History of specific gastrointestinal signs
This section focuses on the main specific gastrointestinal signs, but other, less specific signs, such as anorexia, weight loss, or polyuria /polydipsia should also not be overlooked.
Table 1.1: Steps for taking a history in patients with gastrointestinal signs2-7-8
Parameters addressed
■ Signalment
■ Chiefcomplaint
■ Present medical history (including chronology and treatments)
■ Past medical history
■ Systems review
■ Current health status (including environment and dietary history)
Table 1.2: Guidelines for history acquisition in patients with gastrointestinal signs10-11
Guidelines for history acquisition
■ always begin with the chief complaint
■ start by asking broad questions
■ ask narrow questions (questions that can be answered with few words such as “yes”, "no", or “I do not know”) to confirm previous answers
■ try to use the owner's words to avoid confusion about what the owner means
■ do not bombard the owner with questions
■ avoid combining questions
■ try to be reassuring when necessary
■ try to focus owner on the main points of the history
■ avoid categorical answers or judgments at the time of history collection
■ avoid external interruptions
1.1.2.1 Dysphagia and regurgitation
Dysphagia, which is defined as difficult or painful swallowing, can be classified as oral, pharyngeal, or esophageal. A good history can help the clinician to characterize the type of dysphagia. An owner questionnaire has been evaluated for characterization of dysphagia and was shown to be useful for exclusion of oral dysphagia and for the detection of pharyngeal dysphagia; however, it was less sensitive and specific for the assessment of esophageal dysphagia.2
Oral dysphagia is characterized by the dropping of food, leaking of water, or abnormally interrupted chewing followed by rejection of food during the meal.
Oral dysphagia is associated with disorders of the oral cavity, or with neuromuscular or osteo-articular disorders that impair normal chewing.Abnormal, repeated swallowing efforts followed by peripran- dial regurgitation of an alimentary bolus mixed with saliva are
4 Diagnostic Tools
Table 1.3: Suspected or confirmed breed predispositions for gastrointestinal diseases in dogs3-6-12
Breed Disease predisposition
Australian Cattle Dog Portosystemic vascular anomalies
Basenji Immunoproliferative lymphoplasmacytic enteritis
Bedlington Terrier Copper-associated chronic hepatitis
Belgian Shepherd Gastric carcinoma
Brachycephalic breeds Hiatal hernia, pyloric stenosis
Border Collie Selective cobalamin malabsorption
Boston Terrier Pyloric muscular stenosis, vascular ring anomalies
Bouvier des Flandres Muscular dystrophy associated dysphagia
Boxer Histiocytic ulcerative colitis, eosinophilic enteritis, lymphoplasmacytic colitis, pyloric muscular stenosis
Cairn Terrier Portosystemic vascular anomalies
Cocker Spaniel Chronic hepatitis and cirrhosis
Dalmatian Copper-associated chronic hepatitis
Doberman Pinscher Parvoviral enteritis, eosinophilic enteritis, chronic hepatitis
English Bulldog Vascular ring anomaly, constipation, fecal incontinence
German Shepherd Exocrine pancreatic insufficiency, megaesophagus, parvoviral enteritis, lymphoplasmacytic enteritis, eosinophilic enteritis,
idiopathic hepatic fibrosis, vascular ring anomaly, perianal fistula, small intestinal bacterial overgrowth
Giant Schnauzer Selective cobalamin malabsorption
Great Dane Gastric dilation volvulus
Irish Setter Megaesophagus, gastric dilation volvulus, gluten-sensitive enteropathy, vascular ring anomaly
Irish Wolfhound Portosystemic vascular anomalies (intrahepatic shunt)
Labrador Retriever Megaesophagus, portosystemic vascular anomalies, chronic hepatitis
Lhasa Apso Hypertrophic pyloric gastropathy
Maltese Hypertrophic pyloric gastropathy, portosystemic vascular anomalies
Miniature Schnauzer Pancreatitis, portosystemic vascular anomalies
Norwegian Lundehund Protein-losing enteropathy, lymphangiectasia
Pekingese Hypertrophic pyloric gastropathy
Rottweiler Parvoviral enteritis, eosinophilic enteritis
Rough Collie Exocrine pancreatic insufficiency, gastric carcinoma
Shar Pei Hepatic amyloidosis, hiatal hernia, protein-losing enteropathy, lymphoplasmacytic enteritis, eosinophilic enteritis, cobalamin
deficiency
Shi Tzu Hypertrophic pyloric gastropathy
Skye Terrier Copper-associated chronic hepatitis
Soft-coated Wheaten Terrier Protein-losing enteropathy and /or nephropathy
Standard Poodle Lobular dissecting hepatitis
West Highland White Terrier Copper-associated chronic hepatitis
Yorkshire Terrier Acute pancreatitis, portosystemic vascular anomalies, intestinal lymphangiectasia, hypertrophic pyloric gastropathy
the hallmarks of pharyngeal dysphagia.
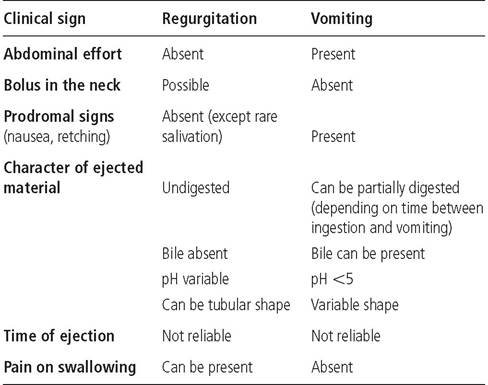
The swallowing efforts are frequently associated with coughing or choking, and also with gagging at rest.Esophageal dysphagia is associated with regurgitation, which is a passive process during which an undigested food bolus is thrown up. Sometimes, the food bolus has a cylindrical sausage shape and is covered with mucus (Figure 1.1). The time elapsed between the swallowing of the food and regurgitation of the bolus is variable but can be quite long, especially when severe esophageal dilation is present. The time period is usually shorter in patients with esophagitis, esophageal stenosis, or esophageal obstruction. In contrast to pharyngeal dysphagia, esophageal dysphagia is usually not associated with swallowing attempts.3 The history may also reveal respiratory signs such as coughing or nasal discharge, even as the primary complaint. A main task of history taking is to differentiate regurgitation from vomiting (Table 1.5).
Table 1.4: Suspected or confirmed breed predispositions for gastrointestinal diseases in cats3-6-13
Breed Disease predisposition
Abyssinian Hepaticamyloidosis
Manx Fecal incontinence, constipation
Oriental Shorthair Hepatic amyloidosis
Persian Portosystemic vascular anomalies
Siamese Megaesophagus, hepatic amyloidosis, pyloric
stenosis, intestinal tumors
1.1.2.2 Gagging
Gagging is defined as swallowing attempts without the presence of an alimentary bolus. Gagging can be a clinical manifestation of dysphagia in patients with pharyngeal disease, but it can also be associated with certain respiratory disorders of the nasal passages, larynx, trachea, or bronchi. Gagging can be associated with ptyalism or retching due to activation of the pharyngeal vomiting receptors.

Figure 1.1:
Regurgitated food. This figure shows regurgitated food from a dog with esophageal stenosis following general anesthesia for spaying.
Note the mucus surrounding a sausage-like bolus of food.1.1.2.3 Vomiting
Vomiting is not always linked to a primary gastrointestinal tract disorder. It must be differentiated from regurgitation and coughing as discussed before (Table 1.5). Vomiting is an active process with prodromal clinical signs and has three phases. The first phase, nausea, is frequently associated with hypersalivation, agitation or depression, yawning, lip licking, or repeated swallowing attempts. The second phase, retching, appears as a vomiting effort with abdominal wall contractions but without ejection of vomitus and can be associated with belching. The last phase, vomiting, is the forceful ejection of gastric contents, which is associated with very repetitive strong abdominal wall contractions.
Vomiting can be classified as acute or chronic, with chronic being defined as lasting for more than 3 weeks. Also, the content of the vomitus should be described, especially concerning the presence of food, parasites, or foreign bodies. Hematemesis is blood-tinged vomitus containing either fresh blood or digested blood, resembling coffee grounds. Hematemesis is associated with gastric or duodenal erosions and should always be considered as a sign of severe disease. However, small amounts of fresh blood are sometimes related to capillary rupture linked to the rise in venous pressure during vomition.4
Gastritis may be associated with the vomiting of bile on an empty stomach or vomiting of food usually shortly (30 minutes to a few hours) after a meal.4,5 Vomitus consisting of large volumes of fluid can be associated with ileus, small intestinal obstruction, or hypersecretory states such as gastrinoma.4
Table 1.5: Differentiation of regurgitation and vomiting3-5-6
Vomitus that smells like fecal material can sometimes be observed in patients with intestinal obstruction or chronic small intestinal bacterial overgrowth.
Vomiting associated with bile that occurs in the morning can be due to duodenal reflux gastritis in small breeds. Vomitus containing food that is produced more than 8 to 12 hours after a meal is highly suggestive of a gastric emptying disorder.3,5 Projectile vomiting can be observed in patients with a gastric outlet obstruction, but may also simply reflect violent vomiting due to any cause.6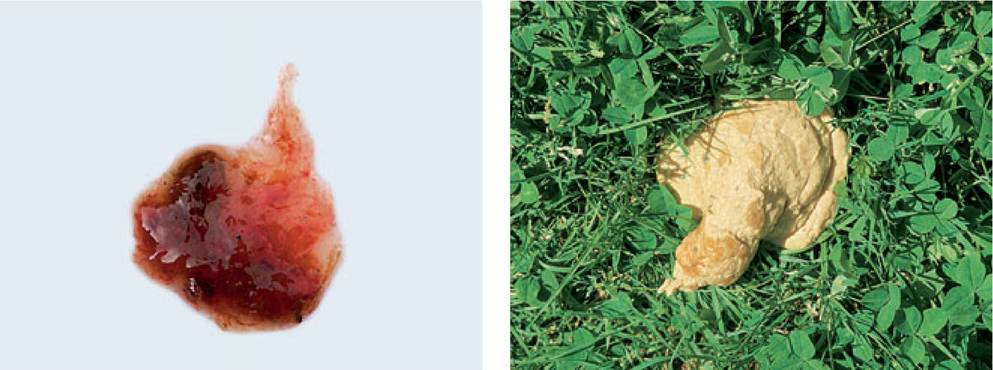
Figure 1.2:
Mucoid stool. This figure shows mucoid stools from a dog with severe colitis due to whipworm infestation. Note that the stool is almost exclusively composed of mucus and blood.
Figure 1.3:
Exocrine pancreatic insufficiency (EPI). Cow-patty yellowish stools from a dog with EPI.
Whenever possible, the number of vomiting episodes should be quantified. This is helpful to plan fluid therapy in patients with acute vomiting and also for the assessment of disease severity (canine IBD activity index; CIBDAI) in patients with chronic vomiting due to inflammatory bowel disease.7
1.1.2.2 Retching
Retching is defined by repetitive efforts to vomit without any expulsion of vomitus. Diagnostically, retching should be approached like vomiting. However, in some instances, even a good history can not differentiate retching or the regurgitation of saliva or mucus from coughing and /or expectorations. In patients that present with acute retching and abdominal distension, gastric dilation /volvulus (GDV) should be ruled out immediately.4
1.1.2.3 Diarrhea
Diarrhea is defined as the passage of feces that contain more water than normal, which increases daily fecal weight. As for vomiting, the first step is to classify whether the diarrhea is acute or chronic. The next step is to describe the fecal character by asking questions about any blood, foreign material, undigested food particles, or mucus in the feces (Figure 1.2).
The color, volume, odor, and consistency of the feces might also be helpful, narrowing the list of differential diagnoses. For example, rancid smelling, large volume, grayish brown, and cowpatty stools may suggest exocrine pancreatic insufficiency or another condition associated with maldigestion (Figure 1.3). The number of bowel movements per day should also be quantified. The main concern is to localize the origin of the diarrhea either to the small or to the large intestine. The characteristics that may be helpful for localization of the cause of diarrheal disease are shown in Table 1.6. However, these characteristics are not absolute by any means and patients with clinical signs of large bowel disease may have more significant small bowel disease. The use of photographic fecal scoring charts may be helpful for the characterization of the diarrhea (Figure 2.4).1.1.2.4 Otherstoolabnormalities
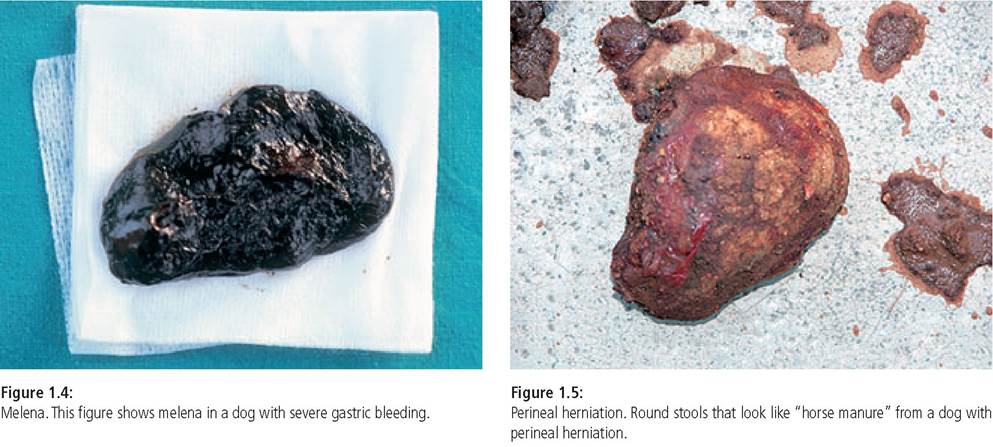
Melena is characterized by black and tarry stools (Figure 1.4) and is sometimes associated with diarrhea. Melena is a sign of the presence of blood in the GI tract. The blood usually comes from the GI tract itself, but it can be swallowed in patients that are bleeding into the respiratory tract. Melena is mostly associated with bleeding of the upper gastrointestinal tract, but the black color and tarry consistency are due to the transit of the blood through the intestinal tract.3 Therefore, blood from the upper parts of the large intestine can also be black and tarry, and blood coming from the small intestine can be fresh if the transit time does not allow for the digestion of the blood.3 Some medications, such as metronidazole, ferrous sulfate, or bismuth or some food ingredients (liver, spinach) can also produce dark stools that can sometimes be confused with melena. Asking about ulcerogenic medications, especially NSAIDs,
anticoagulant exposure (e. g., rodenticide), or recent trauma is also important.
Fresh blood that is adherent to the feces is called hematochezia and is consistent with large bowel or recto-anal bleeding. Hematochezia can be associated with local disorders (colitis, proctitis, foreign body, or neoplasia) or coagulopathy. It is not always associated with dyschezia or straining to defecate and is therefore sometimes not observed by the owner.
Ribbon-like stools are observed in conditions associated with a narrowing of the colonic, rectal, or anal passage and frequently lead to dyschezia or constipation. Sometimes, round or ball-like feces looking like horse manure (Figure 1.5) are observed with perineal herniation or anal diverticula.
Acholic feces are clay-like feces that can be observed in patients with extra-hepatic bile duct obstruction or destructive choloangiolitis.1
1.1.2.7 Flatulenceandborborygmus
Flatulence and borborygmus (rumbling of the gastrointestinal tract) are ultimately due to the presence of large amounts of intestinal gas that can occur in association with many digestive disorders. Excessive gas can also be associated with abdominal discomfort. A dietary history is important in these patients since certain types of foods commonly lead to the formation of excessive gas in the intestinal lumen (e.g., legumes, soybeans, or excess fat).
Table 1.6: Characterization of small and large bowel diarrhea3,5,6,11 Please note that none of these parameters is absolute.
| Parameter | Small intestine | Large intestine |
| Feces | ||
| Volume per defecation | Increased | Decreased or normal |
| Mucus | Absent (except in ileitis) | Frequently present |
| Melena | May be present | Rarely present |
| Hematochezia | Absent except in acute hemorrhagic diarrhea | Frequently present |
| Steatorrhea | Present in patients with maldigestion or malabsorption | Absent |
| Defecation | ||
| Frequency | Usually slightly increased up to 4 times per day but can be severely increased in severe acute enteritis | Increased (many defecations with small volume) |
| Dyschezia | Absent | Present |
| Tenesmus | Absent | Frequently present |
| Urgency | Absent; except in severe cases | Usually present; sometimes with indoor soiling |
| Other signs | ||
| Flatulence / borborygmus | May be present | May be present |
| Weight loss | May be present | Rare |
| Anal pruritus | Absent | May be present |
| Vomiting | May be present | May be present in acute colitis |
1.1.2.5 Dyschezia
Dyschezia is defined as difficult or painful defecation characterized by straining to defecate with or without defecation. Dyschezia can be observed in association with large bowel diarrhea but also with some other conditions such as constipation, rectal disease, anal disorders such as anal furunculosis or anal gland sacculitis, or prostatomegaly in male dogs.
Tenesmus is straining to defecate and is a clinical manifestation of either dyschezia or colonic and recto-anal discomfort.
1.1.2.6 Constipation
Constipation is defined by the passage of dry, hard feces and is associated with a decreased number of bowel movements and straining to defecate. In cases of suspected constipation, it is important to ask about urination behavior as urinary straining can be confused with straining to defecate in some patients, especially in cats with lower urinary tract obstruction. Straining before defecation is usually associated with obstructive or functional disorders inducing constipation. In contrast, straining throughout defecation or persisting after defection has been completed is frequently associated with diarrhea of inflammatory disorders of the colon and /or rectum.3
Sometimes, the constipated patient is presented for diarrhea. The diarrhea perceived by the owner is due to a small quantity of liquid fecal material passing around the fecal bolus lodged in the colon and /or rectum.
1.1.2.7 Fecalincontinence
Fecal incontinence is characterized by uncontrolled loss of feces without crouching to defecate. It must be differentiated from urgency to defecate by carefully questioning the owner as these two causes of fecal soiling are frequently confused. In patients with true fecal incontinence, the stools are usually normal and loss of feces frequently occurs during excitation or coughing. The owner should be questioned about the presence of controlled and normal defecation to assess whether the neuro-muscular control of defecation is functional. A history of trauma (especially tail trauma in cats) as well as medical or surgical conditions of the perianal area are frequently associated with fecal incontinence.
1.1.2.8 Anal pruritus
Anal pruritus is manifested by perineal licking or biting, anal scratching, or scooting. It is usually associated with recto-anal diseases such as anal furunculosis, anal gland disorders, or Dipylidium infestation, but can also be a manifestation of food allergy, constipation, or inflammatory bowel disease.
1.1.2.9 Abdominal pain
The owner may report certain behaviors such as a saw horse stance or prayer position (stretching out the forelimbs with the sternum in contact with the floor and standing on the hindlimbs), which are strongly suggestive of cranial abdominal pain.4 Bruxism (teeth grinding) or restlessness can also sometimes be associated with severe abdominal pain in dogs and cats. Restlessness can sometimes be observed during the first stages of gastric dilation/volvulus.8 In cases of extreme abdominal pain, the pet may be severely depressed or even aggressive.
1.1.3