hepatic AND PANCREATIC NEOPLASIA
Nonhematopoietic Primary Liver Tumors in Dogs
Background
Primary hepatic neoplasia is uncommon in the dog. When neoplasia is found in the liver, it is more likely to be due to metastasis.
The most common histologic types of primary liver tumors include hepatocellular adenoma, hepatocellular carcinoma, bile duct (cholangiocellular) carcinoma, and hepatic carcinoid. Tumor types found less frequently include bile duct cystadenoma, cholangioma, fibroma, fibrosarcoma, hemangioma, hemangiosarcoma, leiomyosarcoma, liposarcoma, myxosarcoma, and osteosarcoma. One study evaluated 110 liver tumors and found that slightly more than 50% were primary hepatocellular carcinomas, with bile duct carcinomas and cystadenomas seen less frequently. Liver carcinomas (hepatocellular or bile duct) affect older dogs with a mean age between 10 and 12 years, whereas hepatic carcinoids occur in younger patients with a mean age of 8 years. In a series of 18 dogs with primary hepatocellular carcinomas, males were affected more often. Another series found that female dogs were more likely to have a bile duct carcinoma.Clinical Parameters
Dogs with liver tumors often have nonspecific signs of illness. However, the most common signs associated with a primary liver tumor include a palpable abdominal mass localized to the region of the liver, anorexia, weight loss, depression, weakness, vomiting, and ascites. Less often, polyuria and polydipsia, pyrexia, poor hair coat, ataxia, diarrhea, or central nervous system signs due to hepatoen- cephalopathy or hypoglycemia may occur.
Clinical Work-up
Hematologic abnormalities can be helpful in assessing the patient with a liver mass. Abnormal platelet function, hypoproteinemia, hypoglycemia, elevated liver enzyme levels (especially aspartate aminotransferase [AST], alanine aminotransferase [ALT], and alkaline phosphatase [ALP]) and less commonly hyperbilirubinemia have been reported in dogs with liver tumors.
In one study all dogs with hepatocellular carcinomas had elevated levels of ALT and ALP. These parameters were less frequently elevated in dogs with metastatic disease. The use of fasting serum bile acid concentrations does not provide compelling evidence of neoplasia. An enzymatic kit to detect alpha fetoprotein was used to distinguish different liver tumor types before biopsy. Levels of alpha fetoprotein were highest in dogs with cholangiocarcinoma and hepatocellular carcinoma; however, this assay is probably best used in conjunction with a complete blood count, biochemical profile, urinalysis, diagnostic imaging of the chest and abdomen, and biopsy of the lesion.Abdominal radiography, contrast procedures, and ultrasonography are most commonly employed to confirm a diagnosis of liver cancer. Other useful imaging methodologies include hepatoscintigraphy, CT, and magnetic resonance imaging (MRI). A radiographic finding that supports a diagnosis of a hepatic mass is a right cranioventral abdominal mass that displaces the gastric shadow to the left and displaces the small intestine caudally. In some instances, peritoneal fluid from ascites or carcinomatosis may obscure radiographic detection of the mass.
Ultrasonography is more precise than radiography in detecting the site of origin of an abdominal mass and also enables the examination of hepatic parenchyma, biliary system, perihepatic structures, and portal and hepatic vascular supply. A hepatic tumor may appear as a large, well-circumscribed mass extending from the liver margins with an echogenicity that is usually more mixed than normal liver (see examples in Chapter 2). Hepatic tumors may also be found in multiples or of homogeneous echogenicity. Areas of edema, necrosis, fibrosis, neovascularization, hemorrhage, and inflammation all contribute to the variable appearance of liver tumors on ultrasound. Differentiating between histologic type and benign versus malignant neoplasms is usually not possible with ultrasound examination alone.
For this reason, hepatic aspiration or biopsy is commonly required to make a definitive diagnosis. Prebiopsy evaluations should include a review of the patient's overall status, risk for hemorrhage or impaired wound healing, and liver size. A very ill patient may not be a good anesthetic candidate, in which case less-invasive biopsy techniques with the use of local anesthetic would be a better choice.A coagulation profile including prothrombin time (PT), partial thromboplastin time (PTT), fibrin degradation products (FDPs), fibrinogen content, and platelet count should identify those patients at increased risk for hemorrhage. At a minimum, packed cell volume (PCV), total solids (TS), estimate of platelet count, buccal mucosa bleeding time (BMBT), and activated clotting time (ACT) should be performed.Techniques for obtaining neoplastic material include fine-needle aspiration (percutaneous, blind), keyhole biopsy (percutaneous, blind), ultrasound- guided fine-needle aspiration or biopsy, transthoracic biopsy, laparoscopic biopsy, or exploratory celiotomy. See the References for hepatic aspiration and biopsy techniques. One study found a poor correlation between cytologic and histologic findings for liver disease, with an agreement of only 44% for hepatic tumors in particular. Ultrasound-guided biopsy with a 14-gauge Tru-Cut biopsy instrument usually provides a definitive diagnosis and is the procedure of choice for diffuse lesions, zonal lesions that involve all hepatic lobules or acini, or focal lesions defined by ultrasound. However, with lesions other than those mentioned, wedge liver biopsy samples taken during laparotomy provide the pathologist with the best specimen for evaluation and allow the surgeon to examine the liver during the procedure as well.
Staging of liver tumors should be performed with chest radiographs and abdominal ultrasound to detect hepatic lymphadenopathy, other organ involvement, or lesions in multiple lobes. Of 49 dogs with hepatocellular carcinoma, 30 (61%) were initially diagnosed to have a solitary mass in only one liver lobe,but 24 of the 30 (80%) actually had lesions in other lobes.
A solitary liver mass was the most common presenting sign for hepatocellular carcinoma in other studies. Regardless of histologic type, metastasis is common for liver tumors. In a study of 57 dogs with liver tumors, metastasis to the regional lymph nodes (14 dogs), lungs (14 dogs), or peritoneal surfaces (7 dogs) occurred in 35 (61%) cases. In another study, spread to the lungs was less common and occurred in only 2 of 13 dogs with hepatocellular carcinoma and bile duct carcinoma. Large, solitary hepatocellular carcinomas are less likely to metastasize than are multiple lesions.Thirteen of 14 dogs (93%) with multiple or diffuse lesions had metastasis, whereas 11 of 30 dogs (37%) with solitary liver masses had evidence of metastasis. The size of a liver mass has little influence on prognosis, although it is speculated that large lesions that have not led to the demise of the patient are more likely to behave in a less aggressive fashion. Further, the degree of invasion and presence of metastasis are more likely to be prognostic indicators than size. Predictably dogs with solitary liver tumors are probably the best candidates for surgical resection and control of disease, whereas dogs with multiple lesions have a less favorable prognosis.Treatment
Up to 75% of the liver can be resected with negligible compromise to liver function, and complete regeneration occurs within 6 to 8 weeks. Several techniques are described in the literature, including partial lobectomy, complete lobectomy, and partial hepatectomy. The most commonly used procedures are partial and complete lobectomies. For benign liver masses—such as hepatocellular adenoma, cholangioma, fibroma, and bile duct cystadenoma—surgical excision has the greatest potential for definitively controlling disease.
Surgery is also the treatment of choice for dogs with hepatocellular carcinoma that involves one or two liver lobes (Figure 11-12). In a report of 18 dogs with solitary hepatocellular carcinoma, 16 were resected with single lobectomies and 2 by partial hepatectomy.
At the time of publication in that study, 8 dogs had died with a mean survival time of 306 days (range, 1 to 548 days), and 10 dogs were still alive with a mean survival time of 377 days (range, 195 to 1025 days).The success of treatment for other types of hepatic neoplasms is less defined. In a report of two dogs with bile duct carcinoma and adenocarcinoma treated with partial hepatectomy, both dogs had survival times of 6 months. A hepatic mesenchymoma treated by excision recurred 4 months after surgery in another dog.
It is unknown whether chemotherapy is valuable as an adjunctive treatment; however, many drugs have been used (5-fluorouracil [5-FU], cisplatin, actinomycin D, and mitoxantrone). Occasional responses have been seen with doxorubicin in humans with hepatocellular carcinoma.
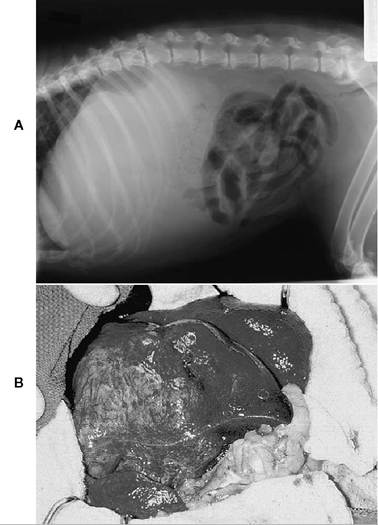
Figure 11-12 Hepatic carcinoma in a dog. A, Radiograph of a 7-year-old, mixed breed, female dog with a tumor of the liver.The mass was identified on an annual physical examination.The biochemical profile was completely normal, suggesting slow growth of the tumor and incomplete involvement of the liver. Resection resulted in a cure of this condition. B, The tumor was a low- grade hepatic carcinoma localized to one liver lobe. This tumor was removed, and the dog was noted to be free of the tumor and all evidence of clinical signs relating to this disease for at least 2 years.
Hematopoietic Liver Tumors in Dogs
Background
Lymphoma is the most common hematopoietic tumor with liver involvement in the dog, followed by a variety of myeloproliferative neoplasias and mast cell tumors.
Clinical Parameters, Work-up, and Treatment
Clinical signs result from the infiltration and disruption of liver function. Diagnosis and treatment for these tumors are similar to that which is described in the section on tumors of the GI tract.
Metastatic Liver Tumors in Dogs
Background
Hemangiosarcoma, islet cell carcinoma, pancreatic carcinoma, and fibrosarcoma are the most common tumor types that metastasize to involve the liver.
Less commonly osteosarcoma, transitional cell carcinoma, mammary carcinoma, intestinal carcinoma, nasal carcinoma, pheochromocytoma, and thyroid carcinoma have been reported.Clinical Parameters, Work-up, and Treatment
Clinical signs for metastatic disease are usually a result of disruption of liver function. The clinical work-up should be the same as that described for primary liver cancer. However, treatment will differ between tumor types and is usually directed at palliation rather than curative intent.
Nonhematopoietic Primary Liver Tumors in Cats
Background
In cats, biliary carcinoma is the most common primary liver tumor, followed by hepatocellular carcinoma, hemangiosarcoma, and other sarcomas. An evaluation of 107 cats with nonvascular, nonhematopoietic liver tumors found 57 intra- hepatic bile duct tumors, of which 34 (60%) were benign. Hepatocellular carcinoma is less common in cats than in dogs and accounted for 25% of primary feline liver tumors. Tumors of the extrahepatic bile duct (9 of 107) or gallbladder (4 of 107) are usually malignant. Most cats affected with bile duct tumors are middle-age, ranging upward in age from 6 years. In a series of 21 cats with liver tumors, affected animals were older than 10 years of age. Sex predilection for bile duct tumors has not been resolved, because one study found male cats to be overrepresented, whereas another found the opposite to be true. In both studies, bile duct tumors were more common in domestic short hairs than in Siamese. The median age of cats affected with hepatocellular carcinoma is 11 years, and males are more commonly affected (11 of 17 [65%]). As is the case with biliary tumors, hepatocellular carcinomas also affect domestic short hairs more frequently. FeLV does not seem to play a role in nonhematopoietic liver tumors. Hepatic myelolipoma, an uncommon tumor consisting of adipose tissue and bone marrow elements, has been associated with diaphragmatic hernias in cats and may be associated with chronic hypoxia or trauma to the liver.
Clinical Parameters
Clinical signs of liver tumors include anorexia, lethargy, and weakness. Less commonly a patient may have presenting symptoms of vomiting, diarrhea, polydipsia, and ascites. In most cats a mass in the cranial abdomen or hepatomegaly can be detected on palpation.
Clinical Work-up
Hematologic abnormalities are less commonly detected in cats than in dogs with liver tumors. Liver enzyme elevations are less likely (possibly due to the short serum half-life of ALP in the cat) and are thought to be nonspecific for liver cancer. In cats with cystadenomas the most common abnormality is azotemia, without bilirubine- mia and elevated liver enzyme levels, which is more indicative of another disease process.
Chest radiographs and abdominal ultrasonography are extremely valuable in assessing cats with a liver mass. Benign liver masses are most often cystic with several different compartments, whereas malignant tumors tend to be multilobular. One study found that benign bile duct adenomas involved multiple liver lobes in 50% (8 of 16) of the cases, whereas the majority (7 of 9 [78%]) of bile duct carcinomas were widespread throughout the liver. Metastasis to the peritoneal surfaces, hepatic lymph nodes, and lungs is commonly encountered with malignant bile duct tumors in cats; less common sites include thoracic lymph nodes, diaphragm, spleen, urinary bladder, GI tract, and bone. Malignant transformation from benign to malignant lesions has also been reported. Of 18 cats with hepatocellular carcinoma, however, only 5 (28%) had evidence of metastasis to the hepatic lymph nodes, lung, or spleen.
Aspiration or biopsy (and prebiopsy evaluation) should be performed as outlined in the section on primary liver tumors in dogs.As is the case in dogs, cytologic evaluation from fine-needle aspiration has only a 44% correlation with histopathologic findings and should be interpreted with caution. In the case of cystadenomas, aspiration of cystic fluid characteristically produces a yellow to colorless transudate with a specific gravity of 1.001 to 1.008 and protein concentration less than 2 gm/dl, with the most common cell type being a macrophage. Although this finding is not diagnostic for hepatobiliary cystadenomas, it will permit one to rule out abscesses, hematomas, and parasitic cysts.
Treatment
In those cases where the liver mass is confined to a resectable portion of the liver and there is no evidence of metastasis, surgical resection is indicated.
Benign hepatobiliary cystadenomas prevail as the tumor type in older cats, and for this reason surgical resection with long-term control of disease is often possible (Figure 11-13). Surgical resection of a hepatobiliary cystadenoma involving both the left medial and lateral lobes of the liver resulted in long-term survival (over 18 months), with the patient still alive at time of publication. Long-term survivals, ranging from 12 to 44 months, with no postoperative complications were reported in five cats with surgical resections of hepatobiliary cystadenomas. This study also found that although complete surgical excision is preferable, even partial resection merits a good prognosis. In another report a 16-year-old cat lived 27 months after surgical excision of a myelolipoma and had no tumor recurrence.
To date there are no reports of adjuvant chemotherapy in cats with malignant tumors of the liver. Few data exist on the efficacy of chemotherapeutic
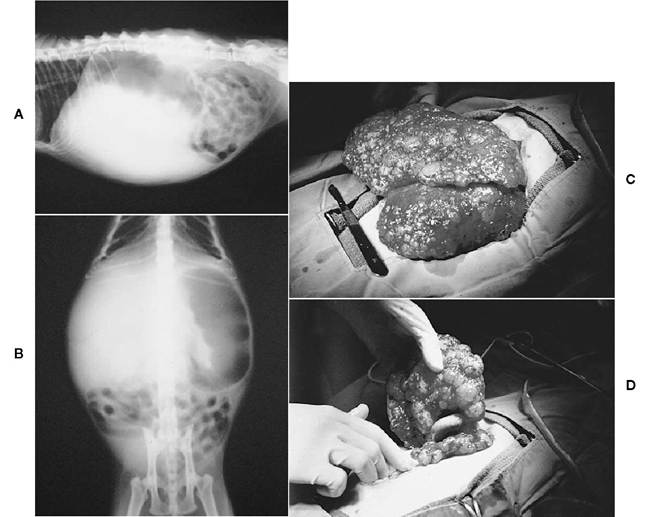
Figure 11-13 Biliary cystic hyperplasia in a 15-year-old cat.The cat was asymptomatic, and results of a complete blood count and biochemical profile were normal. A, Lateral and, B, ventrodorsal survey abdominal radiographs showing marked hepatomegaly and displacement of the stomach dorsally and to the left. C and D, Appearance of the liver at laparotomy. Multiple (polycystic) hepatic cysts were present throughout the liver. Treatment involved removal of two liver lobes to decrease the size of the liver.The polycystic disorder appears to be inheritable and runs a benign course in affected patients. (Courtesy Dr. Todd R. Tams.)
treatment of dogs with primary hepatic tumors. Doxorubicin and 5-FU have been recommended by some; however, efficacy is unknown.
Hematopoietic Liver Tumors in Cats
Background
Lymphoma is the most common hematopoietic tumor with liver involvement in the cat, followed by a variety of myeloproliferative neoplasias and mast cell tumors.
Clinical Parameters, Work-up, and Treatment
Clinical signs result from the infiltration and disruption of liver function. Diagnosis and treatment for these tumors are similar to that which is described in the section on tumors of the GI tract.
Metastatic Liver Tumors in Cats
Background
Metastatic liver disease is less common in the cat. Although no specific tumor type is overrepresented, the most common metastatic tumor types include pancreatic carcinoma, intestinal carcinoma, and renal carcinoma.
Clinical Parameters, Work-up, and Treatment
Clinical signs for metastatic disease are usually a result of disruption of liver function. The clinical work-up should be the same as that described for primary liver cancer. However, treatment will differ between tumor types and is usually directed at palliation rather than curative intent.
Exocrine Pancreas Tumors in Dogs
Background
Exocrine pancreatic tumors are uncommon.These tumors do not show a sex predilection and occur in older dogs. Cocker spaniels may be overrepresented, because this breed was seen in 3 of 14 cases reported in one study. Another series found that only spaniel breeds were affected in the cases reported.The most common histologic type is carcinoma arising from the ductal epithelium, with adenocarcinoma—which arises from the acinar cell—being the second most common.
Clinical Parameters
Nonspecific clinical signs such as weight loss, depression, and anorexia are often seen with pancreatic tumors. Although these tumors are thought to cause vomiting, this is a relatively uncommon finding; if vomiting does occur, it is usually at the terminal stages of disease when extrahepatic bile duct obstruction secondary to liver metastasis has occurred. Abdominal palpation may reveal a mass in the cranial abdomen, and abdominal fluid may also be present. In a report of three dogs with pancreatic carcinoma found on necropsy, panniculitis with subsequent subcutaneous swelling and shifting leg lameness over a period of months were the only clinical signs reported.
Clinical Work-up
A complete blood count, biochemical profile, urinalysis, chest and abdominal radiographs and abdominal ultrasound should be performed to evaluate the general health status of the patient, stage for metastasis, and assess the primary mass. In dogs with pancreatic carcinomas, half are solitary masses and the rest consist of multiple nodules throughout the pancreatic parenchyma. Metastases are common, occurring in over 92% of cases. The liver is most commonly affected (12 of 13) with the omentum (6 of 13) and regional lymph nodes (4 of 13) less frequently affected. Less commonly other visceral sites are sites for metastasis. For instance, in one case of pancreatic carcinoma associated with diabetes insipidus, metastasis to the pituitary gland was detected. Although it is unusual, no evidence of metastasis was seen in one series of three cases of pancreatic carcinoma where panniculitis, subcutaneous swelling, and shifting leg lameness were clinically apparent for months. Blood work revealed marked elevations in levels of serum lipase and amylase in one of these cases, although no evidence of pancreatitis was seen. Hematologic abnormalities associated with pancreatic carcinoma may include elevated serum amylase and lipase levels; lipase levels of 25 times greater than normal are most likely to be diagnostic for exocrine pancreatic carcinoma.
Ultrasonography can be useful in detecting a pancreatic mass if the pancreas can be visualized despite shadowing from gas-filled GI structures. This will also permit evaluation of the liver for metastases, although definitive diagnosis requires biopsy.
Treatment
If a pancreatic mass is detected in a stable patient and there is no evidence of metastasis, exploratory laparotomy with intent to surgically resect the mass may be considered. However, due to the high rate of metastasis, the prognosis should be considered poor for control of disease.
Chemotherapy is not considered effective in the treatment of pancreatic carcinoma because there is a high incidence of de novo resistance to cytotoxic drugs.
Endocrine Pancreas Tumors in Dogs
Insulinoma (Beta Cell Tumor, Islet Cell Tumor)
Background
Insulinomas are functional secreting tumors that arise from the islet cells in the endocrine pancreas. In addition to the secretion of insulin and its precursors, insulinomas are now known to secrete pancreatic polypeptide, somatostatin, glucagon, serotonin, gastrin, and corticotropin. These tumors are most commonly carcinomas and most often present late in the course of disease with signs attributable to the resultant hypoglycemia. Insulinomas occur in older dogs, with no sex predilection reported.
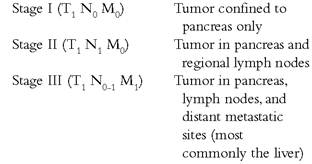
Metastasis is common with insulinomas. At the time of diagnosis, evidence of metastasis is present in approximately 36% of the cases, with the most common sites being the lymph nodes and liver. Spread to the duodenum, mesentery, omentum, spleen, spinal cord, and kidney have also been reported.
The WHO staging scheme is as follows:
Clinical Parameters
Clinical signs of insulinomas include seizures, collapse, generalized or caudal weakness, lethargy, ataxia, muscle fasciculations, bizarre behavior, polyphagia, exercise intolerance, shaking/trem- bling, polyuria/polydipsia, and weight gain. These clinical signs can be explained by hyperinsuline- mia with resultant hypoglycemia and release of counter-regulatory hormones (catecholamines and glucagon in the early phase and cortisol and growth hormones in the later phase of disease). Because of the patient's ability to adjust to a chronic state of hypoglycemia, signs of hypoglycemia are often not seen, even with extremely low blood glucose levels. The rate of decrease in blood glucose, as well as the duration of hypoglycemia, is considered important in the development of clinical signs.
There are two types of presenting clinical signs: neuroglycopenic (seizures, weakness, ataxia, and lethargy) and sympathetic (behavioral changes, shaking/trembling, and muscle fasciculations). Neurologic signs are due to the reliance of the central nervous system on diffusion for glucose uptake (which is predictably low in periods of hypoglycemia) and its inability to utilize other forms of energy, such as fatty acids and ketone bodies. The sympathetic signs are related to an increased discharge of counter-regulatory hormones. There is no correlation between the severity of clinical signs and the stage of disease, however.
Clinical Work-up
Basic blood work and urinalysis, chest and abdominal radiographs, and abdominal ultrasound should be performed to diagnose and stage dogs with suspected insulinomas, to rule out other causes of hypoglycemia, and to evaluate for the presence of any concurrent disease. Blood work, urinalysis, and radiographs are usually unremarkable in the patient with insulinoma, with the exception of hypoglycemia and, rarely, elevated liver enzymes. Abdominal ultrasound infrequently detects a mass on the pancreas, but other organ metastases and/or mesenteric lymphadenopathy may be evident.The diagnosis of insulinoma is based on demonstration of hyperinsulinemia in the face of hypoglycemia. There are several means by which one can achieve this, including the insulin-glucose, glucose-insulin, and amended insulin-glucose ratios. For the most part these ratios are not considered diagnostic because they are associated with a high number of false-positive results. For this reason, performing a paired insulin and glucose test is considered to be the most reliable method of diagnosing an insulinoma. This test is further described below.
One study describes the use of chromogranin A (CgA) and neuron-specific enolase (NSE) as a marker for cannine and feline pancreatic islet cell tumors.The study found these assays to be sensitive in detecting tumors of neuroendocrine origin. Another report describes the use of fructosamine measurement, which may be helpful in conjunction with insulin measurement in diagnosing an insulinoma. Provocative testing has been described in the literature. Such tests include glucagon tolerance, glucose tolerance, tolbutamide tolerance, L-leucine, oral glucose tolerance, epinephrine tolerance, and the calcium infusion test. These tests use the administration of potentially dangerous substances and are expensive, time consuming, and most importantly not as accurate as the paired insulin- glucose tests.
Preferred Test Protocol. Most dogs will become hypoglycemic within 8 to 10 hours of fasting. Dogs should be fed at 5:00 PM, 8:30 PM, and midnight, then fasted thereafter. Blood glucose should be monitored starting at 8:00 AM the next morning. When serum glucose is 60 mg/dl, serum should be saved for insulin levels. This test will detect hyperinsulinemia in approximately 77% of patients.The remaining 23% will show insulin levels in the normal range, which is highly suggestive for but not diagnostic of insulinoma, and the test should be repeated.
Treatment
Surgical resection is the treatment of choice for insulinoma. Both lobes of the pancreas are affected with equal frequency, with the body of the pancreas affected less commonly. In a study of 39 dogs with insulinoma comparing surgical to medical treatment, 26 underwent exploratory celiotomy and partial pancreatectomy and the median survival was 381 days (range, 20 to 1758 days). Thirteen were treated medically and had a median survival of 74 days (range, 8 to 508 days). Twelve of the 13 dogs (92%) died or were euthanized because of clinical signs resulting from hypoglycemia.
Medical Management. Medical management should be approached in a stepwise fashion. Initially a reduction in exercise and concomitant dietary changes (frequent small feedings containing high protein and complex carbohydrates) is employed. Prednisolone can be introduced as signs of hypoglycemia worsen. Prednisolone has antiinsulin and hyperglycemic effects starting at a dose of 0.11 mg/lb (orally twice daily); the dose can be increased as needed up to 0.5 mg/lb (orally twice daily) when iatrogenic Cushing's disease becomes a risk.
Diazoxide has several beneficial effects in the treatment of insulinomas. It inhibits cell uptake of glucose, blocks calcium entry into beta cells, catalyzes the breakdown of glycogen to glucose, and enhances glucose synthesis. The initial dose is 2.3 mg/lb (orally twice daily), which may be increased to 13.6 mg/lb (orally twice daily) if required to control signs of hypoglycemia. Potential side effects include GI toxicity (vomiting, diarrhea, inappetence), hyperglycemia, diabetes, myelosup- pression, and hypernatremia. Hydrochlorothiazide (0.9 to 1.8 mg/lb, orally once daily) can be added to potentiate the effects of diazoxide.
Octreotide acetate (somatostatin) can be given at 10 to 20 μg subcutaneously two to three times daily. Its efficacy is variable in the small subset of patients treated to date. Calcium channel blockers may be useful.Alloxan (29.5 mg/lb intravenously with concurrent fluid therapy) has been described in a small number of dogs. Streptozotocin, a nitrosurea compound, has also been reported in two dogs but is extremely nephrotoxic, can be hepatotoxic, and should be considered as a rescue agent only. Similarly, doxorubicin and streptozotocin, carboplatin, cyclophosphamide, tubercidin and mithramycin have all been used in humans, but with variable effects, and there is no data on canine patients to date. Radiation therapy has not been reported in dogs. The prognosis for long-term control of insulinoma in the dog is grave in those with metastatic disease, although the short-term control is good.Young dogs and those with very high serum insulin concentrations have shorter survival times. In one study the overall survival for dogs undergoing surgery for insulinoma was 10 to 14 months. Dogs in stages I and II tend to have similar survival times, although dogs in stage II have recurrence of clinical signs earlier. More than 80% of dogs in stage III have recurrence of disease at 1 year. There is little doubt that surgery should be recommended for patients with suspect insulinomas and that many patients require concurrent medical management.
Glucagonoma
Background
A rare tumor of the pancreatic alpha-islet cells, glucagon-secreting tumors have been described in the dog in a number of case reports. A review of the characteristic syndrome, referred to as glucagonoma syndrome, cites no sex predilection.
Clinical Parameters and Work-up
Clinical signs described in the literature include skin lesions, referred to as superficial necrolytic dermatitis (SND) or metabolic epidermal necrosis (MEN).These lesions are characterized by mild to marked hyperkeratosis and fissuring of the footpads, erythema, and crusting plaques on the oral cavity, muzzle, limbs, abdomen, and genital areas. Staging for glucagonoma should include basic blood work, urinalysis, and thoracic and abdominal imaging. Biochemical abnormalities are variable and may include hyperglycemia, elevated liver enzyme levels, and nonregenerative anemia. A case report on one dog found hyperglucagonemia, hyper- insulinemia, and hypoaminoacidemia. Ultrasound findings are usually unremarkable, although a pancreatic mass was suggested in one of seven dogs reported.
Treatment
Surgical excision is the treatment of choice. Metastasis is common to the liver (three of four dogs [75%]) and/or mesenteric lymph node (one of four dogs [25%]). However, survival and resolution of disease is reported in one case.The major postoperative surgical complication in reported cases was bile duct obstruction and pancreatitis.
Medical management includes symptomatic therapy with intravenous amino acid administration. A 10% solution of crystalline amino acid solution, approximately 11.4 ml/lb of body weight, is administered over 6 to 8 hours and repeated every 7 to 10 days. Oral nutritional support with a high- quality protein diet should also be instituted. Supplementation with egg yolks (three to six daily), zinc, essential fatty acids, and prednisone have also been described. Somatostatin analogues have been used in humans and have resulted in remissions, although these drugs have not been evaluated in dogs.
Gastrinoma
Background
A rare tumor of the pancreatic islets, gastrinomas secrete gastrin and result in hypertrophic gastritis and subsequent peptic ulcers. This syndrome is referred to as Zollinger-Ellison syndrome. These tumors are usually small, discrete masses within the pancreas. Most are malignant and metastasize to the regional lymph nodes and liver.
Clinical Parameters and Work-up
Clinical signs of gastrinomas include chronic vomiting and weight loss.These signs are related to the hypersecretion of gastrin and consequent ulceration. A complete staging scheme should include a complete blood count, biochemical profile, urinalysis, and thoracic and abdominal imaging. Diagnosis involves the measurement of serum gastrin, demonstration of gastric hypertrophy and ulceration (via endoscopy), and increased secretion of gastric acid. Provocative testing with secretin or calcium is usually only indicated when gastrin levels are minimally elevated. A novel method of diagnosis described is the use of somatostatinreceptor scintigraphy.
Treatment
Although the course of gastrinomas tends to be chronic, early surgical resection can be attempted. Medical management is symptomatic and includes an ^-receptor antagonist or omeprazole, and octreotide acetate. Ulcer therapy is described in detail in Chapter 5. Survival data is sparse; however, one dog treated with octreotide (10 to 20 μg subcutaneously three times daily) lived for 10 months, and two dogs treated with a combination of antacids and octreotide lived for 4.5 months.
Pancreatic Polypeptidoma (Vasoactive Intestinal Peptidoma, Somatostatinoma)
Background
Pancreatic polypeptidoma is a rare endocrine tumor of the pancreatic islet cell; pancreatic polypeptide hormone is elevated in 77% of dogs with endocrine polypeptideomas.
Clinical Parameters and Work-up
Clinical signs of vomiting, hypertrophic gastritis, and duodenal ulceration characterize this tumor. Basic blood work and urinalysis, chest and abdominal radiographs, and abdominal ultrasound should be performed to assess general health status, possibly diagnose a pancreatic mass, and stage the disease. These tests are usually unremarkable. Because the signs are similar to those seen with gastrinoma, this is one case that would merit provocative testing with secretin and calcium.The result should be a normal gastrin level in response to these challenges. Further, failure to respond to H2-receptor antagonist therapy should raise the index of suspicion that a polypeptidoma, rather than a gastrinoma, is responsible for clinical signs. Lastly, immunohistochemical staining of pancreatic biopsy specimen for pancreatic polypeptide will confirm the diagnosis.
Treatment
Surgical resection in a healthy patient with no evidence of metastasis should be attempted. Few data exist on survival times because of the rarity of this tumor. Individual cases where complete excision has been performed have resulted in long-term control and resolution of all clinical signs.
Exocrine Pancreatic Tumors in Cats
Background
Exocrine pancreatic carcinomas are similarly rare in the cat. No breed or sex predilection is reported, and affected cats are generally older.
Clinical Parameters
The clinical signs associated with exocrine pancreatic carcinomas in the cat are nonspecific, as in the dog; signs include anorexia, vomiting, and weight loss. Other clinical signs reported are lethargy, icterus, constipation, diarrhea, steatorrhea, pyrexia, dehydration, and a distended abdomen. In contrast to dogs, cats usually have larger and more easily palpated abdominal masses. A unique paraneoplastic alopecia has been reported in cats with pancreatic acinar carcinoma. This effect has not been recognized in dogs or humans to date and has no known etiology.
Clinical Work-up
A minimum database, chest and abdominal radiographs, and ultrasound of the abdomen should be performed to evaluate the general health status of the patient, stage for metastasis, and assess the primary mass. The results of routine blood work are usually unremarkable, although neutrophilia, anemia, hypokalemia, bilirubinemia, azotemia, hyperglycemia, and elevated liver enzyme levels have been reported. Serum lipase and amylase levels are rarely elevated.
Ultrasonography can sometimes detect a soft tissue density in the cranial abdomen, but determining whether the mass arises from the pancreas can be difficult. There may be effusion in the abdomen that can be aspirated, but this rarely provides a diagnosis because pancreatic carcinomas do not readily exfoliate into the peritoneum. This tumor can metastasize anywhere, but liver and intraabdominal nodes are commonly involved.
Treatment
Because diagnosis is usually made by exploratory laparotomy, if the patient is in good general health and there is no evidence of metastasis, an attempt at surgical resection can be considered. However, due to the highly malignant nature of this tumor (81% metastasis at the time of diagnosis), complete surgical excision is rarely achieved. Chemotherapy and radiation therapy have not been reported to be efficacious in pancreatic neoplasia.
Endocrine Pancreas Tumors in Cats
Insulinoma (Beta Cell Tumor, Islet Cell Tumor)
Background
Insulinoma is rare in the cat. It is a functional secreting tumor that arises from the islet cells in the endocrine pancreas. In addition to the secretion of insulin and its precursors, insulinomas are now known to secrete pancreatic polypeptide, somatostatin, glucagon, serotonin, gastrin, and corticotropin. Insulinomas are considered slow growing, are most commonly carcinomas, and often present late in the course of disease with signs attributable to the resultant hypoglycemia. Insulinomas occur in older cats.
Clinical Parameters
Clinical signs most commonly seen in cats are seizures, cutaneous twitching that progresses to muscle tremors, generalized ataxia, and focal tremors of the facial and appendicular musculature. These clinical signs can be explained by hyperinsulinemia with resultant hypoglycemia and release of counter-regulatory hormones (catecholamines and glucagon in the early phase and cortisol and growth hormones in the later phase of disease).Because of the patient's ability to adjust to a chronic state of hypoglycemia, signs of hypoglycemia are often not seen, even with extremely low blood glucose levels. The rate of decrease in blood glucose, as well as the duration of hypoglycemia, is considered important in the development of clinical signs.
There are two types of presenting clinical signs: neuroglycopenic (seizures, weakness, ataxia, and lethargy) and sympathetic (behavioral changes, shaking/trembling, and muscle fasciculations). The neurologic signs are due to the reliance of the central nervous system on diffusion for glucose uptake (which is predictably low in periods of hypoglycemia) and its inability to utilize other forms of energy such as fatty acids and ketone bodies. The sympathetic signs are related to an increased discharge of counter-regulatory hormones.
Clinical Work-up
Basic blood work and urinalysis, chest and abdominal radiographs, and abdominal ultrasound should be performed to diagnose and stage cats with suspected insulinomas and to rule out other causes of hypoglycemia. Blood work, urinalysis, and radiographs are usually unremarkable. Abdominal ultrasound infrequently detects a mass on the pancreas, but other organ metastases and/or mesenteric lymphadenopathy may be evident. The diagnosis of insulinoma is based on demonstration of hyperinsulinemia in the face of hypoglycemia. There are several means by which one can achieve this, including the insulin- glucose, glucose-insulin, and amended insulin- glucose ratios. For the most part these ratios are not considered diagnostic because they are associated with a high number of false-positive results. For this reason, performing a paired insulin and glucose test is considered to be the most reliable method of diagnosing an insulinoma. This test is further described in the earler section on endocrine pancreas tumors in the dog. However, it should be noted that the radioimmunoassay for insulin has not been validated in cats and so should be interpreted with caution.
One study describes the use of CgA and NSE as a marker for canine and feline pancreatic islet cell tumors and found these assays to be sensitive in detecting tumors of neuroendocrine origin. One report in the dog states that the use of fructosamine measurement may be helpful, in conjunction with insulin measurement, in diagnosing an insulinoma. Provocative testing has been described in the literature. Such tests include glucagon tolerance, glucose tolerance, tolbutamide tolerance, L-leucine, oral glucose tolerance, epinephrine tolerance, and the calcium infusion test. These tests use the administration of potentially dangerous substances and are expensive, time consuming, and most importantly not as accurate as the paired insulin-glucose tests.
The metastatic behavior of insulinoma in the cat is unknown. Of three cases, only one had histologic confirmation. This mass was solitary and well encapsulated. No metastases were detected grossly. However, this patient developed hypoglycemia 7 months later, suggestive of incomplete surgical excision and recurrence or a metastatic lesion.
Treatment
Minimal information is available for treatment of insulinoma in the cat. However, in a stable patient with no evidence of metastasis, surgical resection can be attempted.
Medical management has not been described for the management of insulinoma in the cat. For a discussion of appropriate drugs for use in the dog, see the section on endocrine pancreas tumors in the dog.
Glucagonoma
Background
Rare tumors of the pancreatic alpha cells, glucagon-secreting tumors have been described in two cats. The typical lesions that are concomitant with a glucagonoma are SND or MEN and are characteristic of glucagonoma syndrome.
Clinical Parameters and Work-up
Clinical signs described in the literature include skin lesions and blood work abnormalities. In the cat, skin lesions are characterized by erythema and crusting plaques on the limbs, abdomen, and genital areas. A complete staging scheme should include basic blood work, urinalysis, and abdominal and thoracic imaging. In one tumor evaluated with immunohistochemical stains, glucagon was not evident in the cells of the carcinoma. Biochemical parameters included normal liver enzyme levels and hyperglycemia. Diagnosis is usually made by skin biopsy, exploratory celiotomy, and histopathologic evaluation of a pancreatic mass.
Treatment
Surgical resection of a glucagon-secreting tumor should be attempted in an otherwise healthy cat with no evidence of metastatic disease; however, because there are very few reports of this tumor to date, no specific recommendations can be made.
Medical management for glucagonoma syndrome has been described in the dog. For specifics, see the section on endocrine pancreas tumors in the dog.
Gastrinoma
Background
A rare tumor of the pancreatic islets, gastrinomas secrete gastrin and result in hypertrophic gastritis and subsequent peptic ulcers. This syndrome is referred to as Zollinger-Ellison syndrome.
Clinical Parameters and Work-up
Clinical signs of gastrinomas include chronic vomiting and weight loss, which is related to the hypersecretion of gastrin and consequent ulceration. The clinical work-up should include basic blood work, urinalysis, and abdominal and thoracic imaging. Diagnosis involves the measurement of serum gastrin, demonstration of gastric hypertrophy and ulceration, and increased secretion of gastric acid. Provocative testing with secretin or calcium is usually only indicated when gastrin levels are minimally elevated. A novel method of diagnosis described is the use of somatostatinreceptor scintigraphy.
Treatment
Although the course of gastrinomas tends to be chronic, early surgical resection can be attempted. Medical management is symptomatic and includes an H2-receptor antagonist or omeprazole, and octreotide acetate. Ulcer therapy is described in detail in Chapter 5.
Pancreatic Polypeptidoma (Vasoactive Intestinal Peptidoma, Somatostatinoma)
This tumor is not reported in the cat.