Feline gastrointestinal lymphoma
Epidemiology
Lymphoma is the most frequently diagnosed canine and feline cancer, and the most common GI neoplasm in both dogs and cats.1-5 There are several anatomical locations for lymphoma and the GI tract is regarded by some authors as the most common site in the cat.6-10 Gastrointestinal tract lymphoma accounts for 32% to 72% of total lymphoma cases.
However, other forms of lymphoma (i.e., leukemic, mediastinal, and multicentric) also have each been reported to be the most common form of lymphoma in cats by other authors.11-14 These discrepancies in the reported incidence of the various forms of lymphoma may be due to the differences in classification schemes used, a change in incidence over time, differences in FeLV subtypes in various geographical areas, and a decreased incidence of non-gastrointestinal forms since the introduction of a FeLV vaccine.15 The apparent increase in the proportion of GI location over time has been elucidated by comparing incidences in the same institutions over different time periods. For example, in the New England area, the proportion of lymphomas in cats that were classified as GI lymphomas increased from 8% in 1979, to 18% in 1983, and 32% in 1996.9,11,16 Likewise, in the NewYork City area, the proportion of GI lymphomas in cats increased from 27% in 1989 to 72% in 1995.8,14The association between FeLV and lymphoma in cats is well established. The incidence of FeLV antigenemia in cats with GI lymphoma ranges from 0% to 38%.10,13,17-21 However, such estimation of FeLV infection rate is significantly influenced by the method of testing. Underestimation of FeLV incidence with immunohistochemistry (IHC) versus PCR has been suggested.13 In one study, PCR testing detected FeLV viral nucleic acid sequences in up to 63% of cats with GI lymphoma, whereas only 38% of cats were positive using IHC.13 Generally, cats with leukemia or mediastinal lymphoma tend to be young and FeLV positive, while those with GI lymphoma are typically older and FeLV negative.6,10,16,17,20,21 An association between lymphoma and FIV has also been proposed.
Cats infected with FIV, FeLV, or both were determined to have 5.6, 62.1, and 77.3 times the relative risk of developing lymphoma respectively, when compared to retrovirus-negative cats.22Gross pathological findings
The gross appearance of feline GI lymphoma varies with the specific anatomical location. Many segments of the GI tract, including the liver, may be involved. There can be a focal mass or diffuse infiltration. In some cases, especially with low-grade lymphocytic lymphoma, the gross appearance may be normal. When a focal alimentary tract mass is present, there is usually transmural thickening, with or without mucosal ulceration
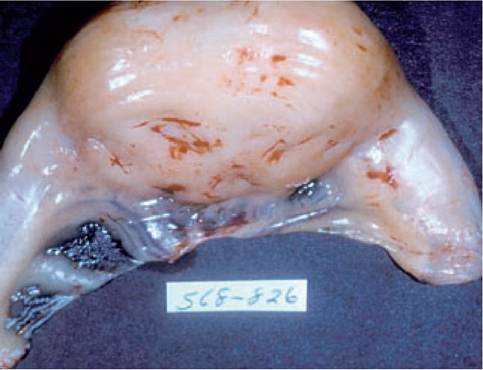
Figure 9.9:
Intestinal lymphoma. This figure shows a solitary mass located in the small intestine of a cat, which was diagnosed as a high-grade lymphoma on histopathology.

Figure 9.10:
Intestinal lymphoma. This figure shows the cut surface of the solitary mass shown in Figure 9.9.

Figure 9.11:
Hepatic lymphoma. Multifocal hepatic nodules in a cat with high-grade hepatic lymphoma.
(Figures 9.9 and 9.10). Mural thickening is often eccentric, resulting in preservation of the lumen, though a functional obstruction may develop (Figures 9.9 and 9.10). This contrasts with intestinal carcinoma, which frequently results in a mechanical obstruction due to a decreased luminal diameter, often appearing as a “napkin ring”. With diffuse infiltration, the intestinal wall may be visibly and /or palpably thickened. Mesenteric lymphadenopathy is usually overt, grossly or on ultrasonographic examination. Intussusception can develop secondary to intestinal lymphoma, with the jejunum being the most common location. In one study, lymphoma was associated with intussusception in seven of twenty cats (35%).23
Hepatic involvement can have a variable appearance.
In some cases, the liver appears to be grossly normal, whereas in others there may be an enhanced lobular pattern, a mottled appearance, or a gross nodular appearance (Figure 9.11).In summary, the appearance of lymphoma is extremely variable in all the regions of the GI tract. In light of how commonly this neoplasm develops in cats, lymphoma should be considered as a differential diagnosis in patients with normal or grossly abnormal organ appearance.
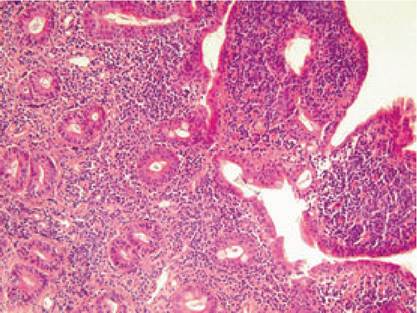
Figure 9.12:
Intestinal lymphoma. This image shows duodenal mucosa from a 14-year-old female Maine Coon cat presented for chronic diarrhea and weight loss. There is severe villous blunting and the lamina propria is infiltrated with monomorphic lymphocytes with large nuclei, typical of feline alimentary lymphoma. (H&E, magnification 200?; image courtesy of Dr. Thomas Bilzer, University of Dusseldorf, Germany.)
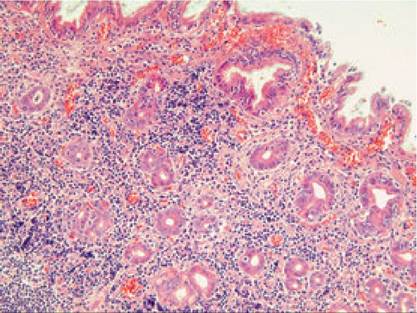
Figure 9.13:
Inflammatory bowel disease. This image shows duodenal mucosa from a 6-year- old female English Setter with chronic diarrhea. The villi are blunted, there are moderate epithelial lesions, and the propria is infiltrated severely by lymphocytes and plasma cells, intermingled with polymorphic granulocytes. The dog was diagnosed with IBD and was successfully managed for a period of more than 1 year by corticosteroid administration. (H&E, magnification 200 ?; image courtesy of Dr. Thomas Bilzer, University of Dusseldorf, Germany)
Histopathology and immunohistochemistry
There are different grades of GI lymphoma, commonly referred to as low-grade (lymphocytic or small cell), high-grade (lymphoblastic, immunoblastic, or large cell), and intermediate grade.24 Less common descriptions, such as large granular lymphocytic lymphoma also exist.25-28 Most published reports are of either undetermined grade or predominately highgrade lymphomas, although more recently low-grade lymphocytic lymphoma was described in a large case series.17,20,21 In the latter study, 50 of 67 cats (75%) diagnosed with GI lymphoma had low-grade, lymphocytic lymphoma.
The criteria used to classify lymphoma as lymphocytic have been described.17 However, these criteria have recently been questioned based on the difficulty in interpreting small endoscopic biopsies, the difference in opinion between pathologists, and a lack of characterization using immunohistochemical methods.29 Consequently, further studies are needed to define specific criteria for differentiating lymphocytic lymphoma, lymphocytic inflammation, and T-cell infiltrative disease, and to correlate such classifications with clinical outcome. While it is customary to consider that there is a continuum from IBD to lymphoma, there is little supporting data for this notion (Figures 9.12, 9.13, and 9.14).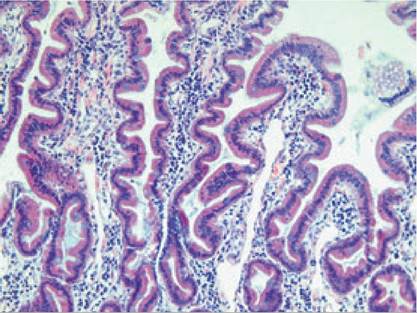
Figure 9.14:
Normal intestinal mucosa. Duodenal mucosa from a healthy 7-year-old female Labrador Retriever showing normal villi and mucosal texture and a mild lympho- plasmacytic infiltration of the propria. (H&E, magnification 200?; image courtesy of Dr. Thomas Bilzer, University of Dusseldorf, Germany)

Figure 9.15:
Small intestinal mass. This figure shows an ultrasonographic image of a focal small intestinal mass in a cat, which was diagnosed as lymphoma.
Recently, IHC has been used to better characterize feline lymphoma. Characterization of the normal feline small intestinal diffuse mucosal associated lymphoid tissue (MALT) has been described in SPF cats, and immunophenotyping has been applied to feline lymphomas.24,29-35 In some studies, intestinal lymphomas were more likely to be of B-cell rather than ofT-cell phenotype, whereas other studies describe a pre- dominantlyT-cell phenotype.21,24,29,33 Also, in a limited number of studies, the immunophenotype did not appear to correlate with response to chemotherapy treatment or survival.10,21,36 Thus, further study is necessary to determine the clinical value of immunophenotyping.
Clinical findings
Clinical signs and physical examination findings
Irrespective of the grade of GI lymphoma, the clinical signs include weight loss, anorexia, vomiting, diarrhea, lethargy, and polydipsia/polyuria. Importantly, many cats have minimal or no vomiting and/or diarrhea, with anorexia, weight loss, or both as the only historical findings.17,20 Therefore, when confronted with these signs in a geriatric cat with an otherwise unrewarding initial evaluation, GI lymphoma should be considered as a differential diagnosis. Physical examination findings may include poor body condition, thickened intestinal loops, and/or a palpable abdominal mass. The presence of an abdominal mass is more suggestive of high-grade lym- phoma.17,20 Notably, many cats may have a normal abdominal palpation.
Ancillary test findings
Laboratory findings are generally non-contributory, with mild anemia and /or hypoalbuminemia most commonly seen. Abnormalities on plain abdominal and thoracic radiographs are also uncommon and usually nonspecific. An abdominal ultrasound examination may be helpful in many cases, and is considered more sensitive than radiography.37,38 Lesions can be nodular (focal or multifocal) or diffuse.37 While the most common ultrasonographic abnormality observed is thickening of the gastric or intestinal wall, other important findings include loss of normal intestinal wall layering, a localized mass effect associated with the intestine (Figure 9.15), decreased intestinal wall echogenicity, regional hypomotility, regional lymphadenopathy, and ascites.18,37,38 Endoscopy can be an effective tool for diagnosing GI mucosal lymphoma in people, as well as in dogs and cats, when involved areas are within the endoscopic retrieval zones.17,39,40 In one study, endoscopy was performed in 61 of 67 cats with GI lymphoma, and was the main ancillary test leading to the definitive diagnosis, with a histological diagnosis reached in 56 cases.17 Most gross endoscopic findings are nonspecific, with considerable overlap with IBD and other GI diseases.
In many cases the endoscopic appearance can be grossly normal.Signalment
Treatment (Table 9.9)
Male cats appear to be predisposed to GI lymphoma.6,17,20,21 While a breed predilection is not apparent, most cats are DSH.17,18,20,21 The reported median age ranges from 9 to 13 years in different studies, with an age range spanning from 1 to 18 years.6,12,17-21
Reports of treatment strategies for feline GI lymphoma are fairly limited and only some of these reports give specific results for cats with GI lymphoma, but rather address the treatment of feline lymphoma in general.8,11,14,17,19-21,36 In addition, the outcome in different forms of GI lymphoma remains ill- defined because many reports do not describe the histological grades or the results of complete anatomical staging, and different combinations of chemotherapeutic agents were used in different studies.
| Primary | Number | Number Grade | Treatment | Percent | Median | Median | Overall | ||
| author | of cats | (and %) with | protocol | CR | remission | bgcolor=white>survival ofmedian | |||
| GI involvement | duration | those in CR | survival Time | ||||||
| Cotter11 | 7 | 7 (100) | NR | C, V, P | 86 | 19 weeks | NR | 26 weeks | |
| Jeglum19 | 14 | 14 (100) | NR | C,V,M | NR | NR | NR | 12 weeks | |
| Mooney14 | 103 | 28 (27) | NR | C,V,P,L | 62 | NR | 7 months | NR | |
| Mauldin8 | 132 | 95 (72) | NR | C,V,P,D,L,M | 67 | 21weeks | NR | 30 weeks | |
| Zwahlen21 | 21 | 21 (100) | NR | C,V,P,D,L,M | 38 | 20 weeks | 41.5 weeks | 40 weeks | |
| Malik36 | 60 | 14 (23) | NR | C,V,P,D,L,M | 80 | NR | 27 weeks | 17 weeks | |
| Mahony20 | 28 | 28 (100) | 89% HG, 11% LG | C,V,P | 32 | NR | NR | 7 weeks | |
| Fondacaro17 | 29 | 29 (100) | 100% LG | P,Cl | 69 | 20.5 months | 22.8 months | 17 months | |
| Fondacaro17 | 11 | 11 (100) | 100% HG | C,V,P or C,V,P,L,D | 18 | 18 months | 18 months | 11 weeks | |
CR = complete remission; NR = not reported; C = cyclophosphamide; V = vincristine; P = prednisone; M = methotrexate; L = L-asparaginase; D = doxorubicin; Cl = chlorambucil; HG = high grade; LG = low grade.
Cotter et al. described seven cats with GI lymphoma treated with cyclophosphamide, vincristine, and prednisone (CVP).11 Six cats achieved complete remission with a median remission duration of 19 weeks, and a median survival time of 26 weeks. Jeglum et al. reported 14 cats with GI lymphoma treated with cyclophosphamide, vincristine, and methotrexate.19 These cats had a median survival time of 12 weeks. Mooney et al. described 103 cats with lymphoma, of which 28 (27%) had GI lesions.14 These were treated with CVP plus L-asparaginase and methotrexate, with 62% achieving a complete remission for a median survival time of 7 months. Cats achieving partial and no remission had median survival times of 2.5 and
1.5 months, respectively. The specific response of cats with GI lymphoma was, however, not described. At the same institution, Mauldin et al. described 132 cats, of which 95 (72%) had a GI lesion.8 These cats were treated with CVP plus doxorubicin, methotrexate, and L-asparaginase. Sixty seven percent achieved a complete remission, with a 21-week disease- free interval. The overall median survival time was 30 weeks. Though the specific responses of those cats with GI lesions were not described, anatomical location was not found to be a prognostic factor in this study. Zwahlen et al. described 21 cats with GI lymphoma of unknown grade, treated with a similar protocol (CVP plus doxorubicin, L-asparaginase, and methotrexate).21 Of these cats, 38% achieved a complete remission, 57% a partial remission, and 5% had stable or progressive disease. The median disease-free interval was 20 weeks, and the median survival time 40 weeks. For those achieving a complete remission, the disease-free interval was 40 weeks, but the median survival was only 41.5 weeks. Sixty cats with lymphoma in Australia treated with a similar protocol achieved a median survival period of 17 weeks, and of 48 cats achieving a complete remission, the median survival was 27 weeks.36 Of these 48 cats, only 14 had GI lesions. Four of the fourteen cats (29%) survived for longer than one year. Mahony et al. described 28 cats, 25 of whom had high-grade GI lymphoma, treated with CVP.20 The overall median survival time was only 7 weeks, whereas the median disease-free interval of those achieving a complete remission (32%) was 30 weeks. These findings are in agreement with those of Fondacaro et al., who described 11 cats with high-grade lymphoma treated with CVP or CVP with doxorubicin and L-asparaginase, where only 18% achieved a complete remission (both cats that responded received doxorubicin), with a median survival of 11 weeks.17 Other chemotherapy agents have not been extensively studied in cats with GI lymphoma. In a phase 1 trial of the oral alkylating agent lomustine (CCNU), two of six cats with GI lymphoma had only a partial response.41
These findings contrast with those of cats having low-grade lymphoma. Fondacaro et al. described 50 cats with low-grade GI lymphoma, 36 of which were treated with chemotherapy.17 Twenty-nine cats with lymphocytic lymphoma were treated with prednisone (10 mg/cat/day) and high-dose pulse chlorambucil (Leukeran®; 15 mg/m2 of body surface area, orally, once daily for 4 days, repeated every 3 weeks). Sixty-nine percent of the cats achieved a complete clinical remission, with a median disease-free interval for cats that achieved complete remission of 20.5 months (range: 5.8-49.0 months). The median survival time for all cats was 17 months (range: 0.350.0 months), with a median survival time of 22.8 months for cats that achieved complete remission (range: 10.050.0 months). Twelve of the twenty cats that achieved a complete remission were “rescued” with cyclophosphamide at a dosage of 225 mg/m2 of body surface area, orally, every three weeks. These cats had a median disease-free interval of 24 months and a median survival time of 29 months. Seven cats were alive at the time of data collection; all but one of
these cats had received a rescue treatment with cyclophosphamide. Adverse reactions to chlorambucil or cyclophosphamide were rare, but included vomiting, diarrhea, anorexia, lethargy, and neutropenia. None of the affected cats required hospitalization or discontinuation of therapy.
Some conclusions and recommendations can be made from these studies. In general, response to chemotherapy for highgrade GI lymphoma is poor, whereas the clinical response for low-grade lymphoma is good. For cats with high-grade GI lymphoma, combining doxorubicin with other agents in a multi-agent protocol, such as CVP and L-asparaginase is associated with longer remission and survival times, when compared with single-agent doxorubicin or CVP alone. For cats with low-grade lymphoma, excellent results can be achieved with oral prednisone and high-dose pulse chlorambucil ther- apy.17 However, it is unknown whether these cats would do better with a more aggressive multi-agent protocol. Lastly, chemotherapy is generally well tolerated by cats. Self-limiting anorexia, vomiting, diarrhea, and myelosuppression may be observed in some patients. It may also be difficult to distinguish some of these chemotherapy-related side effects from active or progressive lymphoma.
The role of surgery in the treatment of GI lymphoma has been discussed previously.17,20,21,36 These studies have shown either no effect or a negative effect of surgical intervention on disease-free interval and survival. However, this effect is most likely not due to the surgical intervention itself, but is more likely due to the fact that cats requiring surgery (i.e., those with GI obstruction) have shorter survival periods due to the severity of their disease. The main indications for surgery are partial or complete intestinal obstruction, intestinal perforation, or to obtain biopsy specimens for a definitive diagnosis.
It is believed that some patients with transmural focal disease are at risk for perforation when treated with cytotoxic chemotherapy that induces a rapid response. Surgery may result in dehiscence at intestinal anastomosis sites, and may require a delay in the initiation of chemotherapy to allow proper wound healing. Following resection of a focal GI or mesenteric mass, chemotherapy is still warranted since most cases have diffuse or multifocal microscopic involvement and lymphoma can be considered a systemic disease in most cases.
Prognostic factors
Few prognostic factors have been described for cats with GI lymphoma. Fondacaro et al. reported that histological grade was a strong indicator of outcome.17 Compared to cats with high-grade lymphoma treated with a multi-agent chemotherapy regimen, cats with low-grade lymphoma treated with oral prednisone and chlorambucil had a significantly better remission rate (69% versus 18%) and survival time (17.0 months versus 2.7 months). Since other studies did not compare low- grade and high-grade lymphomas, this finding has not been further verified. Low-grade and high-grade GI lymphomas in many ways represent different disease entities, and must be considered separately. Thus, statements about feline GI lymphoma may in some cases be overly generalized.
In the majority of studies, the most significant prognostic indicator for a positive outcome was initial response to chemo- therapy.7,8,10,14,17,20,21,36 In general, cats that survive the initial induction period and achieve remission generally also have a better long-term outcome. Though this may seem intuitively obvious, it may give clinicians and owners encouragement to continue chemotherapy treatment in cats that attain a complete remission. Otherwise there is no consistent association with any patient or tumor characteristic that is predictive of outcome (including sex, immunophenotype, clinical stage, age, and body weight). In most recent studies, FeLV virus anti- genemia was not found to be a negative prognostic fac- tor.8,20,21,36 Some studies also showed little benefit of an exhaustive “staging evaluation”, since very few factors have enough of an impact on prognosis to make their determination helpful.8,20,21,36
Recently, investigators have looked at molecular markers as prognostic factors. However, argyrophilic nucleolar organizer region (AgNOR) frequency and proliferating cell nuclear antigen labeling index (PCNA-LI) showed no correlation with response to chemotherapy or survival.10,42 Similarly, the immunophenotype of tumor cells also does not seem to correlate with outcome in cats.10,21,36 This is in contrast to dogs, where a T-cell phenotype has long been recognized as a negative prognostic factor for response to therapy and survival. Concentration of serum alpha1-acid glycoprotein, an acute phase protein, has recently been evaluated in cats with lymphoma, and was not shown to be useful in predicting the response to treatment or survival.43 The limitations of many studies published include incomplete staging, inconsistent grading, multiple non-sampled GI locations, lack of prospective randomization to different chemotherapy protocols, lack of control (untreated) patients, and lack of confirmation of remission through follow-up biopsies. Prospective, controlled, and randomized cohort studies with large numbers of cats aimed at investigating the response of each grade of GI lymphoma to single agent chemotherapeutic regimens seem warranted. Furthermore, additional studies to correlate clinical outcome with immunophenotyping and molecular markers are needed.
9.3.5