve effect in some dogs; may cause sicca in dogs and salicylate toxicosis in cats.
1In some cats with severe colitis, prednisone dosage may need to be increased to 2.3 mg/lb/day, divided bid. In dogs, if steroidal side effects become a problem, decrease the dosage and combine with azathioprine or metronidazole or both.
tAzathioprine may cause myelotoxicity, so monitor CBC; tablet can be crushed and compounded into a favorite liquid for accurate dosing of cats.
^Retention enemas for topical therapy of the distal colon may relieve signs of tenesmus and urgency in some patients with proctitis.
lTylosin powder is bitter tasting and thus best tolerated when mixed with food. It should be mixed in capsules for administration to cats.
identified by digital rectal palpation when this area is involved.
Diagnosis
Regional granulomatous colitis must be differentiated from intestinal neoplasia and from infectious causes of pyogranulomatous bowel lesions, such as histoplasmosis, pythiosis, and mycobacte- riosis. In cats FIP coronavirus can occasionally cause pyogranulomatous colitis manifesting as a large tumorlike mass. Barium contrast radiography or ultrasonography of the ileum and colon may delineate a thickened or stenosed segment of bowel. A routine CBC may reveal eosinophilia, neutrophilia, or monocytosis. Panhypoproteinemia due to chronic intestinal bleeding and protein loss may be found in some patients.
Definitive diagnosis of granulomatous colitis depends on biopsy by colonoscopy or laparotomy. Colonoscopic findings include thickened and corrugated folds, proliferative mucosal masses, ulceration, loss of distensibility, and partial obstruction. The key histopathologic feature is transmural granulomatous inflammation. Fibrosis and aggregates of epithelioid cells, giant cells, and eosinophils are often found deep in the lesion. Deep ulceration is common. Whenever granulomatous lesions are found in the bowel, infectious causes should be ruled out with special stains that identify fungi and acid-fast organisms. In cats polymerase chain reaction assay for detection of coronavirus in biopsy specimens should be considered.
Treatment
Medical treatment of regional granulomatous colitis is based on the use of antiinflammatory and immunosuppressive agents such as olsalazine or sulfasalazine, prednisone, azathioprine, and metronidazole, as described for treatment of lymphocytic- plasmacytic colitis (see Table 8-2). If the degree of thickening and cicatrization of the affected segment of bowel is producing severe stenosis and obliteration of the lumen, surgical excision of the lesion may be necessary. Surgery should be followed by long-term medical therapy for 6 to 8 weeks or longer to prevent recurrence of the lesion at the surgical site. The prognosis is guarded.
Histiocytic Ulcerative Colitis
Histiocytic ulcerative colitis is a chronic idiopathic IBD of young boxer dogs characterized by infiltration of the lamina propria and submucosa of the colon by distinctive histiocytes engorged with deposits that stain positive with PAS stain. A mixture of other types of inflammatory cells also is found in the lesion, and there is usually severe mucosal ulceration. Affected boxers generally develop a severe unresponsive bloody-mucoid large bowel diarrhea before 2 years of age. Colonoscopy reveals diffuse severe mucosal inflammation with corrugation, ulceration, bleeding, and thickened folds. Weight loss and moderate hypoproteinemia may occur in dogs with long-standing disease. The diagnosis is based on the known breed predisposition and the presence of numerous PAS-positive histiocytes in a colonoscopic biopsy specimen.
The disease is treated with olsalazine or sulfasalazine, prednisone, azathioprine, and metronidazole in single-agent or combination regimens as described for lymphocytic-plasmacytic colitis (see Table 8-2); however, lifetime therapy is needed and the prognosis for effective control of the disease is poor. In general these dogs seem to have less diarrhea on a highly digestible diet than on a high-fiber diet.
There have been isolated case reports of histiocytic colitis in a cat and a French bulldog, but it is not known if these represent the same disease as occurs in boxers.
Colitis Associated With Pancreatitis
Necrotizing hemorrhagic colitis occurs occasionally in dogs with acute pancreatitis. It is presumed that because the transverse colon lies adjacent to the inflamed pancreas, it can sometimes become secondarily involved in the local inflammatory and vascular-compromising processes in that region of the abdominal cavity.
The diagnosis is based on colonoscopic demonstration of lesions of colitis in the transverse colon in a patient that has laboratory, radiographic, and ultrasonographic evidence of pancreatitis. Olsalazine, sulfasalazine, or metronidazole can be added to the treatment regimen for pancreatitis, but corticosteroids should be avoided in acute pancreatitis.
Cecocolonic Intussusception (Cecal Inversion)
Cecocolonic intussusception results in invagination of the cecum into the lumen of the colon, where the mucosa of the inverted cecum then becomes congested, inflamed, hemorrhagic, and ulcerated. Whipworm infection has been suggested as a predisposing cause. With partial ileocolonic obstruction, chronic or intermittent bloody-mucoid diarrhea is usually the presenting sign; thus cecal inversion can often mimic colitis or colonic neoplasia. When cecal inversion causes complete ileocolic obstruction, the signs are acute depression, anorexia, vomiting, and dehydration.
The inverted cecum can sometimes be palpated as a firm, painful, right cranial abdominal mass, but usually the diagnosis is made by identification of the inverted cecum during colonoscopic examination of the proximal colon by ultrasonography or by demonstration of an intraluminal filling defect at the ileocolic junction on a barium contrast radiographic study. Surgical excision of the cecum is the treatment of choice.
Short Colon
Short colon, a malformation resulting from developmental errors in rotation and elongation of the embryonic gut, has been reported in both cats and dogs. The animals were diagnosed with colitis, and the malformation was apparently an incidental finding, although there had been a lifelong history of soft feces. Barium contrast radiography and colonoscopy revealed an abnormally short colon with absence of the ascending and transverse colons and location of the ileocolic junction and cecum in the left hemiabdomen at the proximal end of the descending colon. A digestible low- residue diet alleviated the soft feces.
Colonic Neoplasia
Colonic polyps and tumors usually cause hema- tochezia, dyschezia, and tenesmus, sometimes with mucoid diarrhea; thus they are easily confused with inflammatory diseases of the colon. Benign tumors, which include adenomatous polyps, adenomas, and leiomyomas, occur most commonly in the rectum and terminal colon of dogs. The most common malignant neoplasms of the colon are adenocarcinoma and lymphosarcoma. Carcinoid tumors, leiomyosarcoma, fibrosarcoma, hemangiosarcoma, and anaplastic sarcoma occur rarely. Metastasis to regional lymph nodes is common with all malignancies of the colon.
Adenocarcinomas are locally invasive and slow growing, and they occur primarily in older patients. There are three forms of adenocarcinoma: (1) the infiltrative type, which produces a thickened stenotic region of the colon that eventually obstructs the lumen; (2) the ulcerative type, which produces a deep indurated mucosal ulcer with raised edges; and (3) the proliferative type, which produces a lobulated mucosal mass.
Colonic lymphosarcomas usually cause a diffuse infiltration and thickening of the colon with mucosal ulceration and corrugation. Most colonic lymphomas occur in the descending colon and rectum of dogs younger than 4 years of age and at the ileocolic junction in cats older than 8 years of age.
Colonic neoplasia should be considered in any dog or cat with rectal bleeding or unresponsive large bowel diarrhea and hematochezia and therefore must be differentiated from colitis. Stenosing or polypoid rectal masses can usually be detected by digital rectal palpation. Most adenomatous polyps can be exposed at the anus by everting the rectal mucosa with gentle traction. Polyps usually appear dark red and lobulated, they are extremely friable, and they bleed easily. More proximal lesions, including most malignant colonic tumors, are identified by colonoscopy, ultrasonography, or barium contrast radiography. Biopsy is needed for definitive diagnosis. Colonoscopic biopsies can reveal the neoplastic cells in many cases, but in some patients the tissue obtained by the biopsy forceps is not adequate or deep enough for confirmation of the diagnosis. Surgical biopsy is then needed.
Surgical resection is the treatment of choice for benign tumors such as polyps and, when feasible, for adenocarcinomas. Excised tissue should always be submitted for thorough histopathologic examination. Unfortunately, most malignant tumors of the colon are too advanced for successful resection by the time they are recognized clinically. Some benign polypoid lesions recur months following excision as malignant (adenocarcinoma). Colonic lymphosarcoma may be treated with anticancer chemotherapy.
Colonic neoplasia is discussed in more detail in Chapter 11.
Irritable Bowel Syndrome
Irritable bowel syndrome (IBS) is characterized by noninflammatory, mucoid large bowel diarrhea associated with episodic disturbances of colonic myoelectrical function. Humans with an irritable colon seem to be hyperreactive to psychological and emotional stress and anxiety. Neurogenic pathways are presumably involved in the pathogenesis of the diarrhea and colonic dysfunction in IBS.
The clinical signs in humans with IBS are alternating patterns of diarrhea, constipation, and abdominal cramping. Evidence for the existence of IBS in animals is mostly circumstantial; thus it is a controversial topic in veterinary medicine. Nonetheless, it seems that a comparable syndrome exists at least in dogs with the most frequent clinical sign being intermittent mucoid diarrhea. Hematochezia is uncommon in IBS and should stimulate a search for other diagnoses. Large-breed dogs, especially those under stress as working dogs (e.g., police dogs, seeing eye dogs), and temperamental or excitable dogs may be predisposed to IBS.
The diagnosis of irritable bowel syndrome should be suspected primarily in dogs with chronic intermittent large bowel diarrhea when a thorough diagnostic evaluation, including colonoscopy, fails to identify a definitive cause. As a diagnosis of exclusion, IBS can be established only by normal colonoscopic biopsy and diligent exclusion of the other known causes of colonic disease such as dietary, parasitic, infectious, and idiopathic colitis (IBD). At colonoscopy the colon may appear to be hypermotile or spastic. The mucosa appears normal except for an erythematous response to insufflation and increased intraluminal mucus.
Treatment of IBS is based on dietary adjustment, motility-modifying drugs, and drugs that relieve anxiety or stress, such as various sedatives and psychotropic drugs. The initial approach should be to manage IBS with dietary modification alone. Supplement dietary fiber in the form of psyllium (Metamucil, 1 to 3 tbsp/day in the food), unprocessed wheat bran (1 to 5 tbsp/day), or a commercial high-fiber diet. Fiber-enriched diets can have a normalizing effect on colonic myoelectrical activity, thereby improving functional diarrhea in some dogs. If dietary fiber supplementation is unsuccessful, episodes of diarrhea can usually be controlled with a brief period of fasting and an opioid antidiarrheal drug such as loperamide (Imodium; dogs: 0.05 to 0.1 mg/lb orally every 8 to 12 hours; cats: 0.05 to 0.15 mg/lb orally every 24 hours). Once an episode has abated, loperamide can be discontinued and remission maintained by dietary and stress management. Stress management may require consultation from an animal behavior expert. Sedative and psychotropic drugs are used to produce anxiety relief and light sedation during stressful times. Standard dosages of benzodiazepines, acepro- mazine, chlorpromazine, or phenobarbital may be helpful in excessively nervous or excitable patients. Amitriptylin (Elavil, 0.5 to 1 mg/lb orally every 12 hours) has been highly effective in treating some dogs with IBS. The concept of “neurogenic inflammation” associated with stress may lead to new strategies for management of IBS in the future.