Feline megacolon
Robert J. Washabau
Etiology
The etiopathogenesis of idiopathic megacolon in the cat is still incompletely understood. Several reviews have emphasized the importance of considering an extensive list of differential diagnoses (e.g., neuromuscular, mechanical, inflammatory, metabolic/endocrine, pharmacological, environmental, and behavioral causes) for the obstipated cat (Table 6.1).1 A review of published cases suggests that 96% of cases of obstipation are accounted for by idiopathic megacolon (62%), pelvic canal stenosis (23%), nerve injury (6%), or Manx sacral spinal cord deformity (5%).2 It is important to consider an extensive list of differential diagnoses in an individual animal, but it should be kept in mind that most cases are idiopathic, orthopedic, or neurological in origin.
Pathophysiology
Megacolon develops through two pathological mechanisms: dilation and hypertrophy. Dilated megacolon is the end stage of colonic dysfunction in idiopathic cases. Cats affected with idiopathic dilated megacolon have a permanent loss of colonic structure and function. Medical therapy may be attempted in such cases, but most affected cats eventually require colectomy. Hypertrophic megacolon, on the other hand, develops as a consequence of obstructive lesions (e.g., malunion of pelvic fractures, tumors, or foreign bodies). Hypertrophic megacolon may be reversible with early pelvic osteotomy or it may progress to irreversible dilated megacolon if appropriate therapy is not instituted.
Constipation and obstipation are earlier manifestations of the same problem.3 Constipation is defined as the infrequent or difficult evacuation of feces, but does not necessarily imply a permanent loss of function. Many cats suffer from one or two episodes of constipation without further progression. Intracta-
Table 6.1: Differential diagnoses for constipation in the cat
Neuromuscular dysfunction
■ Colonic smooth muscle: idiopathic megacolon, aging
■ Spinal cord disease: lumbosacral disease, cauda equina syndrome, sacral spinal cord deformities (Manx cat)
■ Hypogastric or pelvic nerve disorders: traumatic injury, malignancy, dysautonomia
■ Submucosal or myenteric plexus neuropathy: dysautonomia, aging
Mechanical obstruction
■ Intraluminal: foreign material (bones, plant material, hair), neoplasia, rectal diverticula, perineal hernia, anorectal strictures
■ Intramural: neoplasia
■ Extraluminal: pelvic fractures, neoplasia
Inflammation
■ Perianal fistula, proctitis, anal sac abscess, anorectal foreign bodies, perianal bite wounds
Metabolic and endocrine
■ Metabolic: dehydration, hypokalemia, hypercalcemia
■ Endocrine: hypothyroidism, obesity, nutritional secondary hyperparathyroidism
Pharmacological
■ Opioid agonists, cholinergic antagonists, diuretics, barium sulfate, phenothiazines
Environmental and behavioral
■ Soiled litter box, inactivity, hospitalization, change in environment
ble constipation that has become refractory to control is referred to as obstipation and implies a permanent loss of function.
A cat is assumed to be obstipated only after several consecutive treatments have failed. Recurring episodes of constipation or obstipation may culminate in the syndrome of megacolon.The pathogenesis of idiopathic dilated megacolon appears to involve the functional disturbance of colonic smooth muscle. In-vitro isometric stress measurements have been performed on colonic smooth muscle obtained from cats with idiopathic dilated megacolon.4,5 These studies initially suggested that the disorder of feline idiopathic megacolon is a generalized dysfunction of colonic smooth muscle, and that treatments aimed at stimulating colonic smooth muscle contraction might improve colonic motility. More recent studies suggest that the lesion may begin in the descending colon and progress to involve the ascending colon over time.6
Clinical history
Constipation, obstipation, and megacolon may be observed in cats of any age, sex, or breed; however, most cases are observed in middle-aged (mean = 5.8 years), male cats (70% male, 30% female) of DSH (46%), Domestic Longhair (15%), or Siamese (12%) breeding.2 Affected cats are usually presented for reduced, absent, or painful defecation for a period of time ranging from days to weeks or months. Some cats are observed making multiple, unproductive attempts to defecate in the litter box, while other cats may sit in the litter box for prolonged periods of time without assuming a defecation posture. Dry, hardened feces are observed inside and outside of the litter box. Occasionally, chronically constipated cats have intermittent episodes of hematochezia or diarrhea due to mucosal irritation caused by fecal concretions. This may give the pet owner the erroneous impression that diarrhea is the primary problem. Prolonged inability to defecate may result in other systemic signs, including anorexia, lethargy, weight loss, and vomiting.
Clinical presentation
Colonic impaction is a consistent physical examination finding in affected cats.
Other findings will depend on the severity and pathogenesis of constipation. Dehydration, weight loss, debilitation, abdominal pain, and mild to moderate mesenteric lymphadenopathy may also be observed in cats with severe idiopathic megacolon. Colonic impaction may be so severe as to render it difficult to differentiate impaction from colonic, mesenteric, or other abdominal neoplasia. Cats with constipation due to dysautonomia may have other signs of autonomic nervous system failure, such as urinary and fecal incontinence, regurgitation due to megaesophagus, mydriasis, decreased lacrimation, prolapse of the nictitating membrane, and bradycardia.Diagnosis
Digital rectal examination should be carefully performed with sedation or anesthesia in all cats. Pelvic fracture malunion may be detected on rectal examination in cats with pelvic trauma. Rectal examination might also identify other unusual causes of constipation, such as foreign bodies, rectal diverticula, strictures, inflammation, or neoplasia. Chronic tenesmus may be associated with perineal herniation in some cases. A complete neurological examination with special emphasis on caudal spinal cord function should be performed to identify neurological causes of constipation, e.g. spinal cord injury, pelvic nerve trauma, and Manx sacral spinal cord deformity.
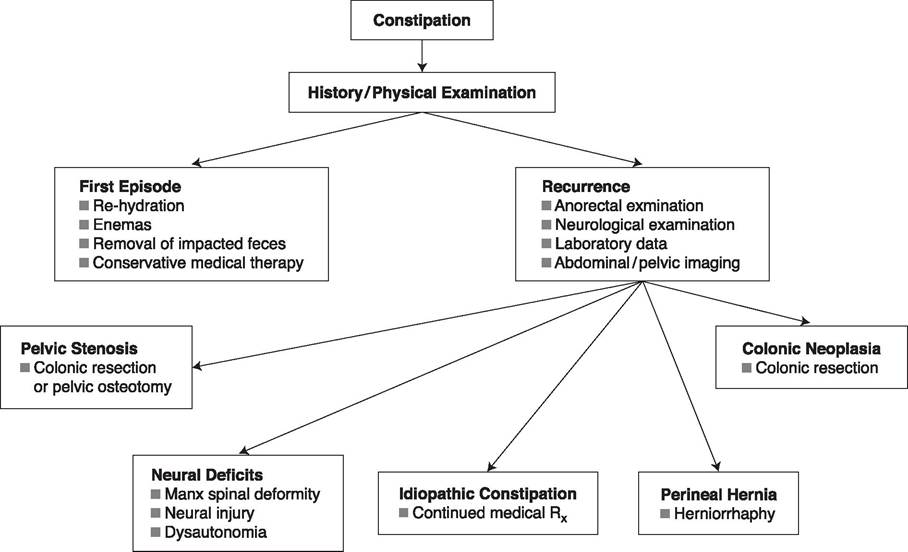
Figure 6.10:
Constipation. This figure shows a systematic work-up for a cat presented for constipation.
While most patients with obstipation and megacolon are unlikely to have significant changes in laboratory data (e.g., CBC, serum chemistry, and urinalysis), these tests should nonetheless be performed in all cats presented for constipation (Figure 6.10). Metabolic causes of constipation, such as dehydration, hypokalemia, and hypercalcemia may be detected in some cases. Though hypothyroidism is a rare cause of constipation in cats, basal serum T4 concentration and other thyroid function tests should also be considered in cats with additional signs consistent with hypothyroidism.
Constipation could theoretically also develop following successful treatment of feline hyperthyroidism.Abdominal radiography should be performed in all constipated cats to characterize the severity of colonic impaction, and to identify predisposing factors such as intraluminal radioopaque foreign material (e.g., bone chips), intraluminal or extraluminal mass lesions, pelvic fractures, and spinal cord abnormalities. The radiographic findings of colonic impaction cannot be used to distinguish between constipation, obstipation, and megacolon in idiopathic cases. The first or second episodes of constipation in some cats may be severe and generalized but may still resolve with appropriate treatment.
Ancillary studies may be indicated in some cases. Extraluminal mass lesions may be further evaluated by abdominal ultrasonography and ultrasound-guided biopsy, whereas intraluminal mass lesions are best evaluated by endoscopy. Colonoscopy may also be used to evaluate the colon and anorectum for suspected inflammatory lesions, strictures, sacculations, and diverticula. Barium enema contrast radiography may be used if colonoscopy is not possible. Both colonoscopy and barium enema contrast radiography will require general anesthesia and evacuation of impacted feces. Cerebrospinal fluid analysis, CT or MRI, and electrophysiological studies should be considered in animals with evidence of neurological impairment. Finally, colonic biopsy or anorectal manometry will be necessary to diagnose suspected cases of aganglionic megacolon.
Treatment
The specific therapeutic plan will depend upon the severity of constipation and the underlying cause.1 Medical therapy may not be necessary with first episodes of constipation. First episodes are often transient and resolve without therapy. Mild to moderate or recurrent episodes of constipation, on the other
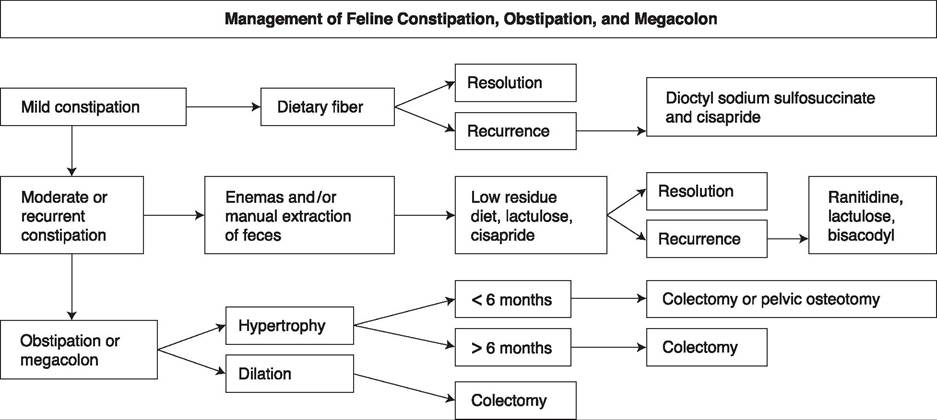
Figure 6.11:
Management of feline obstipation, constipation, and megacolon.
hand, usually require some medical intervention. These cases may be managed, often on an outpatient basis, with dietary modification, water enemas, oral or suppository laxatives, and/ or colonic prokinetic agents. Severe cases of constipation usually require brief periods of hospitalization to correct metabolic abnormalities and to evacuate impacted feces using water enemas, manual extraction of retained feces, or both. Follow-up therapy in such cases is directed at correcting predisposing factors and preventing recurrence. Subtotal colectomy will become necessary in cats suffering from obstipation or idiopathic dilated megacolon. These cats, by definition, are unresponsive to medical therapy. Pelvic osteotomy without colectomy may be sufficient for some cats suffering from pelvic canal stenosis and hypertrophic megacolon.7 An algorithm for the therapeutic approach to the constipated, obstipated, and megacolonic cat is outlined in Figure 6.11.
Removal of impacted feces
The removal of impacted feces may be accomplished through the use of rectal suppositories, enemas, or manual extraction.
Rectal suppositories. A number of pediatric rectal suppositories are available for the management of mild constipation. These include dioctyl sodium sulfosuccinate (emollient laxative), glycerin (lubricant laxative), and bisacodyl (stimulant laxative).
Table 6.2: Index of pharmaceutical agents for constipation
Drug class Examples
Rectal ■ Bisacodyl (Dulcolax, Boehringer Ingelheim)
Suppositories ■ Dioctyl sodium sulfosuccinate (Colace, Mead Johnson)
■ Glycerine
Enemas ■ Warm tap water
■ Warm isotonic saline
■ Dioctyl sodium sulfosuccinate (Colace, Mead Johnson)
■ Dioctyl sodium sulfosuccinate (Disposaject, PittmanMoore)
■ Lactulose (Cephulac, Merrell Dow; or Duphalac, Reid Rowell)
■ Mineral oil
Oral ■ Bulk laxatives
Laxatives - Canned pumpkin
- Coarse wheat bran
- Psyllium (Metamucil, Searle)
■ Emollient laxatives
- Dioctyl calcium sulfosuccinate (Surfax, Hoechst)
- Dioctyl sodium sulfosuccinate (Colace, Mead Johnson)
■ Lubricant laxatives
- Hyperosmotic laxatives
- Lactulose (Cephulac, Merrell Dow; or Duphalac, Reid Rowell)
- Mineral oil
- Petrolatum (Laxatone; Evsco)
■ Stimulant laxatives
- Bisacodyl (Dulcolax; Boehringer Ingelheim)
Prokinetic ■ Cisapride (compounding pharmacies)14 agents ■ Nizatidine (Axid; Eli Lilly)
■ Ranitidine (Zantac; Glaxo SmithKline)
Enemas. Mild to moderate or recurrent episodes of constipation may require administration of enemas and/or manual extraction of impacted feces.
Several types of enema solutions may be administered, such as warm tap water (5-10 mL/kg), warm isotonic saline (5-10 mL/kg), dioctyl sodium sulfosuccinate (5-10 mL/cat), mineral oil (5-10 mL/cat), or lactulose (5-10 mL/cat). Enema solutions should be administered slowly with a well-lubricated 10-12 F rubber catheter or feeding tube. Enemas containing sodium phosphate are contraindicated in cats because of their propensity for inducing severe hypernatremia, hyperphosphatemia, and hypocalcemia in this species.Manual extraction. Cases unresponsive to enemas may require the manual extraction of impacted feces. Cats should be adequately rehydrated and then anesthetized with an endotracheal tube in place to prevent aspiration should colonic manipulation induce vomiting. Water or saline is infused into the colon while the fecal mass is manually reduced by abdominal palpation. Sponge forceps may also be introduced with caution rectally to break down the fecal mass. It may be advisable to evacuate the fecal mass over a period of several days to reduce the risks of prolonged anesthesia and perforation of a devitalized colon.
Laxative therapy
Laxatives promote evacuation of the bowel through the stimulation of fluid and electrolyte transport or an increase in propulsive motility. They are classified as bulk-forming, emollient, lubricant, hyperosmotic, or stimulant laxatives according to their mechanism of action. There are literally hundreds of products available for the treatment of constipation. Table 6.2 summarizes those products that have been used with some success in cats.
Bulk-forming laxatives. Most of the available bulk-forming laxatives are dietary fiber supplements of poorly digestible polysaccharides and celluloses derived principally from cereal grains, wheat bran, and psyllium.8 Fiber-supplemented diets are available commercially, or the pet owner may wish to add psyllium (1-4 teaspoons per meal), wheat bran (1-2 tablespoons per meal), or pumpkin (1-4 tablespoons per meal) to canned cat food. Cats should be well hydrated before commencing fiber supplementation to maximize the therapeutic effect. Fiber supplementation is most beneficial in mildly constipated cats, prior to the development of obstipation and megacolon. In obstipated and megacolon cats, fiber may in fact be detrimental and low residue diets may be more beneficial in cats with these conditions.
Emollient laxatives. Emollient laxatives are anionic detergents that increase the miscibility of water and lipid in ingesta, thereby enhancing lipid absorption and impairing water absorption. Dioctyl sodium sulfosuccinate and dioctyl calcium sulfosuccinate are examples of emollient laxatives available in oral and enema form. Anecdotal experience suggests that dioctyl sodium sulfosuccinate therapy may be most useful in animals with acute but not chronic constipation. As with bulkforming laxatives, animals should be well-hydrated before emollient laxatives are administered. It should be noted that the clinical efficacy has not been definitively established for emollient laxatives. Dioctyl sodium sulfosuccinate, for example, inhibits water absorption in isolated colonic segments in vitro, but it may be impossible to achieve tissue concentrations great enough to inhibit colonic water absorption in vivo. Further studies are required to determine the clinical efficacy and therapeutic role of dioctyl sodium sulfosuccinate in the management of the constipated cat.
Lubricant laxatives. Mineral oil and white petrolatum are the two major lubricant laxatives available for the treatment of constipation. The lubricating properties of these agents impede colonic water absorption as well as permit greater ease of fecal passage. These effects are usually moderate, however, and, in general, lubricants are beneficial only in mild cases of constipation. Mineral oil usage should probably be limited to rectal administration because of the risk of aspiration pneumonia with oral administration, especially in depressed or debilitated cats.
Hyperosmotic laxatives. This group of laxatives consists of the poorly absorbed polysaccharides (e.g., lactose or lactulose), the magnesium salts (e.g., magnesium citrate, magnesium hydroxide, or magnesium sulfate), and the polyethylene glycols. Lactose is not effective as a laxative agent in all cats.12 Lactulose is the most effective agent in this group. The organic acids produced from lactulose fermentation stimulate colonic fluid secretion and propulsive motility. Lactulose administered at a dosage of 0.5 mL/kg body weight PO q 8-12 h fairly consistently produces soft feces in the cat. Many cats with recurrent or chronic constipation have been well managed with this regimen of lactulose. The dosage may have to be tapered in individual cases if flatulence and diarrhea become excessive. Magnesium salts are not currently recommended in the treatment of feline constipation and idiopathic megacolon. Some veterinarians have reported anecdotal successes with the polyethylene glycols.
Stimulant laxatives. The stimulant laxatives (bisacodyl, phenolphthalein, castor oil, cascara, and senna) are a diverse group of agents that have been classified according to their ability to stimulate propulsive motility. Bisacodyl, for example, stimulates nitric oxide-mediated epithelial cell secretion and myenteric neuronal depolarization. Diarrhea results from the combined effect of increased mucosal secretion and colonic propulsion. Bisacodyl, at a dosage of 5 mg per cat PO q 24 h, is the most effective stimulant laxative in the cat. It may be given individually or in combination with fiber supplementation for the long-term management of constipation. Daily
administration of bisacodyl should probably be avoided, however, because of injury to the myenteric neurons with chronic usage.
Colonic prokinetic agents
Previous studies of feline colonic smooth muscle function have suggested that stimulation of colonic smooth muscle contraction might improve colonic motility in cats affected with idiopathic dilated megacolon.4,5,9 Unfortunately, many of the currently available GI prokinetic agents have not proved useful in the therapy of feline constipation, either because of significant side effects (e.g., bethanechol) or because the prokinetic effect is limited to the proximal GI tract (e.g., metoclopramide, domperidone, or erythromycin). The 5-HT4 serotonergic agonists (e.g., cisapride, prucalopride, tegaserod, and mosapride) appear to have the advantage of stimulating motility from the gastroesophageal sphincter to the descending colon with relatively few side effects.10 Cisapride, for example, increases gastroesophageal sphincter pressure, promotes gastric emptying, and enhances small intestinal and colonic propulsive motility. Cisapride enhances colonic propulsive motility through the activation of colonic neuronal or smooth muscle 5-HT receptors in a number of animal species.11,12 In vitro studies have shown that cisapride stimulates feline colonic smooth muscle contraction, although it has not yet been conclusively shown that cisapride stimulates feline colonic propulsive motility in vivo.5,12 A large body of anecdotal experience suggests that cisapride is effective in stimulating colonic propulsive motility in cats affected with mild to moderate idiopathic constipation; cats with long-standing obstipation and megacolon are not likely to show much improvement with cisapride therapy. Cisapride was widely used in the management of canine and feline gastric emptying, intestinal transit, and colonic motility disorders throughout most of the 1990s.10,13,14 Cisapride was withdrawn from the USA, Canada and certain Western European countries in July of 2000 following reports of untoward cardiac side effects in human patients. Similar cardiac effects have been characterized in experimental dogs, but in vivo effects have not yet been reported in dogs or cats. The withdrawal of cisapride has created a clear need for new GI prokinetic agents, although cisapride continues to be available in several western European countries and from compounding pharmacies throughout the United States.
Prucalopride, a new prokinetic agent currently undergoing drug-development and testing may prove useful in the therapy of GI motility disorders of several animal species.
Misoprostol is a prostaglandin E1 analogue that reduces the incidence of NSAID-induced gastric injury. The main side effects of misoprostol therapy are abdominal discomfort, cramping, and diarrhea. Studies in dogs suggest that prostaglandins may initiate a giant migrating complex pattern and increase colonic propulsive activity. In vitro studies of misoprostol show that it stimulates feline and canine colonic smooth muscle contraction. Given its limited toxicity, misoprostol may be useful in cats (and dogs) with severe refractory constipation.
Ranitidine and nizatidine, classic histamine H2 receptor antagonists, may also stimulate canine and feline colonic motility. These drugs stimulate contraction apparently through the inhibition of tissue acetylcholinesterase and accumulation of acetylcholine at the motor endplate. It is not yet clear how effective these drugs are in vivo, although both drugs stimulate feline colonic smooth muscle contraction in vitro. Cimetidine and famotidine, members of the same class of drug, are without this effect.
Surgery
Colectomy should be considered in cats that are refractory to medical therapy. Cats have a generally favorable prognosis for recovery following colectomy, although mild to moderate diarrhea may persist for weeks to months postoperatively in some cases.15,16 Pelvic osteotomy without colectomy has been recommended for cats with pelvic fracture malunion and hypertrophic megacolon of less than 6 months duration.17 Pathological hypertrophy may be reversible with early pelvic osteotomy in such cases. Some surgeons still prefer colectomy in this instance because of the technical difficulty of some pelvic osteotomies.18
Prognosis
Many cats have one or two episodes of constipation without further recurrence, although others may progress to complete colonic failure. Cats with mild to moderate constipation generally respond to conservative medical management (e.g., dietary modification, emollient or hyperosmotic laxatives, and colonic prokinetic agents). Early use of colonic prokinetic agents (in addition to one or more laxative agents) is likely to prevent the progression of constipation to obstipation and dilated megacolon in these cats. Some cats may become refractory to these therapies, however, as they progress through moderate or recurrent constipation to obstipation and dilated megacolon; these cats eventually require colectomy. Cats have a generally favorable prognosis for recovery following colectomy, although mild to moderate diarrhea may persist for 4 to 6 weeks post-operatively in some cases.
Key Facts
■ Megacolon is a disorder found most often in male, middle-aged cats, although it may affect cats of any age, gender, or breed.
■ Medical therapy consists of colonic reduction of impacted fecal material, laxative therapy, prokinetic therapy, and surgery.
■ Cats may have transient diarrhea following sub-total colectomy, but most recover normal intestinal function following such surgery.