INFLAMMATORY BOWEL DISEASE
Historical Perspectives
IBD is now well recognized as one of the most common causes of chronic vomiting and diarrhea in cats and dogs. Our knowledge about the various manifestations of this syndrome has expanded greatly over the last 20 years.
Before the mid-1980s there was very little information in the veterinary literature about inflammatory bowel disorders. Early reports included an overview of clinical observations of malabsorption in the cat (1969) and a single case report on a cat with what was described at that time as ulcerative colitis (1972). Textbooks on small animal medicine published in the 1970s included only short and vague discussions about malassimilation syndromes (primarily lymphangiectasia, lymphosarcoma, and exocrine pancreatic insufficiency), and most of this information pertained only to dogs. Several of the earliest reports on IBD in dogs, centering on histiocytic ulcerative colitis in boxers, appeared in human journals in 1967 and 1970. Our recognition that IBD is a truly common disorder in cats and dogs did not really occur until the 1980s.In humans a type of IBD known as ulcerative colitis was described as early as 1859 in England. It was not until 1932, however, that small intestinal inflammatory disease, specifically ileitis, was defined as a separate entity. It is now apparent in humans that the prevalence of inflammatory bowel disorders has increased dramatically over the past several decades, such that thousands of Americans and hundreds of thousands of patients worldwide are affected. Currently in the human field there are entire textbooks devoted to IBD, some encyclopedic in extent and containing tremendous diversification of viewpoints by their many authors.
To what factors do we owe our rather dramatic increase in awareness of the clinical manifestations of this syndrome in cats and dogs over the past 20 years? Is IBD a relatively new disease, or rather have we as clinicians simply become more skilled at recognizing it? I believe that the latter is much more likely.
Our recognition that IBD commonly occurs directly parallels our increased use of endoscopy to investigate more thoroughly patients with such clinical signs as vomiting, diarrhea, weight loss, and change in appetite. In the not too distant past, the diagnostic work-up of a patient with chronic vomiting and/or diarrhea was commonly limited to such tests as fecal examination for parasites, fecal cultures, hematologic studies, and survey and contrast radiography, or in some cases simply fecal tests and a series of empiric pharmaceutical maneuvers. Now, however, an understanding of the absolute importance of histologic evaluation of GI tissues in patients whose symptoms are not readily explained by routine tests and dietary trials is thankfully well entrenched in our thinking. Indeed, IBD is a diagnosis that can be made only by biopsy specimen analysis. I suspect that in the past many patients with what was described as “nonspecific enteritis” may actually have had some type of IBD.Without specific treatment, many patients with chronic vomiting and/or diarrhea with subsequent wasting disease were euthanized or died prematurely as a result of “unknown causes.”My personal experience parallels that of other veterinary gastroenterologists working in the early 1980s.Beginning in 1980 as pediatric-sized endoscopes became more readily available and as we gained the necessary skills to routinely guide an endoscope through the pylorus and into the duodenum of cats and dogs, we rapidly became more capable of obtaining GI tissue samples both more safely (endoscopy is less invasive than exploratory surgery, with procurement of full-thickness biopsy specimens) and more readily (owners are much more likely to allow endoscopy than they are to approve a laparotomy). Once it became apparent that significant inflammatory bowel changes were present in a number of patients with GI symptoms (especially vomiting and/or diarrhea), it followed that procurement of gastric and intestinal biopsy samples should be strongly recommended in any patient with chronic (lasting as little as 4 weeks) unexplained signs.
Indeed, the more we looked, the more we found.On a personal note, I have had the good fortune to have worked at two large high-caseload institutions (Angell Memorial Animal Hospital in Boston and the VCA West Los Angeles Animal Hospital) in urban areas where a majority of animal owners tend to demonstrate a strong desire to provide the best medical care that they can for their pets. Many of our owners have embraced the idea of reaching a definitive diagnosis as early as possible. With the availability of endoscopy, we have been able to recommend and perform GI biopsies much earlier on the “chronicity curve” of disease. Our patients and their owners have no doubt benefited greatly from this approach. As a result of these experiences, I have had the opportunity to study the various clinical manifestations of IBD in quite a large number of cats and dogs. The information that follows represents a compilation of my experiences as a clinician along with observations of other specialists in gastroenterology who have also managed a significant number of cases.
We are in the midst of an exciting era of research in the field of the various inflammatory bowel disorders. It must be realized, however, that despite our ever-increasing knowledge in this area in both the human and the veterinary fields, we are still at the frontier. We have much to learn!
Terminology and Pathogenesis
The term inflammatory bowel disease describes a group of chronic intestinal disorders that are characterized by a diffuse infiltration within the lamina propria by various populations of inflammatory cells, including lymphocytes, plasma cells, eosinophils, neutrophils, and macrophages. The most commonly identified idiopathic inflammatory bowel disorders in cats are lymphocytic- plasmacytic enteritis, benign lymphocytic enteritis (an apparently distinct disorder from intestinal lymphosarcoma), and lymphocytic-plasmacytic colitis. Two different classifications of eosinophilic IBD have been identified in cats: eosinophilic enteritis and hypereosinophilic syndrome.
Eosinophilic enteritis is characterized by diffuse or focal infiltration of inflammatory cells that are almost entirely eosinophils into one or more layers of the alimentary tract. The stomach, small intestine, and colon may all be involved in some cases (eosinophilic gastroenterocolitis). Eosinophilic enteritis in cats is similar in clinical manifestations and response to treatment (very favorable) to the same condition in dogs.
Hypereosinophilic syndrome is a severe type of IBD in cats that involves massive infiltration of eosinophils in the alimentary tract and other parts of the body. Dramatic bowel thickening often results.
The eosinophilic disorders are not seen very commonly in cats. Of the two, hypereosinophilic syndrome is less common and more life threatening. Occasionally, mixed populations of inflammatory cells (e.g., lymphocytic-plasmacytic-eosinophilic, lymphocytic-eosinophilic) are identified. Inflammatory disease may be localized to the small intestine (enteritis), specific areas of the small intestine (e.g., duodenitis, ileitis), or colon (colitis).Although some cats have generalized intestinal involvement (enterocolitis), many cats with IBD have only small intestinal disease.
In dogs the most common types of IBD are lymphocytic-plasmacytic enteritis and lymphocytic-plasmacytic colitis. Pure lymphocytic enteritis is rarely identified in dogs. Eosinophilic enteritis is occasionally seen, but definitely not as commonly as was once speculated.
It is essential that the clinician understand that identifying an increase in inflammatory cells on intestinal biopsy specimen analysis does not automatically warrant a diagnosis of IBD. Inflammatory cells may be present in increased numbers simply as a normal response to a variety of inciting factors. Potential underlying causes include hyperthyroidism (thyrotoxicosis may generate an inflammatory response); various infectious agents, including bacteria, viruses, and parasites (including Giardia); food antigens; presence of a foreign body; and GI neoplasia, which may be associated with a blanket of inflammatory cells surrounding neoplastic cells (e.g., this may occur with lymphosarcoma).
It is my impression that tissue samples that are characterized by moderate to severe inflammation represent true idiopathic disease in a majority of cases. Specimens that reveal only mild inflammation, however, could be consistent with either mild idiopathic IBD or any number of underlying disorders. It is the clinician’s responsibility to investigate thoroughly (see section on diagnosis) for underlying causes, whenever possible, before settling on a final diagnosis of idiopathic IBD. By taking this approach, we will most certainly better serve both our patients (by definitively diagnosing and specifically treating any underlying disorders) and our combined efforts in more accurately defining the diverse group of inflammatory bowel disorders. The term IBD is used here to describe a chronic disorder in which no specific cause can be determined.
The definitive cause of IBD, despite years of major research in humans and some recent work in animals, remains unknown. It is likely that a cytopathic immunologic response results in the bowel from chronic antigenic challenge. It appears that immune activation in IBD is largely confined to the GI tract, so the search for the “antigenic trigger” has focused on the intestinal lumen. Although the specific inciting factor or factors for these host hypersensitivity responses are still unclear, the most commonly speculated causes include defective mucosal immune responses, changes in mucosal permeability, dietary influences, and intestinal microorganisms.
Recently research in human medicine has focused on a possible autoimmune response in the pathogenesis of IBD. It has been proposed that there may be a specific immune response against an antigen expressed on the patient’s own cells, particularly on intestinal epithelial cells. In this theory the patient mounts an appropriate immune response against some luminal antigen (e.g., dietary or microbial). However, because of similarities between proteins on the epithelial cells and the luminal antigens, the patient’s immune system also attacks the epithelial cells.
The immune response may be directed specifically at the epithelial cell. A defect in immunoregulation may be involved in this process (i.e., in individuals with IBD there may be a failure to suppress the inflammatory response). Thus, as a result of failure of normal suppressor mechanisms, there may be a prolonged and vigorous response to some normal luminal antigens.Although theories abound, there is still no defined cause for IBD. Active research in both the human and the animal fields for pathogenic mechanisms continues.
Patient Profile
Although IBD most commonly occurs in middleage to older cats and dogs, it has occasionally been diagnosed in patients as young as 4 months. The predominant clinical sign in young cats with IBD tends to be diarrhea, whereas in young dogs I have found vomiting to be the more predominant sign. Attempts to perform intestinal biopsies on young patients are made only after meticulous effort is taken to rule out intestinal parasites (including Giardia and Cryptosporidium), infectious agents (including viruses and bacteria, including Campylobacter, Salmonella, and Shigella), adverse food reactions, and metabolic derangements. No breed or sex predilections have been identified in animals with IBD.
History and Clinical Signs
One of the most common clinical signs observed in patients with idiopathic small intestinal IBD is vomiting. Vomiting is a common presenting complaint seen in clinical practice, and clinicians should give careful attention to patterns observed by the owner. In inflammatory bowel disorders, vomiting is most often recognized as an intermittent occurrence for weeks, months, or years. Often as the disorder progresses, there is an increased frequency of vomiting and other clinical signs, which leads the owner to seek veterinary attention. Alternatively, an occasional patient with even moderate to severe inflammatory changes on biopsy specimen analysis may be presented with clinical signs limited to an acute onset of vomiting and lethargy, with no past history of GI signs.
Vomiting episodes are usually associated with retching, are nonprojectile, and may produce clear fluid, bile, or foam. Vomiting of food, either fresh or partially digested, is sometimes observed. In patients with concurrent gastric hypomotility that is either idiopathic or secondary to chronic gastritis or IBD, vomiting of undigested food may occur many hours after eating. Blood is rarely present. Hematemesis may indicate concurrent gastric involvement (e.g., erosions, foreign body, gastritis, neoplasia) or superficial erosive changes in the proximal small intestine.
Vomiting in IBD can occur at variable times after eating. Many patients with mild IBD go about their daily routine showing no untoward effects from any of the vomiting episodes. The vomiting and associated nonspecific signs may be cyclical in nature. Clinical signs may be evident on one or several days and then spontaneously disappear, indicating that untreated IBD runs a course often characterized by exacerbations and remissions. Successes therefore should not automatically be attributed to the symptomatic treatment that is often given in these cases (nothing by mouth, bland diets, antiemetics). It is owing to this cyclic nature that some patients with IBD are not presented until signs are more frequent or severe. If a pattern of intermittent vomiting in a cat causes owner concern, a work-up to determine its cause should be undertaken, even if it is not a longstanding clinical sign.Without question, IBD is one of the leading differentials of chronic vomiting in cats and dogs.
In my experience the second most common sign observed in feline IBD is diarrhea. It may be the most common sign in dogs. Diarrhea may be the sole clinical sign or may occur in conjunction with intermittent vomiting. Diarrhea may be acute or chronic, but most cases are evaluated because of chronic diarrhea that is responsive or only temporarily responsive to diet changes or nonspecific symptomatic treatment. The first step in diagnosis of a disorder characterized by diarrhea is to decide whether the process is principally affecting small or large intestine or both. This helps determine the direction of further work-up and is done by combining information from history, physical examination, and stool characteristics (frequency, volume, consistency, odor, color, composition).
Small bowel diarrhea is most often characterized by large quantities of soft-formed, bulky, or watery stool. Steatorrhea may be evident, and more chronic cases are often accompanied by weight loss and listlessness. In contrast, diarrhea of large bowel origin most often has a loose, stringy consistency due to increased mucus content, and intermittent streaks of fresh blood may be present. Owners are often not aware of the presence of blood. Other signs include increased frequency of attempts to defecate (cat owners may misinterpret this as attempts to urinate), defecating in abnormal places, and hiding (cats). Cats with large intestinal inflammation sometimes begin defecating outside the litter box. Dogs sometimes demonstrate a sense of urgency to defecate.
If the disease is limited to the large intestine, most patients remain active and alert, have a normal appetite, and do not lose weight. Some patients have both small and large intestinal disease, with similar histologic changes, yet only small intestine or large intestine signs predominate. If biopsy specimens are to be obtained in chronic diarrhea cases, obtaining tissue samples from both small and large intestine is strongly recommended. Treatment for only small or large intestinal disease is not likely to result in complete resolution of signs if generalized involvement is present.
In some cats with chronic IBD, diarrhea does not occur until some stressful episode (e.g., change in environment, queening) causes an exacerbation of clinical signs. In these cases of acute diarrhea, initial testing is naturally directed toward ruling out dietary indiscretions, parasites, foreign bodies, and infectious agents (e.g., Campylobacter). Often no definitive diagnosis can be made, and feeding trials and empirical treatment fail to effect lasting resolution of the diarrhea. Further work-up involving intestinal biopsy in these cases may reveal chronic moderate to severe inflammatory bowel changes. A review of the history again may surprisingly not show any past occurrence of vomiting or diarrhea. Diarrhea, once apparent, usually does not resolve until specific treatment for IBD is instituted in these cases.
In addition to vomiting and diarrhea, other clinical signs that may be observed in IBD include changes in attitude or activity, altered appetite, and weight loss. Many patients tend to be more depressed during periods of increased vomiting. As with the sign of vomiting, these activity-level changes are often cyclic. In some cats with chronic diarrhea, listless behavior is the predominant attitude. An owner may describe decreased tendencies to play, decreased interest in surroundings, and more frequent hiding or sitting near heating units for long periods of time.
Appetite changes in cats with IBD vary from decreased to complete anorexia to ravenousness. Inappetence seems to occur more commonly in cats that have vomiting as the primary clinical sign and usually occurs during exacerbations of clinical signs. In some cats, anorexia is the primary clinical sign and vomiting or diarrhea is not observed until later or not at all. The three leading differential diagnoses for a cat with a ravenous appetite, diarrhea, and weight loss are IBD, hyperthyroidism, and exocrine pancreatic insufficiency (an uncommon disorder in cats). I have also seen cats with chronic low-grade lymphocytic lymphoma of the small intestine exhibit identical clinical signs (Box 7-2). Dogs with IBD tend to have a normal to decreased appetite, depending on the degree of disease that is present. One notable exception is that Chinese shar-peis with IBD frequently have an increased to ravenous appetite (see further information about shar-peis later in this chapter).
The clinical course of IBD in many dogs and cats, at least fairly early in the course, is characterized by unpredictable exacerbations and remissions. This makes accurate assessment of disease burden difficult. It is important that an early assessment be made for patients that demonstrate GI symptoms so that the best course of therapy can be
| BOX 7-2 | Differential Diagnosis of Disorders Causing Chronic Diarrhea, Weight Loss, and Ravenous Appetite in Cats |
| Hyperthyroidism Inflammatory bowel disease Intestinal lymphoma Exocrine pancreatic insufficiency | |
instituted early rather than later, when more intensive therapy might be needed.
Diagnosis
The differential diagnosis for IBD is listed in Box 7-3.A definitive diagnosis of IBD can only be made based on intestinal biopsy specimen analysis. Other tests are run to evaluate the overall health status of the patient and to rule out other disorders. Recommended baseline tests include a complete blood count, complete biochemical profile, urinalysis, and fecal examinations for parasites and in cats a serum thyroxine (T4) test and tests for feline leukemia virus antigen and feline immunodeficiency virus antibody.
Baseline test results frequently are normal or negative, but abnormalities that may be identified include mild nonregenerative anemia (anemia of chronic inflammatory disease); leukocytosis (20,000 to 50,000 cells∕μl) without a left shift (suggests active chronic inflammatory disease); eosinophilia (mild to dramatic increase) in some cats and dogs with eosinophilic enteritis and in all cats with hypereosinophilic syndrome; and hypoproteinemia (increased loss of protein through a damaged intestinal lining) or mild hyperproteinemia (due to increased globulin fraction in idiopathic
BOX 7-3
Differential Diagnosis of Disorders Resembling Inflammatory Bowel Disease in Dogs and Cats
Chronic giardiasis
Hyperthyroidism (cats)
Dietary sensitivity (e.g., food allergy or intolerance) Bacterial overgrowth
Clostridium perfringens enterotoxicosis Lymphangiectasia (dogs)
Lymphoma
Pythiosis
Functional bowel disorder (e.g., irritable bowel syndrome)
Histoplasmosis
Exocrine pancreatic insufficiency
Feline infectious peritonitis (gastrointestinal involvement)
Adenocarcinoma
Stagnant loop (secondary intestinal obstruction)
(e.g., adenocarcinoma, mesenteric adhesions) IBD or feline infectious peritonitis with intestinal involvement).
Hypoproteinemia (total protein less than 6.0 g/dl, with albumin and globulin fractions proportionately decreased) occurs much less commonly in cats with IBD than in dogs and usually indicates moderate to severe intestinal involvement when it is identified in a cat with IBD. A work-up should be expedited to determine the cause. The most common cause of hypoproteinemia in cats with a total protein level less than 5.0 g/dl in my case series is intestinal lymphoma. The most common cause of PLE in dogs is lymphocytic-plasmacytic enteritis.
Fecal α.-protease inhibitor (FθpPI) is an assay that will help detect evidence of excessive intestinal protein loss in dogs before hypoproteinemia develops. O1-PI is a plasma glycoprotein. It is not present in the intestinal lumen above trace background concentrations unless there is abnormal transmucosal loss of plasma, lymph, or intracellular fluid as a result of GI disease. FapPI can reach abnormal concentrations before there is enough protein loss from the intestine to cause panhypoproteinemia. OpPI is excreted in the stool with minimal loss of its immunoreactivity, because it is largely resistant to degradation in the intestinal lumen by virtue of its inhibitory activity.
This assay is useful in dogs with chronic diarrhea that have normal or slightly decreased serum protein levels, as a screening tool for evidence of the presence of a potentially severe PLE disorder. The assay is available at the GI laboratory at Texas A&M University.[‡‡‡‡] Contact the laboratory for special fecal sample submission tubes. Samples are submitted frozen. The level of FOpPI in healthy dogs has been determined to be no more than 5.7 μg∕g.Values as high as 53.2 μg∕g have been observed in dogs with PLE sufficiently severe to cause panhypoproteinemia. Values in the range of 6.0 to 15.0 μg∕g have been observed in dogs with PLE not sufficiently severe to cause panhypoproteinemia.
Hyperthyroidism should always be ruled out in any cat older than 5 years of age that has manifest unexplained GI signs. Hyperthyroidism is occasionally diagnosed in cats younger than 5 years of age, so this possibility should always be considered. Testing for hyperthyroidism may include running a free T4 by equilibrium dialysis or a thyroid hormone (T3) suppression test in cats with clinical signs suggestive of hyperthyroidism but that have a baseline T4 level in the high normal range. Interestingly, thyrotoxicosis can cause inflammatory changes in the intestinal tract, and this may explain why some cats with hyperthyroidism have vomiting or diarrhea. These changes often resolve after treatment for hyperthyroidism is instituted. Failure of vomiting or diarrhea to resolve, however, within 4 to 6 weeks of institution of treatment for hyperthyroidism suggests the possibility of ongoing inflammatory disease or some other disorder that likely requires primary therapy.
I have observed cats with moderate to severe lymphocytic-plasmacytic enteritis or lymphocytic enteritis that were also hyperthyroid. Intestinal biopsy specimens were obtained from these patients after treatment for hyperthyroidism effectively decreased serum thyroid hormone concentrations into the normal range but had little effect in resolving ongoing GI symptoms (generally primarily vomiting and/or diarrhea, although in several cats the predominant sign was inappetence). It has been my impression that cats with such significant degrees of inflammation have both hyperthyroidism and idiopathic IBD rather than a single problem.
It is also recommended that all dogs and cats exhibiting chronic signs of GI disease have the serum cobalamin concentration measured. Several studies have demonstrated that some patients with GI disease have a significant deficiency of tissuelevel cobalamin. This is particularly important in any case in which there has already been a subop- timal response to previous therapy, because supplementation with cobalamin may be helpful to such patients. Clinical signs of cobalamin deficiency include chronic wasting or failure to thrive, lethargy, and diarrhea. Subnormal cobalamin levels may result from intestinal mucosal disease, reduced intrinsic factor availability, or bacterial competition. Cobalamin therapy in patients with subnormal levels may be an important key to improved weight gain and a decrease in signs such as vomiting and diarrhea. Dose recommendations are described in the treatment section for IBD.
Patients with chronic diarrhea should also be thoroughly evaluated for intestinal parasites, including Giardia and Cryptosporidium, and Clostridium perfringens enterotoxicosis (CPE). A panel of fecal tests is run, including zinc sulfate centrifugal
222 chapter 7 I Chronic Diseases of the Small Intestine
flotation, Giardia antigen test, C. perfringens enterotoxin assay, and Cryptosporidium indirect fluorescent antibody test. Dogs and cats with IBD may have multiple GI disorders concurrently, and it is important that each problem be identified so that the most comprehensive treatment regimen can be instituted. Dogs should also be tested for intestinal bacterial overgrowth (described later in this chapter).
Survey abdominal radiographs and barium contrast study results are often unremarkable. Because cost containment is so often an important factor in clinical practice, barium series are often not performed unless clinical signs or abdominal palpation findings (e.g., obstruction) indicate that this procedure should be done. In many cases, money is best spent on baseline tests and intestinal biopsies. Abnormal findings that may be identified on a barium series include diffuse mucosal irregularities or spicular small intestinal mucosal changes and thickened bowel segments. Positive findings do not provide a definitive diagnosis; rather, they confirm the need for direct examination and biopsy of the affected areas. Radiographs can also suggest false-positive findings.
Intestinal biopsies can be performed either under endoscopic control or by exploratory laparotomy. Among the many advantages of endoscopy are that it is relatively quick and noninvasive. Multiple biopsy samples can be obtained, and the stomach, proximal small intestine (and frequently the proximal jejunum in cats), and colon can be thoroughly evaluated. In many cats, ileum samples can be obtained blindly, with the endoscope tip situated in the ascending colon or at the junction of the transverse and ascending colon. In most dogs larger than 8 to 10 lb, a pediatric-sized endoscope can be advanced into the ileum. A total of 8 to 10 small bowel biopsy specimens are usually obtained at endoscopy, depending on the gross appearance of the mucosa. Biopsies of proximal small intestine, as well as stomach, should always be done in patients with chronic vomiting that are undergoing endoscopy. It is not uncommon for cats and dogs with inflammatory changes involving only the small intestine to be presented with signs limited to chronic intermittent vomiting. If only gastric biopsy samples are obtained, the diagnosis may be missed.
The gross appearance of the mucosa in IBD can range from normal (primarily cream to slightly pink in color) to mildly erythemic to varying degrees of mucosal irregularity (Figure 7-1). Mucosal irregularity may appear as fissures or resemble a cobblestone texture in more advanced cases (Figure 7-2). Focal erosions may also be observed. The mucosa may be friable and may bleed from direct contact with the endoscope tip as it is advanced. Endoscopic biopsy techniques useful in the small intestine have been described in detail elsewhere. Biopsy samples vary in size. They are often small when the intestinal mucosa is
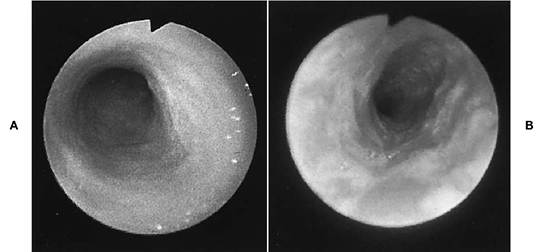
Figure 7-1 A, Endoscopic photograph of normal duodenal mucosa in a dog. Normal small intestinal mucosa is primarily cream to slightly pink in cats and pinkish white to light red in dogs.The mucosa often appears slightly irregular or velvety as a result of its makeup of digitate villi. B, Mild mucosal irregularity, increased graininess, and patchy erosive mucosal changes in a dog with moderate lymphocytic-plasmacytic enteritis. There was a history of chronic intermittent vomiting that had recently become more frequent.

Figure 7-2 Severe mucosal irregularity (note sizable troughs) in a 9-month-old cat with a ravenous appetite, voluminous loose stools, and weight loss. Endoscopy was done after there was no response to empirical treatment for exocrine pancreatic insufficiency and occult gastrointestinal parasitism. The histologic diagnosis was severe lymphocytic- plasmacytic enteritis.
normal. When the intestinal mucosa is compromised by some disorder, sample size is invariably larger. Occasionally a long linear strip (2 to 3 cm) of tissue is lifted off when marked inflammatory disease causes altered mucosal and submucosal integrity. A greater than normal amount of hemorrhage may occur at the site after mucosal samples are obtained. This is rarely of any concern. The risk of gastric or intestinal perforation by endoscopic biopsy forceps is extremely low and would only be expected to occur if tissue samples are obtained from the depths of ulcerated areas.
The abdomen should be carefully palpated before endoscopy when the patient is under general anesthesia to examine for abnormalities that may have been missed during palpation when it was awake. A disadvantage of endoscopy is that extraluminal lesions cannot be evaluated. This is not a significant problem, however, if the decision to perform endoscopy rather than exploratory laparotomy is based on careful patient evaluation, including baseline testing and abdominal palpation. In addition, ultrasound can be used to examine for intestinal masses and to evaluate wall thickness.
If it appears that an intestinal mass is present, greater consideration is given to doing an exploratory laparotomy. If exploratory laparotomy is performed, a total of three full-thickness biopsy samples are obtained (one each from the duode- num,jejunum, and ileum). At laparotomy, a majority of patients with IBD have grossly normal bowel. If clinical signs warrant abdominal exploratory, intestinal biopsy specimens must be obtained regardless of the gross appearance of the intestines. A lymph node biopsy should also be done if there is any lymphadenopathy. Biopsy samples of other tissues (e.g., liver, pancreas, kidney) are obtained if indicated based on abnormal laboratory test results or abnormal gross appearance.
The reason for obtaining multiple biopsy samples from the small bowel is that intestinal diseases may have varying degrees of severity in different parts of the intestinal tract. There may also be segmental lesions with some normal areas still present. It is even possible to find patchy normal zones of intestine in a patient with a life-threatening intestinal disease. Therefore there is no guarantee that representative tissue samples will be obtained from a patient that in fact does have intestinal lesions, especially when there are no grossly evident lesions to guide the clinician to a site that is more likely to yield significant information. By obtaining multiple samples and using techniques best suited for procuring high-quality samples, diagnostic yield will be enhanced.
Interpretation of Pathologic Findings
In inflammatory bowel disorders, increased numbers of inflammatory cells are present in the lamina propria. Infiltrations of either single-cell or mixed-cell type may be involved. Often one to two cell types predominate (e.g., lymphocytic- plasmacytic enteritis, lymphocytic enteritis). Neutrophils are not commonly identified in IBD but, when present, probably indicate an inflammatory response to a microbial component of the disorder. Histologic changes are usually reported as mild, moderate, moderate to severe, or severe, and the percentages of various inflammatory cells are noted. Other abnormalities that may be observed include mucosal atrophy, villous atrophy without cryptal hyperplasia, villous fusion, epithelial erosion, and fibrosis.
In general, “mild” IBD refers to increased inflammatory cells without architectural disruption, glandular necrosis, or fibrosis in the lamina propria. “Moderate” IBD refers to increased numbers of inflammatory cells with attendant separation and distortion of glands or crypts. There may also be mild villous blunting.“Severe” IBD is manifest by architectural distortion of the mucosa, marked villous blunting, marked separation of glands or crypts, necrosis, and fibrosis. Studies are ongoing to further define the criteria for various degrees of IBD.
Severe cases of lymphocytic-plasmacytic enteritis or lymphocytic enteritis can be difficult to differentiate histologically from lymphoma, especially in cats, when endoscopic-sized biopsy samples are evaluated. There are serious implications as to what type of therapy to prescribe in such cases. Changes that tend to suggest lymphoma include absolute uniformity of the lymphocyte population, mitotic cells, pleomorphism, and attendant ablation of villous arches. Areas of necrosis may be present. Overlying mixed inflammatory cell infiltrates may make it difficult to differentiate benign from malignant disease. If a diagnosis is unclear from evaluation of endoscopic biopsy samples, it may be necessary to repeat the procedure to obtain more samples (generally 2 to 4 weeks later) or to obtain full-thickness intestinal samples at laparotomy. Use of immunohistochemical staining techniques may also be helpful. Histologic differentiation of IBD and lymphoma is summarized in Table 7-1.
A major, and probably underappreciated, problem related to interpretation of pathologic findings by clinicians is the lack of uniformity with which pathologists assess intestinal biopsy specimens. Variability in the histologic assessment of the general group of inflammatory bowel disorders has raised many questions about the significance of certain findings. Part of the basis for the confusion is that little information is available regarding normal cellularity of the lamina propria or normal villus length in dogs and cats of different breeds and ages, that eat different diets, that live under different conditions, and so on. This then makes it difficult to clearly define and describe various degrees of normal and abnormal intestinal histologic findings. One pathologist’s interpretation may be quite different from that of another. The difficulty becomes somewhat greater when inadequate endoscopic samples (too small or damaged) are submitted or when a pathologist is inexperienced or disinterested in evaluating other than fullthickness intestinal samples. It is therefore recommended that clinicians select their pathologists carefully and that consistent efforts be made to obtain the best-quality tissue samples. There are veterinary pathologists who specialize in GI tissue pathology, just as there are specialists in dermatologic pathology. Most pathologists are eager to discuss cases with clinicians, and indeed this opportunity to compare observations is an invaluable means of making the best use of the available information for determining a patient’s treatment and prognosis. In some situations it may be best to obtain a second or third opinion before deciding on a final diagnosis.
In recent years investigators have begun some very important work centered on developing specific criteria for histologic grading of various inflammatory bowel disorders in small animals. In one study it was shown that there can be
| UABLEUitf Features of Lymphocytic-Plasmacytic Enteritis/Colitis | ||
| and Intestinal Lymphosarcoma | ||
| Lymphocytic-Plasmacytic | Intestinal | |
| Enteritis/Colitis | Lymphosarcoma | |
| Gross features | ||
| Thickened bowel wall | ± | ± |
| Involvement of other organs | - | ± |
| Histologic features | ||
| Cell population | Heterogeneous | Homogeneous |
| Lamina propria infiltration | + | ± |
| Submucosal infiltration | ± | ± |
| Muscularis infiltration | — | ± |
| Serosal infiltration | - | ± |
| Involvement of other organs | - | ± |
From Roth L: Pathologic atlas of selected gastrointestinal disorders. In August JR, ed: Consultations in feline internal medicine, Philadelphia,1991,WB Saunders.
±, May be present; —, absent; +, present.
substantial interobserver variation among pathologists when evaluating the same intestinal histologic sections. Biopsy specimen interpretation can be notoriously subjective from one pathologist to the next. Most clinicians are well aware of the importance of obtaining intestinal biopsy specimens from patients with signs that may be consistent with intestinal disease. As we go forward we need to focus more on two important areas, namely, we need more consistency among pathologists regarding how different pathologists interpret the same tissue specimens, and there is a need for some correlation between the pathologist’s description of the tissue and the clinical state of the patient.
We need to know whether or not a clinically significant disorder exists in a particular tissue, because in some instances a pathologist may interpret a sample as being abnormal, suggesting the presence of intestinal disease, and yet the patient may be known to have no signs that correlate with these findings.
Variation in the interpretation of intestinal biopsy specimens among pathologists has also been described in human medicine, in which there are also sometimes blatant differences in diagnostic criteria. It is certainly acknowledged that histologic evaluation of the digestive tract is difficult. Continued collaboration between clinicians and pathologists is essential if we hope to develop a more accurate and predictable set of criteria for consistent interpretation of intestinal biopsy samples.
Treatment
It is important that the clinician formulate a treatment protocol based on a correlation of clinical course, laboratory and gross findings, and histologic findings rather than relying on histologic changes alone. Although treatment principles for cats and dogs with IBD are similar, drug selection and dosage regimens vary between these two species in some situations. For the sake of clarity, treatment recommendations for cats and dogs are discussed separately.
Cats
Dietary Therapy
Because dietary allergens may play a role in the cause of IBD, specific dietary therapy may be beneficial. Dietary therapy is instituted at the outset for all cats with IBD, and in cats with mild IBD, dietary therapy alone may be sufficient for resolution of clinical signs. In one study, which evaluated 55 cats with various GI symptoms, of which vomiting and diarrhea were the most common signs, 16 cats (29%) were classified as food sensitive based on response to feeding of a novel protein source (either chicken or lamb in this particular study). Resolution of GI signs occurred fairly quickly in these cats, and then signs recurred once the original diet was reintroduced. All of the cats with food sensitivity had inflammation, identified on endoscopic biopsy specimens, in at least one region of their intestinal tract. Gastric mucosal biopsy specimens were abnormal in 66% of the food-sensitive cats, and duodenal samples were abnormal in 50%. This study provides further confirmation of the importance of dietary therapy in cats with inflammatory GI disorders. Clearly, long-term control of IBD with minimal drug administration may be aided by specific dietary management. However, some cats will be only temporarily responsive or only minimally responsive to careful dietary manipulations. Therefore some cats with mild disease will require some form of pharmacologic therapy in addition to dietary manipulation. Most cats with moderate to severe IBD will require pharmacologic therapy, and this is started in conjunction with dietary therapy as soon as a diagnosis is made.
There is no single diet that can be universally recommended for management of IBD in cats. The diet must be chosen based on the dietary history, and then an assessment has to be made as to how well the affected patient embraces the recommended diet. Adjustments may need to be made over time. We now have the advantage of having a wide variety of very palatable commercial diets available, and using commercial diets, compared with home-prepared diets, reduces concern about dietary imbalances significantly. Using commercial diets is also much more convenient for owners.
In general the first step is to select a diet with a novel protein source, that is, something the animal has not been fed before (e.g., duck, venison, lamb, rabbit, whitefish, turkey). The effects of this diet should be assessed over a 3- to 4-week period for therapeutic response and palatability. If there is not a satisfactory response to the first diet and the cat’s condition remains very stable, then an alternate diet can be tried, or, alternatively, drug therapy can be instituted at this point as well. Most owners are anxious for prompt resolution of their pet’s clinical signs, and so I usually try to make a determination as to whether ongoing strict dietary trials will be practical or not.
Many of the commercially available therapeutic diets have been enriched with omega-3 fatty acids. Altering the dietary ratio of omega-6 to omega-3 polyunsaturated fatty acids may affect the inflammatory response of IBD. Omega-3 fatty acids competitively inhibit formation of prostaglandins and leukotrienes derived from arachidonic acid, resulting in decreased concentrations of proin- flammatory fatty acid metabolites. It remains unclear, however, if dietary supplementation with fatty acids is truly beneficial.
Hydrolyzed protein diets have become available for dietary therapy. The theory is that because these diets contain no intact proteins, only peptides of sizes ranging from 6,000 to 15,000 daltons, which are proposed to be nonantigenic, no adverse reaction to the diet will occur. It is still possible, however, for an antigenic response to one of the epitomes of the peptides to occur. Further investigation is needed; however, these diets certainly do represent an attractive option for feeding to some patients with dietary sensitivities or true food allergy.
Recent studies conducted in dogs and cats have shown that cell mediated immunity declines with age. Dietary supplementation with vitamin E appears to enhance this function. Other potential benefits of vitamin E include reduction of oxidative damage and correction of a deficiency of vitamin E that may naturally occur in animals with severe GI disease. Therefore it may be beneficial to provide vitamin E supplementation for dogs and cats with moderate to severe IBD. At this time it is still unclear what dose of vitamin E is best for antioxidant effects in the GI tract. A dose of 100 IU per 10 lb per day is suggested.
For cats with concurrent large bowel disease and symptoms, fiber supplementation may be helpful. Beneficial effects of fiber supplementation include improved fecal character, improved colonic motility, binding of potential colonic irritants, and production of beneficial short-chain fatty acids that positively influence large intestinal structure and function.
Once the disease has been in remission for 6 or more months, adjustments in the type of foods offered can be attempted, based on owner and patient preferences. New ingredients should be added one at a time, and the owner should observe for any adverse effects. If any adverse effects occur, the offending ingredients are removed. Usually several palatable and effective diets can be identified that will be well tolerated over time.
Pharmacologic Therapy for Cats
With IBD
Corticosteroids are the cornerstone of pharmacologic therapy for idiopathic inflammatory bowel disorders. Mild to moderate cases often respond to prednisone or prednisolone at a starting dose of 0.5 to 1 mg/lb divided twice daily for 2 to 4 weeks, followed by a gradual decline in 50% increments at 2-week intervals. Cats with inflammatory changes graded as mild usually respond quite well to the lower dose, and alternate-day or every-third-day treatment can often be achieved by 2 to 3 months. In many but not all cats with mild disease, treatment can be discontinued altogether by 3 to 6 months.
If biopsy specimen analysis reveals disease that is moderate to severe, a dose of 1 to 2 mg/lb divided twice daily is used for the first 4 weeks or until clinical signs resolve. Some clinicians feel that better bioavailability will be achieved in cats with use of prednisolone rather than prednisone. Therefore for more severe cases it may be best to prescribe prednisolone specifically. This dose of corticosteroid is generally very well tolerated in cats. In these cases a dose of 0.5 to 1 mg/lb/day may be necessary long-term (months to years) to maintain clinical remission. Use of combination drug therapy (e.g., prednisolone and metronidazole, or prednisolone and azathioprine) may also be required at the outset to control clinical signs and prevent progression of the disease. Cats with hypoproteinemia and histologic changes graded as severe often respond quite well when an aggressive therapeutic course is undertaken. Dexamethasone (0.15 to 0.25 mg/lb orally every 24 hours) may be useful in cats that are poorly responsive to increased doses of prednisolone.
It has been my experience that young cats (less than 5 years of age) with IBD often do not need to be treated as long as do many middle-age to older cats. This may be due in part to the fact that by the time older cats are diagnosed, the disease is often long-standing and often of a moderate to severe degree. Earlier diagnosis of these older cats in conjunction with appropriate therapy will likely provide a better opportunity for lower daily or alternate-day dosage levels to be successful in maintaining control. I have found that many older cats with moderately severe to severe IBD require prednisone or prednisolone at 1 mg/lb/ day for life for adequate control of all symptoms related to IBD. Combination drug therapy may also be required (see subsequent information). Many clinicians who treat empirically for suspected IBD often use inadequate dosages of corticosteroids (initial dose either not high enough or tapered too early). The importance of evaluating biopsy samples, including periodic follow-up biopsy specimens in some cases, to best tailor a treatment program cannot be overemphasized.
Methylprednisolone acetate (Depo-Medrol) can be used as sole treatment for cats with mild to moderate IBD or as adjunctive therapy when oral prednisolone and/or metronidazole are used as the primary treatment and flare-ups of clinical signs occur. Consistent control of clinical signs in cats with moderate to severe IBD is more difficult to maintain when methylprednisolone acetate is used alone, however. It is recommended that sole use of methylprednisolone acetate be reserved for situations in which the owner is unable to consistently administer tablet or liquid preparations orally. Initially 20 mg is given subcutaneously or intramuscularly and is repeated at 2-week intervals for two to three doses. Injections are then given every 4 to 6 weeks or as needed for control.
Budesonide is a glucocorticoid that represents a new alternative for management of IBD in dogs and cats, especially in severe cases that have proven to be refractory to prednisolone, metronidazole, azathioprine, and dietary management; or that are intolerant of the corticosteroids discussed previously. Budesonide is a new and recently approved corticosteroid for use in humans. It is one of a group of novel corticosteroids that have been in development for use in humans in an attempt to make available alternative preparations that will help limit toxicity associated with corticosteroid use. Others include fluticasone propionate, tixocortol pivalate, and beclomethasone dipropionate.
Budesonide undergoes high first pass metabolism in the liver, and 90% is converted into metabolites with low corticosteroid activity. It has minimal systemic availability. The potential for typical corticosteroid side effects is significantly reduced as a result of decreased bioavailability and the resulting limited systemic exposure, which makes this a particularly attractive drug for use in humans and animals that are poorly tolerant of other corticosteroids. Budesonide also has a high receptor-binding affinity in the mucosa. It has been referred to as a “locally acting” corticosteroid.
Therapeutic results with budesonide have been promising in humans with Crohn's disease, collagenous colitis and lymphocytic colitis, ulcerative colitis, either when administered as a retention enema or in oral form, and primary biliary cirrhosis. Budesonide has been used by some veterinary clinicians in recent years to treat IBD in dogs and cats. Dosage recommendations vary. In humans, a range of 6 to 9 mg per day has been used during initial therapy. The following general recommendations have been made for dogs and cats. In general, budesonide is administered to cats and small dogs at 1 mg once per day. It has been used at higher doses (3 mg per small dog or cat per day), but the lower dose is frequently effective. Large dogs receive 3 mg twice daily initially, and the dosage is later tapered to 3 mg once daily, and then to alternate day administration for longer term use.
Budesonide can be used in combination with other drugs. Since cats tolerate corticosteroids very well, there is little indication to use budesonide as a primary therapy for IBD. However, this may be a very attractive option for use in diabetic cats that also have IBD.
Potential adverse effects include PU/PD, when budesonide is used at the high end of the dose range, and GI ulceration. These reactions have been observed in some human patients. These problems would be more likely to occur in dogs than in cats. It appears to be very safe when used at the levels listed above.
When combination therapy is indicated, metronidazole is usually the first choice to be used in conjunction with prednisolone. It can also be used as sole treatment in some cases (e.g., in the unusual event that a cat cannot tolerate corticosteroids, or if their use is contraindicated). Metronidazole's mechanism of action includes an antiprotozoal effect, inhibition of cell-mediated immune responses, and anaerobic antibacterial activity. A dosage of 5 to 10 mg/lb twice daily is used for IBD. Ideally at least several months of metronidazole therapy is given once it is started. In some cats with severe disease, long-term consecutive use (months to years) or 1- to 2-month cycles of treatment may be required.
Side effects of metronidazole at this low dose are uncommon in cats. Adverse reactions that have been observed include primarily GI (inappetence, nausea, and occasionally vomiting and/or diarrhea) and neurologic (ataxia, seizures, disorientation) problems. In my experience, neurologic side effects are very rare when the dose range recommended here is used, for whatever duration (weeks to months to years). I have observed two cats that were treated with prednisone and metronidazole (5 mg/lb twice a day in one, and 7 mg/lb twice a day in the other) for IBD that developed rear limb ataxia within 3 to 4 days of the start of therapy. In both cases the metronidazole was discontinued within 24 hours and the ataxia completely resolved within 2 to 4 days. Metronidazole was not reinstituted in either cat.
The most troublesome problem that the owners of my patients have encountered with metronidazole is excessive salivation after pill administration in cats. Metronidazole is known to have a sharp, unpleasant metallic taste. Most cats are given half to one quarter of a 250-mg tablet per dose, and the taste of broken sections is apparently quite bitter. Salivation does not occur when the medication is administered directly to the back of the mouth and quickly swallowed. If, however, the pill is retained in the oral cavity for even the shortest time, the battle is most likely lost! Recompounding metronidazole into a tasty suspension form often makes the task of administering metronidazole much easier.
Metronidazole has shown evidence of carcinogenic activity in studies involving chronic oral administration in mice and rats. There are reports of humans with Crohn's disease who have been treated with high doses of metronidazole for prolonged periods of time and in whom breast or oral cancer subsequently developed. A cause-and- effect relationship has not been established. To date I am aware of no cases of GI or mammary cancer that have occurred in dogs or cats in conjunction with metronidazole use. I consider it to be a safe drug for prolonged use (months to years) in patients with chronic disorders for which longterm therapy is required.
If remission cannot be maintained with use of corticosteroids and metronidazole, azathioprine (Imuran) should be added to the treatment regimen. There is no need to reduce the prednisolone dose in cats when azathioprine is used in conjunction. It may not be necessary to continue metronidazole after completion of the first 4 weeks of azathioprine therapy. This decision is best made on an individual case basis. Azathioprine is a potent immunosuppressive drug. It is metabolized to 6-mercaptopurine, its active metabolite, which functions to interfere with antigenic triggering of lymphocytes. Replication of rapidly dividing cells, including immunoblasts, is inhibited, and there is interference with cellular function. Azathioprine is usually used in cats only when the previously discussed therapeutic measures fail to control the disease. The most important side effect of azathioprine in cats is bone marrow suppression.
I use a maximum starting dose of azathioprine in cats of 0.15 to 0.23 mg/lb once every other day. At this low dose, side effects are very uncommon in my experience, but I have seen one cat develop significant pancytopenia within 4 weeks of the start of therapy. The cat gradually recovered after immediate cessation of azathioprine. One blood transfusion was required. Alternatively, if clinical signs of IBD do not resolve on the initial azathioprine dose, the dose can gradually be increased if there is no evidence of bone marrow suppression. Because of lag effect, beneficial therapeutic results from azathioprine are often not apparent until 3 to 4 weeks after treatment is started. Azathioprine is generally used for 3 to 9 months or longer in cats. A maj ority of cats with IBD do not require azathioprine treatment.
A complete blood count and platelet count should be run to monitor for anemia, leukopenia, and thrombocytopenia before the start of therapy with azathioprine and at 3- to 4-week intervals for the first 2 months, and then once every 2 months. Significant side effects are most often identified during the first 3 to 6 weeks of treatment. There is usually no physical evidence of early azathioprine toxicity in cats. Mild leukopenia (e.g., 3000 to 4000 cells∕μl) is usually the first abnormality that is identified. Azathioprine is currently available only as 50-mg tablets. Because it is too difficult to break azathioprine into a consistent fragment size for cats, it should always be recompounded into an oral suspension form for administration to cats. A major advantage of administering azathioprine in this manner is that any required increase in dosage can be done very accurately. If azathioprine is well tolerated and there has been inadequate clinical improvement, the dosage can be increased from 0.15 mg/lb to 0.2 mg/lb to 0.25 mg/lb every 48 hours.
Another immunosuppressive drug that is used in some cats with severe IBD is chlorambucil (Leukeran). Some clinicians use chlorambucil as an alternative to azathioprine (they are not used in conjunction). Chlorambucil is an alkylating agent. Alkylating agents alter DNA synthesis and inhibit rapidly proliferating cells. Chlorambucil is administered initially at 0.05 to 0.1 mg/lb/day in conjunction with prednisolone at 1 mg/lb/day. The small pill size of chlorambucil (2 mg) allows for easy dosing. Most cats receive one-half tablet (1 mg) per day. Various dosage schedules for cats have been published. An alternate schedule is 0.07 to 0.15 mg/lb every 72 hours. Toxicities are uncommon in cats but may include anorexia, vomiting, and diarrhea, but these problems generally resolve rapidly when chlorambucil is reduced from daily to every-other-day administration. Bone marrow suppression is possible but uncommon and is mild and rapidly reversible when it does occur. Once the desired clinical response is achieved, chlorambucil is gradually tapered over several months while prednisolone is continued as the primary maintenance drug.
Colostrum is currently recognized as an emerging therapy for various inflammatory disorders in human medicine. Some patients with infectious diarrhea caused by Cryptosporidium parvum have also benefited from bovine colostrum immunoglobulin concentrate. Animal studies have shown promise, and so colostrum also represents a potential alternative therapy for various disease conditions in animal patients. Colostrum is particularly rich in immunoglobulins, antimicrobial peptides (e.g., lactoferrin and lactoperoxidase), and other bioactive molecules, including growth factors. Recent studies have suggested that the peptide growth factors in colostrum might provide novel treatment options for a variety of GI conditions, as well as other disorders. The growth factors in colostrum include insulinlike growth factor I and II (IGF-1 and IGF-2), epithelial growth factor (EGF), transforming growth factors A and B (TGFs A and B), growth hormone (GH), fibroblast growth factor (FGF), and platelet derived growth factor (PDGF). Bovine colostrum is an excellent source of growth factors and immunoglobulins, and it will most likely be the main source for therapeutic supplies of colostrum, since it is readily available in large supplies, as opposed to human colostrum. The growth factors in bovine colostrum reportedly boost cell and tissue growth by stimulating DNA and RNA formation, and also assist in repairing and replacing cell structures. Other beneficial effects include increases in T cell numbers. Antiaging effects are currently under investigation in humans.
Proposed mechanisms of action for colostrum in IBD include inhibition or prevention of reproduction of pathogenic invaders and protection against toxins through the action of immunoglobulins, lactoferrin, and other immune factors, and stimulation of repair of intestinal membranes at the cellular level through actions of epithelial growth factors. There may also be an enhanced effect of assimilation of nutrients.
Currently colostrum can be considered as an alternative therapeutic option for animals with IBD that are poorly responsive to conventional medications and dietary trials. Colostrum has been effective in improving the stool consistency of some animals with chronic diarrhea caused by IBD. Results in human trials have been promising, and use of colostral-derived preparations may become more prevalent in the next several years. Studies are needed to help determine the most effective dose.Various preparations are currently available in health food stores.
Cats with hypereosinophilic syndrome should be treated aggressively as soon as a diagnosis is established. Prednisolone (1.5 to 2 mg/lb divided twice a day for 2 to 4 weeks, then reduced to a maintenance dose of 1 to 1.5 mg/lb/day), metronidazole, and azathioprine should be used in conjunction. Contrary to early reports that characterize this severe eosinophilic enteritis syndrome as very poorly responsive to treatment, early aggressive therapy can help achieve a state of remission in some patients that can last for months to several years or more. Cats with eosinophilic enteritis, which is a much milder disease than hypereosinophilic syndrome, generally respond well to corticosteroids alone (follow guidelines for treatment of mild to moderate IBD).
Antibacterial therapy can be quite beneficial in some situations, most notably for treatment of patients that are suspected of having a bacterial cause or component of IBD and CPE. Indications for use of antibiotics include histologic changes that include presence of neutrophils or evidence of crypt abscesses or poor initial response to antiinflammatory therapy. Intestinal bacterial problems occur more commonly in dogs than in cats. CPE can cause intermittent or chronic diarrhea (see Chapter 8). Definitive diagnosis requires identification of C. perfringens enterotoxin in fresh feces (assay available at commercial laboratories). Amoxicillin, metronidazole, and tylosin appear to be the most effective antibiotics for treatment of CPE. Occasionally only tylosin is effective (1∕i6 tsp Tylan Soluble powder administered in capsule form twice a day for cats). Cats generally will not eat food to which tylosin powder has been added. Antibiotics used most commonly for bacteria-related intestinal problems in cats include amoxicillin, metronidazole, enrofloxacin, and trimethoprim-sulfa.
Usually a 2- to 4-week course of antibacterial therapy is adequate (adjunctive treatment in cases in which the inflammatory disease is considered most significant). In cats with IBD that experience intermittent flare-ups of diarrhea, the most commonly successful therapeutic maneuvers are use of antibiotics for 2 to 3 weeks at a time or use of more aggressive antiinflammatory measures. Because metronidazole has both antibacterial and antiinflammatory activity, it is an excellent choice for use in cats in which symptoms are not well controlled by corticosteroids alone. Metronidazole is often used in these situations for several months or more at a time.
Some cats with concurrent IBD and colitis may show minimal or no clinical signs of colitis. Initiation of treatment specific for colitis (sulfasalazine [Azulfidine] at 5 to 7 mg/lb two times daily for 7 to 10 days at a time and increased dietary fiber) may result in dramatic improvement in cats with enterocolitis. It is interesting to note, however, that cats with colitis generally demonstrate a much better response to corticosteroids than do dogs. Therefore sulfasalazine is used much less commonly in cats that in dogs.
As described earlier, significant tissue-level cobalamin deficiency is present in some patients with GI disease. This is usually secondary to reduced cobalamin absorptive capacity. Therapy involves administering injectable cobalamin at the following schedule for cats: 250 μg subcutaneously once a week for 6 weeks, then every 2 weeks for the next six doses, then once monthly. Most generic cobalamin preparations contain 1 mg/ml (1000 μg∕ml). It is important to note that multivitamin and B- complex injectable formulations contain significantly lower concentration of cobalamin and they also cause pain when injected. Therefore it is recommended that these preparations not be used for cobalamin supplementation. Unless the intestinal disease is totally resolved, long-term and perhaps lifelong supplementation with cobalamin may be necessary. The frequency of injections on a longterm basis is determined by regular measurement of serum cobalamin concentration.
Poor responses to treatment of cats with IBD usually result from the following:
1. Inadequate initial or long-term maintenance corticosteroid dosage
2. Failure to use ancillary medications (metronidazole, azathioprine, chlorambucil) in cases in which disease is moderate to severe
3. Failure to recognize and treat a concurrent condition (e.g., gastric hypomotility disorder that may either be secondary to IBD or idiopathic in nature, hyperthyroidism, parasitism [e.g., Giardia, Cryptosporidium], CPE)
4. Poor owner compliance
5. Treatment for only small intestinal inflammatory disease when colitis is present as well (colitis that might respond better to sulfasalazine than to corticosteroids or metronidazole)
6. Failure to recognize and treat low body cobalamin levels (measure serum cobalamin)
7. Failure to identify an effective diet
Management of Dogs With IBD
Specific treatment recommendations for dogs with IBD are as follows. Corticosteroids are the initial treatment of choice for lymphocytic-plasmacytic and eosinophilic enteritis. Mild to moderate cases (as determined by clinical signs, normal protein levels, and degree of inflammatory cell infiltrate on biopsy specimens) often respond to prednisone at a dose of 0.25 to 0.75 mg/lb divided twice daily for 2 to 4 weeks, followed by a gradual decrease in 50% increments at 2-week intervals. Alternate-day or every-third-day treatment can often be reached by 2 to 3 months. Occasionally treatment can be discontinued altogether by 3 to 6 months.
Moderate to severe cases and any case in which the total protein is less than 5.5 g/dl should be treated more aggressively using an initial prednisone dose of 1 mg/lb/day for 2 to 4 weeks before an attempt is made to decrease the dose. Dogs in this category often require long-term therapy (months to years) on an every-other-day or every-third-day basis to maintain remission. Use of combination drug therapy (prednisone and metronidazole) in these cases at the outset is recommended to improve chances of controlling clinical signs more quickly and to prevent progression of the disease.
If significantly bothersome side effects are caused by prednisone (e.g., severe polyuria/ polydipsia, panting, lethargy), either oral dexamethasone or budesonide can be used instead. Budesonide is a new oral corticosteroid that was described earlier in the section on management of IBD in cats. Its use should be considered in any case where conventional corticosteroids may be problematic, for example, where side effects are very significant or in diabetic animals or those with Cushing's disease that also require management for IBD. In general, budesonide is administered to small dogs at 1 mg once per day. It has been used at higher doses (3 mg per small dog per day), but the lower dose is frequently effective. Large dogs receive 3 mg twice daily initially, and the dosage is later tapered to 3 mg once daily, and then to alternate day administration for longer term use. In some dogs, dexamethasone is much better tolerated than prednisone and side effects are minimal or nonexistent. If prednisone side effects are judged to be severe, it is generally discontinued for 12 to 36 hours to allow for adequate metabolism and clearance. Prednisone may then be reintroduced at 25% to 50% of the previous dose, or, alternatively, dexamethasone can be instituted at a conservative level (0.005 to 0.01 mg/lb/day orally). Some dog breeds are very sensitive to steroids and are poorly tolerant of prednisone doses over 0.5 to 0.75 mg/lb/day Arctic breeds and rottweilers are often in this category.
As was discussed in the section on treatment of cats with IBD, metronidazole has both antibacterial and antiinflammatory effects. It is very useful in treatment of IBD in dogs, as well as in cats. Metronidazole is administered at 5 to 10 mg/lb two times daily. A major advantage of using combination therapy is that the corticosteroid dose can usually be decreased from the high initial dose in a timely manner, thus decreasing the likelihood of significant corticosteroid-related side effects. Also, I have successfully managed on a long-term basis canine patients with mild to moderate lymphocytic-plasmacytic enteritis that were intolerant to corticosteroids on metronidazole alone.
When prednisone and metronidazole are used in combination, the dosage level of each drug is generally gradually decreased as the patient's condition improves and laboratory parameters (especially protein levels and white blood cell count) return to normal. Corticosteroids are decreased gradually for several months before any reduction is made on the metronidazole dose. If there has been an excellent response, it is possible that metronidazole can be discontinued after several months. Alternatively, if chronic therapy is required, metronidazole can often be administered on a once-daily basis and eventually on an every- other-day basis. If it is not possible to discontinue medication altogether owing to recurrence of symptoms when no medication is given, control can be maintained with prednisone and/or metronidazole given on an alternate-day basis. If both drugs are used, I often recommend giving prednisone on one day and metronidazole on the alternate day. Occasionally in dogs with moderate to severe IBD or in a case in which both IBD and chronic bacterial overgrowth are present, it is necessary to continue metronidazole on a longterm (months to years) basis (5 to 7 mg/lb twice daily). I have observed no instances of significant complications when this protocol has been used.
Dogs with marked hypoproteinemia (total protein less than 4.5 g/dl) caused by severe lymphocytic-plasmacytic enteritis often respond well when an aggressive therapeutic course is undertaken (prednisone, metronidazole, and azathioprine used in combination). This aggressive approach has led to control of clinical signs and return to a total protein level of greater than 6.0 g/dl (by 2 to 4 months) in a number of cases. One exception to this approach in my experience is that patients with hypoproteinemia resulting from eosinophilic enteritis often respond well to corticosteroids alone.
Combination drug therapy is used early in severe cases or if a side effect to one drug requires that it be used at a lower dose. If corticosteroids are poorly tolerated (e.g., excessive polyuria/polydip- sia, listlessness, panting, inappetence associated with steroid hepatopathy) or if corticosteroids and metronidazole are unable to achieve remission, azathioprine should be added to the regimen. Azathioprine is started early in the course for cases of lymphocytic-plasmacytic enteritis that cause a protein-losing enteropathy and result in a total protein level less than 4.5 g/dl.
The canine dose of azathioprine is 1 mg/lb/day (note significant difference in dose between cats [0.15 mg/lb once every other day] and dogs). If azathioprine is used at the outset, the prednisone dose is decreased by 50% from 1 mg/lb/day after 3 to 4 weeks or based on clinical improvement (i.e., remission of signs and increase in protein levels) and degree of tolerance of this dose of prednisone. Subsequent decreases in the prednisone dose can usually be made at monthly intervals until an alternate-day schedule is reached. If azathioprine is started in any type of IBD case because of significant corticosteroid side effects, the prednisone is initially decreased by 50% to 75% but is not stopped completely unless absolutely necessary because loss of remission might result.
Azathioprine is generally used for 3 to 9 months in dogs. Once adequate control is achieved, the daily dose is decreased by 50%, and subsequently alternate-day therapy is used. Side effects are uncommon in dogs but may include anorexia, jaundice (hepatic damage), poor hair growth, and bone marrow suppression. In addition, it is suspected that azathioprine has the potential to induce pancreatitis (this is an uncommon occurrence, however, in my experience). A complete blood count should be run to monitor for evidence of anemia or leukopenia at 3-week intervals for the first 2 months and then once every several months. Routine monitoring also includes periodic (once every 4 to 6 weeks initially) evaluation of hepatic enzyme levels (increases may be due to corticosteroids and occasionally azathioprine) and protein levels.
Colostrum, which is currently recognized as a potential new adjunctive therapy for IBD patients that do not respond fully to more conventional therapies, was described in the section on management of IBD in cats. There may be indications for use of colostrum in dogs as well. Therapeutic trials in dogs are needed to determine whether or not this is a useful option to consider.
IBD that is initially graded as moderate to severe can usually be managed quite successfully and can be maintained in remission but not often cured. Sometimes follow-up biopsy specimen analyses in severe cases reveal only slight to moderate histologic resolution of inflammatory infiltrates despite excellent clinical control even on lower drug doses. Alternatively, dramatic histologic resolution has been noted in other cases. Treatment decisions (e.g., can treatment be discontinued completely?) ideally are based on a thorough review of clinical response to date (control of clinical signs, levels of medication required, and resolution of hypoproteinemia if it was initially present) and follow-up endoscopic biopsy specimen information.
As a general clinical rule of thumb, an attempt can be made to discontinue therapy after 2 to 3 months of successful control on twice-weekly medication. If signs recur, medication is resumed on a daily basis for 7 to 14 days before a gradual reduction program is started. In some dogs with severe lymphocytic-plasmacytic enteropathy and marked hypoproteinemia, therapy can be successfully discontinued as early as 6 months to 1 year. In others, lifelong treatment is required.
Cobalamin deficiency and associated clinical signs were described in the section on IBD in cats. For dogs that are thought to be deficient in cobalamin, supplementation is as follows: dogs up to 10 lb, 250 μg per injection; 10 to 30 lb, 500 μg per injection; and over 30 lb, 1000 μg per injection. As with cats, injections are administered once weekly for 6 weeks, then every 2 weeks for six doses, and then once monthly. The incidence of low tissue cobalamin levels in dogs with chronic intestinal disease is not known, but it is recommended that dogs with a history of chronic GI disease be investigated for this possibility by running serum cobalamin assays.
Dietary Therapy
In some patients with mild lymphocytic-plasmacytic enteritis or eosinophilic enteritis, dietary modification may lead to partial or complete resolution of clinical signs and even improvement in histologic lesions. In others, dietary therapy may be an important adjunct to pharmacotherapy in the control of clinical signs related to chronic IBD. It is also possible that dietary management used on a long-term basis will effectively help maintain control once drug therapy is discontinued. Potential benefits of dietary therapy include reduction of hypersensitivity reactions to dietary antigens, alteration of bowel motility, and effects on composition of the bowel flora and mucosal morphology and function.
Dietary therapy for IBD may involve use of a strict elimination diet or a balanced commercial diet that contains minimal additives. In most cases, diets that are highly digestible and have low residue work best for small intestinal disease. If a decision is made to manage a patient initially with dietary therapy alone, the dietary trial should be conducted for a minimum of 3 to 4 weeks. Some patients require 6 weeks or more before clinical improvement occurs. If biopsy results reveal moderate to severe IBD and/or if there is any degree of patient compromise, pharmacotherapy should be included in the treatment regimen along with dietary management. In my experience, patients with this degree of disease rarely respond to dietary manipulation alone.
Diets that often work well include those that supply a single source of protein to which the patient has not previously been exposed (i.e., “novel” proteins). These may include lamb, rabbit, venison, duck, whitefish, or low-fat cottage cheese. A single digestible carbohydrate such as boiled rice should be added to home-prepared diets. Many of the premium commercial diets now include optimum levels of omega-6 and omega-3 fatty acids. These agents may be useful in reducing inflammation in the intestine. Dividing feedings into two to three meals per day will help maximize dietary assimilation.
Unusual Complications in Patients With Inflammatory Bowel Disease
Several complications associated with IBD or its treatment have been reported. These include the potential for IBD to progress to lymphoma, hemorrhagic diathesis secondary to intestinal malabsorption of fat and the fat-soluble vitamin K, and toxoplasmosis in cats on immunosuppressive therapy for treatment of IBD.
Lymphoma. It has been recognized in cats, dogs, and humans that IBD can progress to lymphoma. In one report, three of nine cats with lymphocytic-plasmacytic gastroenteritis confirmed by full-thickness biopsy, diagnosed during a 1-year period, subsequently developed GI lymphoma 9 to 18 months after the initial diagnosis. Clinical signs initially resolved in all cats in response to management with hypoallergenic diets but later recurred in the three cats with lymphoma.
To date the progression has been found overall to be an uncommon occurrence. No one type of IBD is recognized as more likely than others to progress to lymphoma. It has occurred in cats with an original diagnosis of lymphocytic enteritis, lymphocytic-plasmacytic enteritis, or lymphocytic-plasmacytic-eosinophilic enteritis.
In my four feline cases in which progression occurred, initially there was excellent control of the inflammatory bowel disorder with conventional treatment. All four cats required chronic medication to control clinical signs, and at a range of 1 to 3 years, clinical remission was lost. Followup histologic evaluation is recommended in patients with IBD if previous treatment is no longer successful in controlling clinical signs in order to detect and treat lymphoma as early as possible.
Hemorrhagic Diathesis. One report described two cats with hemorrhagic diathesis that was thought to be related to a chronic malabsorption of fat and the fat-soluble vitamin K. Both cats experienced a sudden onset of bleeding. In one there was an acute intraabdominal bleeding episode, whereas in the other there was spontaneous and extensive subcutaneous hemorrhage. Both cats had marked lymphocytic-plasmacytic enteritis with villous atrophy.
Spontaneous bleeding is an infrequent but well-documented complication of intestinal malabsorption in humans. The acquired hemorrhagic diathesis is characterized as a hypoprothrombine- mic disorder secondary to malabsorption of vitamin K. The fact that this occurs infrequently in patients with malabsorption is probably attributable to absorption of bacterially derived vitamin K2 from the ileum and colon.
Treatment involves subcutaneous injections of vitamin K (oral administration should be avoided because the active absorption of vitamin K from the duodenum is unpredictable in patients with malabsorption). Its use is also indicated before surgery when abnormal clotting is detected. Chronic maintenance therapy (oral vitamin K) may also be required. Dietary fat requirements of patients with malabsorption should be met by short- or mediumchain saturated fatty acids, because absorption of vitamin K is reduced by progressively longer chain fatty acids and greater degrees of unsaturation.
Toxoplasmosis. Intensive immunosuppressive therapy for IBD can potentiate reactivation of latent infections. Toxoplasmosis was reported in two cats that were initially diagnosed with and treated for IBD. Toxoplasma gondii was found on follow-up biopsy (full thickness) of the intestine in one cat 9 weeks after endoscopic biopsy specimens had revealed severe lymphocytic-plasmacytic gastroenteritis. Treatment had included prednisone, metronidazole, and azathioprine. Both cats had serologic evidence of active toxoplasmosis. In cats treated with azathioprine, it is hypothesized that active toxoplasmosis was attributable to reactivation of a prior infection, resulting from the immunosuppressive effects of prednisolone and azathioprine. Both cats had no signs of illness other than GI tract disease (diarrhea, weight loss). Recent coincidental infection was considered highly unlikely because both cats were kept strictly indoors and were fed controlled diets.
Experience from these two cases indicates that toxoplasmosis should be considered in cats with IBD if signs of illness (i.e., GI type of signs) occur during treatment with immunosuppressive drugs.
Recurrent signs of IBD may actually not be due to failure of the current treatment regimen. Diagnosis of toxoplasmosis is based on serologic documentation of active toxoplasmosis (IgM titers should be done because they may permit earlier diagnosis than is possible with IgG titers) and response to an anti- Toxoplasma drug (clindamycin is recommended). Treatment for IBD is continued as needed.