Gastritis
Classification
By definition, gastritis is an inflammatory disease of the stomach. Many patients with clinical signs of vomiting or upper GI problems are thought to have some type of mucosal injury; however, as infiltration of the gastric mucosa with inflammatory cells is either not diagnosed or minimal, it might be therefore more accurate to use the term gastropathy for these cases.
The Sydney classification system is the most commonly used scheme for the classification of gastritis in human medicine.1 Unfortunately, a similar system is, as yet, not available in veterinary medicine. Gastritis is commonly grouped into acute or chronic, based on the duration of the clinical signs and not on histological parameters. If inflammation is deep, a peptic ulcer may ensue.
4.4.1.1 Acute gastritis
Although many conditions have been found to cause acute gastritis, the most common ones are dietary hypersensitivity and dietary indiscretion.2 Acute gastritis does not have any age predilection and can occur in any dog or cat. It is most often a result of ingestion of inappropriate food (i.e., spoiled or toxic food stuff) or foreign material (e.g., rocks, bones, wood, or weeds). Other possible causes are drugs (e.g., NSAIDs, corticosteroids), chemicals (e.g., fertilizer, herbicide), or heavy metals (e.g., lead, zinc). Several infectious causes also can cause gastritis, such as viral (e.g., parvovirosis, distemper, infectious hepatitis) or parasitic organisms (e.g., Physaloptera spp., Ollula- nus spp.). In human medicine, the discovery of bacterial gastritis due to Helicobacter pylori infection has revolutionized the field of gastroenterology.3 In contrast, in veterinary medicine it is still not clear if Helicobacter spp. is indeed pathogenic, or merely a commensal organism, rarely resulting in vomiting in some patients.4 Most often, only a tentative diagnosis can be reached based on signalment, history, clinical signs, and physical examination findings.
During endoscopy, superficial hemorrhage due to erosions and edema can be seen.Treatment of acute gastritis
Initially, dietary restriction by withholding food for 1224 hours is all that is needed. Depending on the severity of the clinical signs (i.e., dehydration, continuous vomiting), the animal will also need to be treated with intravenous crystalloids (e.g., lactated Ringer’s solution) but no water is given orally. Because most affected animals are hypokalemic, potassium often needs to be supplemented based on the actual serum potassium concentration (see Table 5.3).Water can be introduced 24 hours after vomiting has ceased. If the animal tolerates oral water, a bland commercial or home-cooked diet (e.g., white fish or chicken and rice, cottage cheese), given in small amounts multiple times during the day, is indicated. The animal’s regular food can be slowly reintroduced over a 3- to 5-day period after vomiting has ceased.
In some patients, symptomatic treatment with antiemetics is necessary to stop the vomiting. Because antiemetic therapy is based on the neurotransmitter-receptor interactions, it is important to understand these mechanisms (Figure 4.5). Several neurotransmitters and receptors have been identified in the chemoreceptor trigger zone (CRTZ), including receptors that bind dopamine (D2-dopaminergic), neurokinin1 (NK1), norepinephrine (α2-adrenergic), 5-hydroxytryptamine (5-HT3- serotonergic), acetylcholine (M1-cholinergic), histamine (H1. and H2-histaminergic), or enkephalins (ENKμ-enkephaliner- gic). In contrast, the only receptors shown to be present in the vomoting center so far are NK1, 5-hydroxytryptamine3 and α2-adrenergic receptors. The α2-adrenergic receptors in the
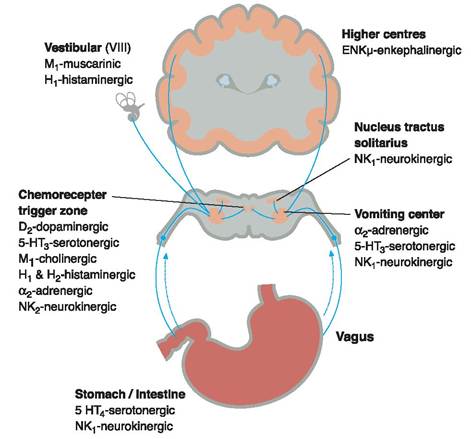
Figure 4.5:
Schematic drawing of the emetic pathways and their receptors.
The vomiting center lies in the medulla oblongata and receives input from various stimuli. From the periphery (e.g., the stomach or intestine), the vomiting center is stimulated via sympathetic and parasympathetic nerves. Additional stimulation comes from the chemoreceptor trigger zone, which is located outside the blood-brain barrier. Finally, stimuli might also come from the vestibular apparatus, higher centers, or the nucleus tractus solitarius.emetic center and in the CRTZ may be antagonized by α2 antagonists (e.g., yohimbine, atipamezole) or by mixed α1∕α2 antagonists (e.g., prochlorperazine, chlorpromazine). In the vestibular apparatus, muscarinic M1 receptors and acetylcholine have been demonstrated to be present, and therefore mixed M1∕M2 antagonists (e.g., atropine, scopolamine) and pure M1 antagonists, such as pirenzepine, may inhibit motion sickness in dogs and cats. Many receptors are found in the gastrointestinal tract, but the NK1, 5-HT3 receptors are likely to play the most important role in the initiation of vomiting. Cytotoxic agents cause the release of 5-HT from enterochromaffin cells in the gastrointestinal tract, which then activate the 5-HT3 receptors on afferent vagal fibers. Thus, vomiting induced by the activation of 5-HT3 receptors can be completely abolished by treating the patient with a 5-HT3 antagonist, such as dolasetron, ondansetron, granisetron, or tropiset- ron. Another antagonist of 5-HT3 receptors is metoclopramide, but only at high concentrations. Recently, the administration of substance P has been found to result in emesis by binding to the NK1 receptor. NK1-receptor antagonists block central and peripheral vomiting both in dogs and ferrets.5
Several antiemetic drugs are directed at the neurotransmitterreceptor system just described (Table 4.1).
These antagonistsare classified as α2-adrenergic, D2-dopaminergic, NK1, H1-his- taminergic, H2-histaminergic, M1-muscarinic-cholinergic, 5-HT3-serotonergic, and 5-HT4-serotonergic. Some of these drugs have several mechanisms of action as an antiemetic agent. For example, the phenothiazines (e.g., prochlorperazine, chlorpromazine) are antagonists of α1- and α2-adrenergic, D2-dopaminergic, H1- and H2-histaminergic, and muscarinic- cholinergic receptors. Phenothiazines are very potent but should be avoided in dehydrated or hypotensive animals without first resuscitating the patient with intravenous fluid administration. Also, these drugs are contraindicated in animals with a known seizure history. Metoclopramide blocks receptors in the CRTZ, increases the threshold in the emetic center, and also has an effect on the viscera. Metoclopramide increases the lower esophageal sphincter tone, decreases the pyloric sphincter tone, and increases the frequency and amplitude of gastric and duodenal contractions. All these functions combined make metoclopramide useful for controlling vomition that is due to nonspecific gastritis or gastric motility disorders. The prokinetic activity of metoclopramide seems to be limited to the liquid phase of gastric emptying as a study showed no effect on the gastric emptying rate of digestible solids.6 Metoclopramide can be given orally, intravenously, or as a constant rate infusion.
Table 4.1: Antiemetic medications. This table shows a comprehensive summary of antiemetic medications with their commonly recommended dosages.
| Classification | Example | Site of action | Dosage | Side effects |
| α2-adrenergic | ■ atipamezole | ■ CRTZ, emetic center | ■ Unknown | ■ hypotension, sedation |
| antagonists | ■ chlorpromazine | ■ CRTZ, emetic center | ■ 0.2-0.4 mg/kg SC, IM q 8 h | ■ hypotension, sedation |
| ■ prochlorperazine | ■ CRTZ, emetic center | ■ 0.1-0.5 mg/kg SC, IM q 6-8 h | ■ hypotension, sedation | |
| ■ yohimbine | ■ CRTZ, emetic center | ■ 0.25-0.5 mg/kg SC, IM q 12h | ■ hypotension, sedation | |
| D2-dopaminergic | ■ chlorpromazine | ■ CRTZ | ■ 0.2-0.4 mg/kg SC, IM q 8 h | ■ tremors, shivering |
| antagonists | ■ domperidone | ■ GI smooth muscle | ■ 0.1-0.3 mg/kg IM, IV q 12 h | ■ none reported |
| ■ metoclopramide | ■ CRTZ, GI muscles | ■ 0.2-0.4 mg/kg PO, SC, IM q 6 h | ■ extrapyramidal signs | |
| ■ prochlorperazine | ■ CRTZ | ■ 0.1-0.5 mg/kg SC, IM q 6-8 h | ■ sedation, hypotension | |
| ■ trimethobenzamide | ■ CRTZ | ■ 3 mg/kg IM q 8-12 h | ■ allergic reaction | |
| NK1-receptor | ■ maropitant | ■ CRTZ, emetic center | ■ 2 mg/kg PO q 24 h | ■ none reported |
| antagonist | ■ 1 mg/kg SC q 24 h | |||
| H1-histaminergic | ■ chlorpromazine | ■ CRTZ | ■ 0.2-0.4 mg/kg SC, IM q 8 h | ■ tremors, shivering |
| antagonists | ■ dimenhydrinate | ■ CRTZ | ■ 4-8 mg/kg PO q 8 h | ■ sedation |
| ■ diphenhydramine | ■ CRTZ | ■ 2-4 mg/kg PO, IM q 8 h | ■ sedation | |
| ■ prochlorperazine | ■ CRTZ | ■ 0.1-0.5 mg/kg SC, IM q 6-8 h | ■ sedation, hypotension | |
| M1-cholinergic | ■ chlorpromazine | ■ CRTZ | ■ 0.2-0.4 mg/kg SC, IM q 8 h | ■ hypotension, sedation |
| antagonists | ■ pirenzepine | ■ vestibular, CRTZ | ■ unknown | ■ unknown |
| ■ prochlorperazine | ■ CRTZ | ■ 0.1-0.5 mg/kg SC, IM q 6-8 h | ■ hypotension, sedation | |
| ■ scopolamine | ■ vestibular, CRTZ | ■ 0.03 mg/kg SC, IM q 6 h | ■ sedation, xerostomia | |
| 5-HT3-serotonergic | ■ dolasetron | ■ CRTZ | ■ 0.3-0.6 mg/kg IV, SC, PO q 8-12 h | ■ unknown |
| antagonists | ■ granisetron | ■ CRTZ, vagal afferents | ■ unknown | ■ sedation, head shaking |
| ■ metoclopramide | ■ CRTZ, GI muscles | ■ 0.2-0.4 mg/kg PO, SC, IM q 6 h | ■ extrapyramidal signs | |
| ■ ondansetron | ■ CRTZ, vagal afferents | ■ 0.5-1 mg/kg PO q 12-24 h | ■ sedation, head shaking | |
| 5-HT4-serotonergic | ■ cisapride | ■ myenteric neurons | ■ 0.1-0.5 PO q 8 h | ■ none reported |
| antagonists |
IM = muscular administration; IV = intravenous administration; PO = oral administration; SC = subcutaneous administration
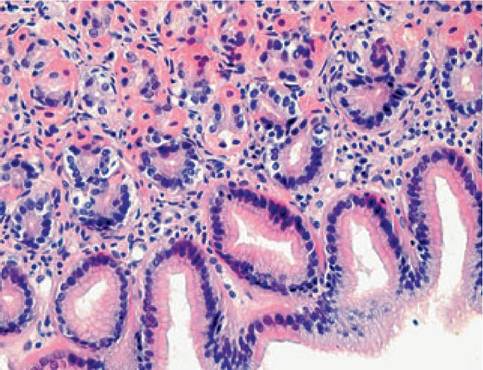
Figure 4.6:
Lymphoplasmacytic gastritis.
This figure shows a histopathological image of the gastric mucosa of a 5-year-old female mixed-breed dog with lymphoplasmacytic gastritis. There are large aggregates of lymphocytes and a smaller number of plasma cells infiltrating the gastric mucosa in this patient. (HE staining, 120x; image courtesy of Dr. Thomas Bilzer, University of Dusseldorf, Germany.)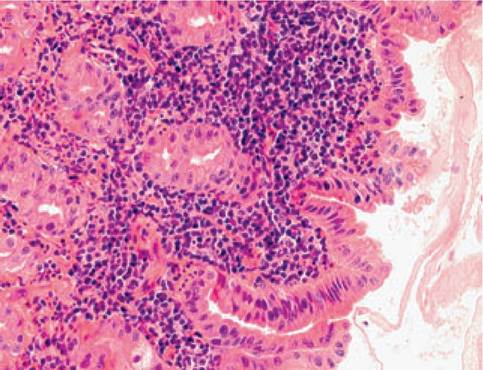
Figure 4.7:
Eosinophilic gastritis. This figure shows a histopathological image of the gastric mucosa of a 13-year-old male cat with inappetence and weight loss. Note the abundant presence of eosinophils throughout this section of gastric mucosa. Histological diagnosis: eosinophilic gastritis. (HE staining, 120x; image courtesy of Dr. Thomas Bilzer, University of Dusseldorf, Germany.)
A new NK1-receptor antagonist, maropitant, will soon become available and licensed for dogs. In various licensing studies, maropitant has been highly effective in abolishing vomiting induced through peripheral emetogenic stimuli, such as cisplatin administration or central emetogenic stimuli, such as apomorphine.7 Even travel-sickness-induced vomiting was successfully suppressed by the administration of maropitant.
4.3.3.1 Chronic gastritis
The pathogenesis of chronic gastritis in dogs and cats is not fully understood. In some cases, a cause, such as parasitism or a metabolic disorder (e.g., uremia, hepatopathy), can be identified. Several dog breeds are at risk for chronic gastritis, including the Basenji, the Drentse Patrijshond, and the Norwegian Lundehund.8 In most cases, however, chronic gastritis is idiopathic and an immune-mediated condition is hypothesized to be responsible for the inflammatory infiltrate in the gastric mucosa. Experimentally, chronic gastritis in dogs can be induced by mucosal irritants, systemic administration of gastric juice, or prenatal thymectomy;9 however, each of these experimental models disturbs oral tolerance.
Chronic idiopathic gastritis is probably part of the inflammatory bowel disease (IBD) syndrome and may arise as an adverse reaction to food or bacterial antigens. The presence of Helicobacter spp. in the stomach of dogs almost certainly does not cause chronic gastritis.4 In cats the clinical role of gastric Helicobacter spp. is less clear.10Clinical signs in dogs and cats with chronic gastritis are characterized by chronic persistent or intermittent vomiting of variable frequency and character. Because inflammation impairs gastric motility and delays gastric emptying, animals with chronic gastritis may retain food in the stomach for long periods of time. A definitive diagnosis of chronic gastritis requires a mucosal biopsy. The gastritis can then be classified based on the histopathological findings as lymphoplasmacytic gastritis, eosinophilic gastritis, hypertrophic gastritis, or atrophic gastritis.
4.3.3.1.1 Lymphoplasmacytic gastritis
Most patients with chronic gastritis have some infiltration of the gastric mucosa with lymphocytes and/or plasma cells (Figure 4.6). This form of gastritis is often part of the more diffuse IBD complex and has likely a similar etiopathogenesis. Abnormal or increased food antigens, intestinal bacterial antigens, or both together and /or an abnormal or overwhelmed tolerance of the host might play an integral part. There are no typical clinical, laboratory, or diagnostic imaging findings in dogs and cats with gastritis. Since no uniform criteria to evaluate gastric biopsies exist so far, there must be good communication between the clinician and pathologist to ensure that neither over- nor under-interpretation of the biopsy specimen occurs. Severe lymphoplasmacytic infiltration is often difficult to distinguish from gastric lymphoma, especially when the biopsy specimens are small.
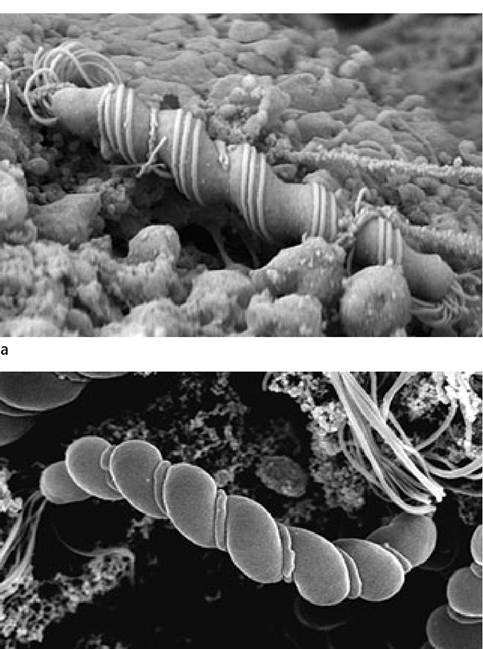
b
Figure 4.8:
Electron microscopic views of Helicobacter spp. a: This picture shows a scanning electron microscopic view of Helicobacter felis from an experimentally infected mouse. Please note the typical three periplasmic filaments and the spiral shape. H. felis measures 4-6 μm in length and approximately 0.5 μm in thickness. (Image courtesy of Dr. M. Stoffel, Bern, Switzerland). b: Scanning electron microscopic image of H. bizzozeroniifrom an experimentally infected mouse. While the most common type of H. bizzozeroniilack the periplasmic fibers, some show a filament running along the groove of the spirals. (Image courtesy of Dr. M. Stoffel, Bern, Switzerland.)
4.4.1.2.2 Eosinophilic gastritis
Eosinophilic gastritis is an uncommon disorder of unknown etiology that is characterized by diffuse eosinophilic infiltration of the distal portion of the stomach (Figure 4.7) and is also often associated with eosinophilic infiltration of the small bowel or colon. Gastric infiltration is usually restricted to the mucosa but in some patients may extend into the muscularis and even the serosa. Mucosal involvement causes enlargement of the rugal folds. The diseased mucosa may become ulcerated, which leads to bleeding or leakage of plasma proteins into the gastric lumen. Peripheral eosinophilia is a common finding, but its severity can vary markedly. Some pets also have a history of either urticaria or vomiting that may be associated with the ingestion of a specific diet.
4.4.1.2.3 Hypertrophic gastritis
Chronic hypertrophic gastritis is a rare disorder that appears either as diffuse, generalized mucosal hypertrophy or, more frequently, as a localized hypertrophy of the antral mucosa that may cause intermittent or chronic pyloric obstruction. Causative factors that may lead to gastric mucosal hypertrophy include chronic inflammation, foreign bodies, or long-term use of proton pump inhibitors. Hypergastrinemia can also have a trophic effect on the mucosa, as seen in chronic renal disease, chronic gastric distension, gastrin-secreting tumors (gastrinoma), and idiopathic hypertrophy of antral G cells. Boxers and Basenjis have a predilection for the diffuse form of hypertrophic gastritis. In contrast, the localized form has a predilection for miniature and toy dog breeds (e.g., Lhasa Apso, Maltese, Pekingese, and Shih Tzu). The hypertrophic mucosa is inflamed and causes delayed emptying, chronic vomiting, anorexia, and lethargy.
4.4.1.2.4 Atrophic gastritis
Atrophic gastritis is a rare disorder in which the gastric mucosa atrophies and loses its secretory functions. Atrophic gastritis has been reported in the Norwegian Lundehund. The cause is unknown, but the condition occurs mainly in older dogs and may be mediated through the immune system. Atrophic gastritis may also be a sequel to chronic reflux gastritis in dogs. The predominant complaint is chronic intermittent vomiting. Mucosal degeneration is thought to result in achlorhydria, which may predispose to bacterial overgrowth in the proximal small intestine. This can lead to malabsorption, chronic diarrhea, and /or loss of body weight and condition.
4.4.1.2.5 Helicobacter infection
Helicobacter spp. are gram-negative, microaerophilic, curved to spiral-shaped, motile bacteria. Their main location is the stomach, however, they can also be found in the intestine and the liver.11-13 To date, over 30 organisms with typical characteristics of Helicobacter spp. have been described, with new species being published constantly. Most gastric Helicobacter-like organisms (GHLO) found in dogs and cats are large spiral organisms (0.5 ? 5-10 μm) that cannot be distinguished by light microscopy. To date H. felis, H. bizzozeronii, H. salomonis, Flex- ispira rappini, H. bilis, and “H. heilmannii” have all been reported to have been present in the stomach of dogs,14-16 while H. felis, H. pametensis, H. pylori, H. bizzozeronii, H. salomonis, and “H. heilmannii” have been reported to be present in the stomach of cats (Figures 4.8 a and b). 13,15,17,18 Mixed infections with two or more Helicobacter spp. appear to be common in dogs and cats.15,16
Several studies showed a high prevalence of GHLO in cats and dogs (Table 4.2) with up to 100% infection rate amongst laboratory animals, 50-100% amongst healthy pets, and 41-100% among vomiting pets. Housing conditions and age appear to play an important role with pets living in shelters or colonies having a higher prevalence, while young animals may be less often colonized than adults, but this is controversial.14,17
The mode of transmission of Helicobacter spp. is still unclear. Fecal-oral transmission is hypothesized by some, since H. pylori can be cultured from cat feces. Oral-oral transmission is hypothesized by others, because H. pylori can be found in the saliva of infected humans. Also, the spouses of infected individuals also were shown to have a higher prevalence.
In human patients, there is extensive evidence implicating H. pylori in the pathogenesis of chronic superficial gastritis. Eradication of H. pylori by use of antimicrobial therapy may cure gastritis and the titer of anti-H. pylori antibodies decreases with time. A plethora of reports have shown many putative mechanisms by which H.pylori alters gastric physiology;19 e.g., through the induction of gastric inflammation (by secretion of IL-8, platelet activating factor, urease, etc.), through the disruption of the gastric mucosal barrier (by disrupting phospholipases, secreting vacuolating cytotoxins, inducing apoptosis, etc.), or through altering the gastric-secretory axis (by decreasing somatostatin release, inducing hypergastrinemia, diminishing the responsiveness of parietal cells, etc.). Infection with Helicobacter spp. also predisposes humans to the development of gastric cancer.
In pets with naturally acquired Helicobacter colonization, however, the pathogenic role of this organism is still highly debated. Obvious clinical signs of infection are absent in the majority of infected cats and dogs, and few studies have investigated the cellular and immunological consequences of infection. In dogs, a mild gastritis with infiltration of the gastric mucosa involving lymphocytes and plasma cells was most commonly found,4,14 but no correlation between the histopathological changes and the occurrence of GHLOs as well as a clear pathologic role due to enlarged canaliculi and py- knotic parietal cells has been reported. In some cats, normal gastric mucosa was found in several GHLO-colonized animals, while others reported mild chronic gastritis irrespective of GHLO colonization.17,20,21 In dogs with naturally acquired Helicobacter spp. infection, a variety of secretory function tests, such as unstimulated gastric pH, fasting, post-prandial and bombesin-stimulated plasma gastrin concentrations as well as
Table 4.2: Prevalence of gastric Helicobacter-like organisms in cats and dogs
| Status | % infected | # of pets | Species | Reference |
| Healthy | 100 | 12 | cat | Weber et al. Am J Vet Res 1958; 19: 677-680 |
| 100 | 130 | dog | Henry et al. Am J Vet Res 1987; 48: 831-836 | |
| 41 | 29 | cat | Geyer et al. Vet Rec 1993; 133: 18-19 | |
| 86 | 155 | cat | Otto et al. J Clin Microbiol 1994; 32: 1043-1049 | |
| 91 | 154 | dog | Eaton et al. J Clin Microbiol 1996; 34: 3165-3170 | |
| 100 | 125 | cat | El-Zataari et al. J Med Microbiol 1997; 46: 372-376 | |
| 100 | 15 | cat | Papasouliotis et al. Vet Rec 1997; 140: 369-370 | |
| 190 | 10 | cat | Yamasaki et al. JAm Vet MedAssoc 1998; 21 2: 529-533 | |
| 186 | 121 | dog | Yamasaki et al. JAm Vet MedAssoc 1998; 21 2: 529-533 | |
| 194 | 132 | cat | De Majo et al. Europ J Comp Gastroenterol 1998; 3: 13-18 | |
| 191 | 158 | cat | Neiger et al. J Clin Microbiol 1998; 36: 634-637 | |
| 100 | 125 | dog | Happonen et al. J Vet MedAssoc 1998; 43: 305-315 | |
| 100 | 15 | cat | Norris et al. J Clin Microbiol 1999; 37: 189-194 | |
| 93 | 168 | dog | Neiger et al. Microbiol Ecol Health Dis 1999; 11; 234-240 | |
| Diseased | 57 | 160 | cat | bgcolor=white>Geyer et al. Vet Rec 1993; 133: 18-19|
| 74 | 142 | dog | Geyer et al. Vet Rec 1993; 133: 18-19 | |
| 176 | 127 | cat | Hermanns et al. J Com Pathol 1995; 1 12: 307-318 | |
| 82 | 122 | dog | Hermanns et al. J Com Pathol 1995; 1 12: 307-318 | |
| 100 | 124 | cat | Papasouliotis et al. Vet Rec 1997; 140: 396-370 | |
| 164 | 133 | cat | Yamasaki et al. JAm Vet MedAssoc 1998; 21 2: 529-533 | |
| 161 | 156 | dog | Yamasaki et al. JAm Vet MedAssoc 1998; 21 2: 529-533 | |
| 195 | 121 | dog | Happonen et al. J Vet MedA 1998; 43: 305-315 |
pentagastrin-stimulated maximal acid output and titratable acidity, were similar when compared to a SPF, Helicobacter-free control group.22
There are only a few studies on experimental infection of dogs and cats with Helicobacter spp. While experimentally infected gnotobiotic dogs showed chronic gastritis and an increase in fasting gastric pH in some, there was no relationship between H.felis infection and gastric inflammation in SPF dogs after six months in others.23 The gastric secretory axis, assessed by fasting and meal-stimulated plasma gastrin concentration, mucosal gastrin and somatostatin immunoreactivity, fasting gastric pH and pentagastrin-stimulated gastric acid secretion functioned similarly in both the infected and uninfected SPF dogs.23 Conventional puppies infected with H. pylori showed some clinical signs shortly after inoculation and the gastric mucosa initially demonstrated acute gastritis changing to chronic gastritis with time. In another investigation, SPF, Helicobacter-free cats were studied before and for one year after inoculation with H.felis.24 Uninfected cats were used as controls. Lymphoid follicular hyperplasia, atrophy, and fibrosis were observed primarily in the pylorus of the infected cats.
Seroconversion of experimentally infected dogs and cats was observed in all of these studies. H.felis- and H. pylori-infected gnotobiotic dogs showed a fairly rapid and uniform seroconversion 3 weeks after infection, while H. felis-infected SPF dogs showed a more gradual and variable seroconversion over a six-month period after infection.23

Figure 4.9:
Rapid urease test. This figure shows examples of a positive (red) and negative (yellow) rapid urease test that is used for the diagnosis of Helicobacter spp. Rapid urease tests are based on a color change, which is caused by a change in pH that is due to the production of ammonium by urease-producing organisms in a biopsy sample.
Diagnostic tests for GHLO are either invasive (i.e., rapid urease tests, histopathology, touch cytology, culture, polymerase chain reaction of biopsies, or electron microscopy) requiring a biopsy sample or they can also be non-invasive (i.e., urea breath and blood tests, serology, and fecal PCR testing).
Invasive tests for Helicobacter spp.
The rapid urease test (also called CLO test for Campylobacter- like organism test) is based on the production of urease by all gastric Helicobacter spp. A tissue sample is incubated in a broth containing urea and phenol red as a pH indicator. As the urease breaks down urea into ammonia, the pH rises and a color change occurs (Figure 4.9). The results can often be obtained within one to three hours, but may take up to 24 hours.
Histopathology relies on the visualization of Helicobacter organisms in gastric biopsy samples. Special staining such as Warthin-Starry silver, Giemsa, or toluidine blue stain will enhance the visibility of GHLOs (Figure 4.10). Due to the patchy distribution of the Helicobacter organisms, several biopsies from the antrum and corpus should be evaluated. Touch cytology stained with Gram’s or Diff Quick stain is a simple, rapid, and sensitive diagnostic test; however, the extent of a concurrent gastritis cannot be evaluated based on cytological evaluation alone (Figure 4.11).
Culture for GHLOs is cumbersome and the least sensitive method for diagnosing these organisms; however, a positive culture is highly specific. Gastric Helicobacter spp. are difficult to isolate in vitro. Polymerase chain reaction (PCR) of DNA extracted from a biopsy specimen permits definitive identification of the Helicobacter strain present. Electron microscopy can be used to differentiate Helicobacter spp. on the basis of typical morphological criteria. Five cultured canine Helicobacter spp. could be differentiated based on transmission and scanning electron microscopy (Figures 4.8a and 4.8b).25 Overall, the rapid urease test, histopathology with special stains, and touch cytology are associated with a high accuracy for diagnosing a Helicobacter spp. colonization in dogs and cats (Table 4.3).
Non-invasive tests
The urea breath and blood tests use labeled urea (mostly labeled with non-radioactive 13C). Ingested urea is metabolized in the stomach by bacterial urease to ammonia and the released carbon atoms are absorbed into the systemic circulation
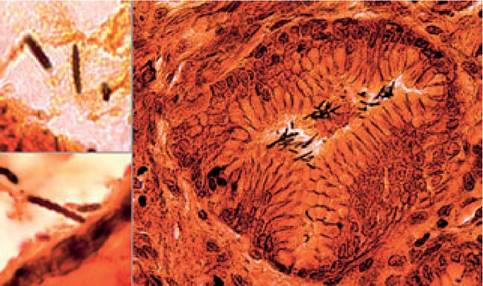
Figure 4.10:
Helicobacter spp. in a Warthin-Starry silver stain of a gastric biopsy. This picture shows a gastric biopsy stained with Warthin-Starry silver stain. This biopsy was taken from a naturally infected cat. Multiple large spiral-shaped organisms can be seen in a gastric pit. The spiral morphology is clearly visible under higher magnification.
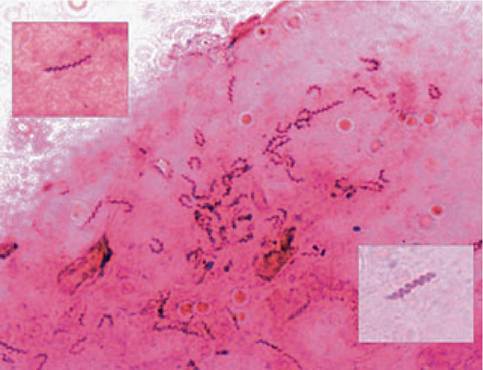
Figure 4.11:
This figure shows multiple Helicobacter spp. organisms in a Gram-stained gastric touch cytology. The proteinaceous background is due to gastric mucous. The enlargements clearly delineate the spiral structure of these bacteria.
and finally exhaled. The exhaled air is collected and the ratio of 12CO2 to 13CO2 is measured.17-26 Since the urea breath test demonstrates the actual colonization with Helicobacter spp. organisms, it is the preferred non-invasive method to document a successful eradication in both humans and animals.
Serology by ELISA or Western blotting is used extensively in human epidemiological studies and IgG or IgA can be quantified in both serum and gastric fluid. Dogs and cats harbor several Helicobacter spp. but not H. pylori, and thus serum samples of pets cannot be analyzed by commercially available serological tests. Amplification of Helicobacter DNA from canine fecal samples has recently been described.12 With this technique, gastric as well as intestinal Helicobacter DNA could be identified in dogs. Also, the treatment success could be monitored non-invasively by this method.
4.3.3.1.2 Parasitic gastritis
Physaloptera spp. are nematodes with an indirect live cycle requiring an intermediate host to develop into the infective stage. Suitable intermediate hosts (e.g., cockroaches, field crickets, canal crickets, or flour beetles) ingest the eggs, which have been shed by the definite hosts (e.g., cats, dogs). The first- stage larvae hatch in the intestine of intermediate hosts, migrate to the outer layer of the intestine, encyst and molt to second-, and finally, infective third-stage larvae. After the intermediate hosts are ingested by either paratenic (e.g. frogs, snakes, or mice) or definite hosts, the adults develop and attach to the gastric or duodenal mucosa.27
Table 4.3: Accuracy of various tests for the diagnosis of gastric Helicobacter spp. in dogs and cats
| Test | Sensitivity | Specificity |
| Based on morphology | ||
| Gram's stain | 95% | 92% |
| Warthin-Starry stain | 90% | 100% |
| Based on urease activity | ||
| Rapid urease tests | 93% | 92% |
| Urea breath test | 90% | 73% |
| Based on molecular genetics | ||
| PCR of gastric biopsy | 94% | 92% |

Figure 4.12:
Physaloptera. This figure shows an endoscopic picture of the stomach of a dog with a single Physaloptera specimen. (Image courtesy of Dr. Mike Willard, Texas, USA.)
It is unclear if Physaloptera are always pathogenic and how many stomach worms are required for clinical signs to ensue. Besides histological evidence of gastritis, these parasites can also result in delayed gastric emptying, possibly due to altered electromechanical activity.28 Other clinical signs are chronic or intermittent vomiting, diarrhea, regurgitation, weight loss, melena, and lethargy.27 Diagnosis can be difficult as fecal flotation is frequently falsely negative. Speculated reasons for this include that the adults only produce low numbers of eggs, the fact that a single-sex infection produces no eggs at all, or the fact that the specific gravity of the fecal flotation medium is too close to that of the eggs and thus the eggs do not float well.28 Identification of worms in the vomit or endoscopic visualization of stomach worms (1-6 cm in length, stout, cream-colored to white, straight or coiled; Figure 4.12) appears to be most successful in the diagnosis of this parasite.
Ollulanus tricuspis is a common gastric nematode of cats with a prevalence of up to 20% that also occurs rarely in dogs.29 After oral ingestion of third-stage larvae, the complete life cycle occurs within the stomach of the host, where the parasite attaches to the gastric mucosa. Infective larvae are vomited up and survive in the environment for up to 15 days, where they can infect another animal. Common clinical signs are inappetence, intermittent vomiting, and weight loss. Gastric erosions, increased mucous production, mucosal hyperplasia, and infiltration with inflammatory cells can be seen histopatho- logically. Diagnosis is best achieved by examining vomited material (possibly induced by the administration of xylazine or metedomidine) or gastric lavage solution. Rarely, parasites can be found in gastric biopsy samples by histopathology. Fecal flotation is rarely diagnostic.
4.3.3.1.3 Treatment of chronic gastritis
If possible, the underlying cause of the gastric inflammation should be managed first (e.g., removal of foreign body, cessation of drug administration). Diagnosis of infestation with a stomach worm (i.e., Physaloptera spp. in dogs and Ollulanus tricuspis in cats) maybe challenging and routine therapy with a broad-spectrum anthelminthic agent that is effective in eradicating stomach worms (i.e., in dogs: pyrantel pamoate at 15 mg/kg PO repeated in 2-3 weeks; in cats: fenbendazole at 50 mg/kg PO q 24 h for 3 days) is prudent before recommending more expensive diagnostic tests.27 However, most cases of chronic gastritis are idiopathic and treatment of the underlying cause is thus rarely possible. In cases of idiopathic chronic gastritis, rational treatment options include dietary management, immunosuppressive therapy, inhibition or neutralization of gastric acid secretion (see 4.4.1.3; Table 4.1; 4.4.1.1).
Dietary management is based on the concept that antigens in the food may be responsible for an exaggerated immune response of the body. Feeding single novel protein and carbohydrate sources, to which the animal has not yet been exposed to, is the cornerstone of this treatment concept. Although commercial “hypoallergenic” diets are very useful, on rare occasions it is necessary to feed a home-cooked novel protein source (e.g., kangaroo or horse). In most cases, some response should be seen after a 2-week strict dietary trial.
Immunosuppressive drug therapy is indicated in those dogs and cats that do not respond to dietary management alone (e.g., those with lymphoplasmacytic or eosinophilic gastritis). Corticosteroids, in addition to their immunosuppressive and anti-inflammatory properties, have regenerative effects on the gastric parietal cells. The ulcerogenic property of corticosteroids is of concern only in dogs that are exposed to a marked synergistic ulcerogenic effect (e.g., NSAID administration or hypotension). Initially, prednisone is given at a dose of 1-2 mg/kg PO q 12 h for 5 to 7 days. This dose is then gradually tapered in decremental doses of 50% over a period of several months. Other immunosuppressive drugs, such as azathioprine and cyclophosphamide, have only been used sporadically in dogs with chronic gastritis and should not be used for this purpose in cats.
4.4.1.3 Gastric ulceration
By definition, an ulcer is an area of damaged gastric mucosa to the level of the lamina muscularis mucosae or deeper; more superficial damage is called erosion. Erosions or ulcers occur when the »aggressive forces« (i.e., acid, pepsin, and /or trauma) are more potent than the Oprotective forces« (i.e., mucosal microcirculation, epithelial turnover, gastric mucus, and prostaglandins). Epithelial cells have a rapid turnover and need an
abundant blood circulation to ensure the transport of nutrients and oxygen and the removal of back-diffused hydrogen ions. The entire gastric surface is replaced every 2 to 3 days. Epithelial cells are produced in the crypts and then migrate towards the gastric lumen, where they are shed. Gastric mucus neck cells produce a viscous gel of glycoprotein (5%) and water (95%), which adheres to the surface of the mucosa. This mucus protects against mechanical abrasion and acts as a barrier against digestive enzymes. In addition, bicarbonate is secreted actively into this layer. A pH gradient forms from the lumen to the epithelium, which neutralizes gastric acid. Finally, prostaglandins, which are derived from arachidonic acid via the enzyme cyclooxygenase (COX), have a protective role for the gut mucosa. They increase gastric mucus and bicarbonate secretion, maintain mucosal blood flow by causing vasodilation, and inhibit acid secretion. They may possibly stimulate mucosal cell turnover and migration by acting as an intercellular messenger. Prostaglandin-inhibiting drugs, such as NSAIDs, can counteract all these protective mechanisms and lead to the formation of gastric ulcers.
Peptic ulcers of the gastric and duodenal mucosa are not commonly seen in dogs or cats, but several underlying mechanisms can lead to the formation of this type of ulcer (Table 4.4). NSAIDs (e.g., aspirin, flunixin, ibuprofen, indomethacin, ketoprofen, meloxicam, naproxen, phenylbutazone, or piroxicam) inhibit the COX-1 enzyme, thereby limiting prostaglandin production. Even though these drugs have been implicated as a common cause of peptic ulcers in dogs, only a few reports of NSAID-induced peptic ulcers in pets exist.30,31 Eicosanoids produced by COX-2 are mainly responsible for the inflammatory and pain properties of the gastric mucosa, while those produced by COX-1 are mainly responsible for its protective mechanisms. Unspecific COX inhibition increases the ulcerogenic risk dramatically. However, newer NSAIDs are COX-2 specific (e.g., carprofen) and have a lower, although not abolished, ulcerogenic effect.32
Corticosteroids also decrease the production of protective eicosanoids. Nevertheless, they are only responsible for peptic ulcers in dogs with concurrent problems, such as severe hypotension or if they are also given NSAIDs.33 Mast cell tumors have long been thought to be responsible for peptic ulcers because of their histamine-containing granules, which can cause hyperacidity in the stomach.34 However, no series of dogs or cats with mast cell tumor and peptic ulceration or even gastritis has been published as of yet. Most dogs with acute intervertebral disk diseases have endoscopic signs of gastric erosions, and surgical interventions with or without corticosteroid administration greatly increases the risk for peptic ulcers.35 The gastrointestinal tract is the shock organ of dogs and therefore, hypovolemia, shock, and sepsis are common, but frequently overlooked, causes of gastric ulceration. Thus all critically ill patients should be considered at risk for developing gastric ulcers.36 Gastrinoma (see 9.4.3) arising from the

Figure 4.13:
Large ulcer at the incisura angularis. An 8-year-old male Basset hound presented with a 7-week history of hematemesis. During gastroscopy a peptic ulcer with a hard rim could be seen. Histopathology of the biopsies revealed the cause of this ulcer to be a gastric adenocarcinoma.
Table 4.4: Causes of peptic ulcers in dogs and cats
Drugs
■ NSAIDs
■ Corticosteroids (only when concurrent risk factors are present; e. g., NSAID administration)
Infiltrative Disease
■ Gastric neoplasia
■ Pythiosis in endemic areas
■ Inflammatory bowel disease
Metabolic Disease
■ Hepatopathy
■ Renal failure (common in older cats)
Gastric hyperacidity
■ Gastrinoma
■ Mast cell tumor (rarely causes gastric ulcers)
■ APUDoma
Other Causes
■ Chemical toxins
■ Disseminated intravascular coagulation
■ Foreign objects (might worsen pre-existing gastritis or ulceration)
■ Hypovolemia
■ Pancreatitis
■ Septic shock
■ Stress?
APUDoma = amine precursor uptake and decarboxylation tumors
pancreas can secrete excessive amounts of gastrin and the resultant hyperacidity may also cause peptic ulceration.
Large ulcers in the pyloric antral region, often near the incisura, are commonly seen in dogs with gastric tumors (Figure 4.13). In a study on cats, 14 of 33 peptic ulcers were due to gastric neoplasia, mostly gastrointestinal lymphoma or gastric adenocarcinoma.31
4
Clinical signs
Clinical signs of peptic ulceration are poorly defined. Chronic vomiting is probably the most frequent sign, with or without hematemesis. Unlike humans, dogs do not secrete acid continuously and blood in the vomitus does, therefore, not always appear digested. Melena and pale mucous membranes may also be observed if bleeding is severe. Inappetence and anorexia are also common. Because of the important pathogenic role of medications, a careful history should include specific questions about any medications the owner may be administering to the animal.
Any changes in routine blood work are nonspecific. However, routine blood work is used to rule out other causes of vomiting. Chronic blood loss may result in anemia that can sometimes be non-regenerative and appear typical for iron deficiency (i.e., hypochromic, microcytic). Blood biochemistry results may show some electrolyte abnormalities as a consequence of profound vomiting.
Minor blood loss from gastric ulceration may not lead to gross melena and a fecal occult blood test may be required to identify such cases. However, some fecal occult blood tests can be affected by red meat in the diet. Fecal occult blood test kits are based on one of two different test principles. Guaiac-based tests contain guaiaconic acid, which when oxidized by hemoglobin leads to the development of a blue quinone. O-toluid- ine-based tests contain tetramethylbenzidine, which when oxidized by hemoglobin also leads to the generation of a blue compound. Both kit types can give positive test results when exposed to red meat or peroxidase-rich foods, such as turnip and cauliflower, present in the diet. However, in one study an o-toluidine-based test was associated with far fewer false positive results due to diet than a guaiac-based test. In another study, the same o-toluidine-based test was also slightly more sensitive than a guaiac-based test at 12 hours after oral administration of hemoglobin. But ideally patients should be fed a meat-free diet for at least 3 days prior to testing.37
Although gastroscopy is by far the best tool to diagnose gastric ulcers, this is often not necessary if the history (i.e., administration of NSAIDs, hematemesis) and clinical findings are indicative of gastric ulcers. Diagnosis can also be made based on contrast radiographic studies or exploratory laparotomy. The latter has the disadvantage that the gastric mucosa is not easily evaluated from the exterior of the stomach.
Treatment
The goals of therapy of gastric ulceration are to eliminate clinical signs, complications, and relapses (Table 4.5). To that end, it is vital to avoid ulcerogenic drugs. If the peptic ulcer might be due to decreased mucosal blood flow, the animal should be given sufficient amounts of intravenous fluids. Antacids act by neutralizing gastric acid. Calcium carbonate (CaCO3), sodium bicarbonate (NaHCO3), magnesium hydroxide (Mg[OH]2), or aluminum hydroxide (Al[OH]3) all contain an H+-binding group. The neutralizing reaction with gastric acid produces water and a neutral salt. Antacids are also of benefit in that they bind to bile acids, decrease pepsin activity in the stomach, and stimulate the secretion of endogenous prostaglandins. However, the requirement of frequent dosing and poor palatability make antacids an inconvenient choice for animals.
The cornerstone of peptic ulcer therapy is the reduction of gastric acid secretion as Schwartz' dictum from 1910 “no acid, no ulcer” remains valid today. There are a variety of drugs available and the two most commonly prescribed drug classes in veterinary medicine are histamine2-receptor antagonists and proton pump inhibitors. H2-receptor antagonists (H2-RA) block the secretion of gastric acid by blocking histamine H2 receptors located on the surface of acid-producing parietal cells within the gastric glands (Figure 4.14). Cimetidine and ranitidine are used equally frequently in veterinary medicine. While ranitidine is 5 to 12 times more potent than cimetidine and has a longer half-life allowing for a decreased frequency of administration, a recent study indicated that ranitidine at the
Table 4.5: Therapeutic agents used for gastric diseases
| Generic name | Class of drug | Dosages |
| aluminum hydroxide | antacid | dogs: 100-200 mg PO q 4-6 h cats: 50-100 mg PO q 4-6 h |
| bismuth subsalicylate | mucosal protectant | 0.25-2.0 ml/kg PO q 4-6 h |
| cimetidine | H2-receptor antagonist | 5-10 mg/kg PO, IV q 8 h |
| famotidine | H2-receptor antagonist | 0.5-1 mg/kg PO, IV q 12-24 h |
| misoprostol | prostaglandin analogue | 2-5 μg∕kg PO q 8-12 h |
| nizatidine | H2-receptor antagonist prokinetic agent | 5 mg/kg PO q 24 h |
| omeprazole | proton-pump inhibitor | 0.7 mg/kg PO q 24 h |
| ranitidine | H2-receptor antagonist prokinetic agent | 1-2 mg/kg PO, IV q 12 h |
| sucralfate | mucosal protectant | 0.5-1 g PO q 8 h |
PO = oral administration; IV = intravenous administration
regular dose (2 mg/kg IV q 12 h) was not different from saline administration in increasing the intragastric pH. In comparison, famotidine (0.5 mg/kg IV q 2 h) was significantly more effective than saline.38 Another H2-RA is nizatidine which, together with ranitidine, also possesses prokinetic activity in the stomach. In addition to their blockade of the histamine H2 receptors of parietal cells, the H2-RA increase the luminal secretion of bicarbonate and mucus as well as raising mucosal blood flow. These effects may be related to a stimulation of prostaglandin synthesis. In addition, it has been suggested that cimetidine increases in vitro cell-mediated immunity by blocking the H2 receptors on T lymphocytes. Cimetidine decreases hepatic perfusion and is recognized as an inhibitor of hepatic P-450 and P-488 enzymes.39 Drugs metabolized by these enzyme systems may be cleared more slowly and may reach a higher plasma concentration (e.g., cyclosporin) when administered together with cimetidine. Other histamine H2-receptor antagonists do not show this interaction and may be preferred in animals receiving multiple drugs.
Omeprazole, a substituted benzimidazole, belongs to the class of proton pump inhibitor drugs (PPIs). By blocking the H+/ K+-APTase enzyme at the luminal membrane of the parietal cell (Figure 4.14), acid secretion is inhibited regardless of the secretagogue (i.e., histamine, gastrin, or acetylcholine). Compared with cimetidine, omeprazole is about 20 times more potent and has a longer duration of action because it accumulates in a pH-dependent manner. Newer PPIs include lansoprazole or pantoprazole, but experience with these newer PPIs in veterinary patients is limited.38
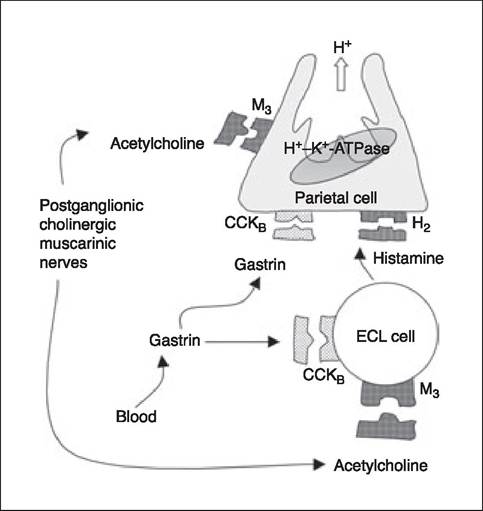
Figure 4.14:
Physiological mechanism of gastric acid secretion. The parietal cell contains receptors for gastrin (CCKB), acetylcholine (M3), and histamine (H2). In addition, gastrin and acetylcholine can also interact with their receptors on enterochromaffin-like cells (ECL-cells) and release histamine.
Sucralfate is a gastromucosal protectant. It is a basic salt of a sulfate disaccharide with many aluminum hydroxide groups. Sucralfate dissociates after oral ingestion to sucrose octasulfate and aluminum hydroxide, which buffers H+. Sucrose octasulfate reacts in the stomach with hydrochloric acid to form a paste-like complex that has greater affinity for damaged tissue than the normal mucosa. This adhering complex prevents further damage of the gastric mucosa by pepsin, acid, or bile. Sucralfate may also have some cytoprotective effects, possibly by stimulation of prostaglandin synthesis. Systemic absorption of sucralfate is minimal, and it is extremely well tolerated. Since sucralfate is effective at an acidic to almost a neutral pH, antisecretory drugs can be used concurrently. Other, orally administered drugs, however, should be given 2 hours apart as sucralfate can affect their absorption.39
Finally, misoprostol is a synthetic analog of prostaglandin E1 (PGE1). Although orally administered, it has to be absorbed into the circulation to be effective. Its effect is the same as those of endogenous prostaglandins. Although the prophylactic effect of misoprostol in dogs receiving corticosteroids or undergoing spinal surgery is debatable, this drug appears to be of little use in dogs that already have a peptic ulcer. Misoprostol can cause abortion and should be avoided in pregnant animals. Also, women in child-bearing age should use gloves when administering misoprostol to their pet.40
Other means of decreasing gastric acid concentration have been developed, but are not yet available for routine use (e.g., gastrin-receptor antagonists, gastrin-releasing peptide receptor antagonists). A class of drugs which might be of future interest is the class of potassium-competitive acid blockers (P-CABs). These drugs block the action of the H+-K+-ATPase by competing with K+.41 Soraprazan and raveprazan are currently under investigation, but no information in dogs or cats is yet available.
4.3.4