Initial evaluation
The first step in the investigation of virtually all clinical problems is a thorough history.With a patient presenting for chronic vomiting, it is essential to determine if the animal is in fact vomiting as opposed to regurgitating (Figure 2.1).
Vomiting is usually preceded by nausea, which may be manifested by pacing, depression, lip licking, swallowing, salivation, and occasionally vocalization (cats). Retching, non-productive, rhythmic, abdominal contractions usually follow, culminating in the act of vomiting. In contrast, regurgitation occurs passively, with animals expelling tubular undigested food or foamy white liquid with little or no effort. Vomitus may contain bile pigment, while regurgitation should not. Both may look “digested” especially if regurgitated food has been retained in the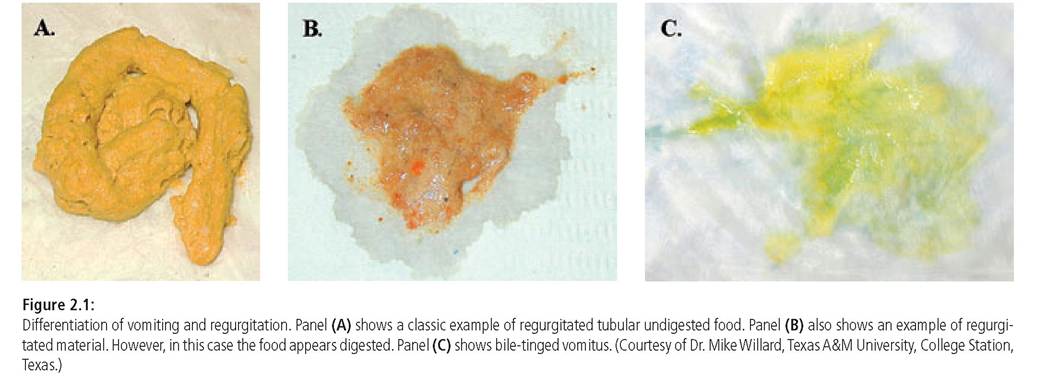
esophagus for a prolonged period of time, so this is not a reliable distinguishing characteristic.
Once it has been established that the animal has truly been vomiting, a more targeted historical investigation should be performed. First, a thorough dietary history should be obtained. It is especially important to question the owner for any evidence of dietary indiscretion, including ingestion of table scraps, garbage, foreign materials (including excessive amounts of hair), toxins, or plants (especially in cats). Questions concerning the consistency of the current diet or any dietary changes should also be asked. The content of the vomitus needs to be examined, looking for the presence of bile, undigested food, or clear liquid. Fresh or digested blood strongly suggests gastrointestinal ulceration; whereas, hair suggests the presence of trichobezoars or a motility disorder. Furthermore, the duration, frequency, and progression of the vomiting may also point to an underlying etiology.
It is common for healthy cats to vomit occasionally up to once weekly; however, changes in the frequency or development of concurrent clinical signs such as anorexia warrant further investigation. It is also important to evaluate any temporal relationship between vomiting and eating. Although not pathognomonic, vomiting of undigested or partially digested food 8-10 hours after eating may indicate a gastric outflow obstruction or another gastric motility disorder.It is also very important to determine what medications the animal is currently being given. Although most medications (e. g., antibiotics, chemotherapeutics, and digoxin) cause acute vomiting, they may play a role in chronic vomiting, especially if the connection between the two events is not made initially or the vomiting is mild and sporadic. Non-steroidal antiinflammatory drugs (NSAIDs) and steroids, when used chronically, can lead to chronic vomiting and hematemesis secondary to gastrointestinal ulceration, and thus, the potential use of these drugs should always be inquired of specifically.
Signalment and past history also can be extremely helpful. For example, a Miniature Schnauzer with previous bouts of pancreatitis may suggest another episode of pancreatitis. Finally, a thorough body systems review may also facilitate a diagnosis. The presence of concurrent clinical signs such as diarrhea, dyschezia, coughing, sneezing, polyuria, dysuria, anorexia, and lethargy all may provide important information, which not only may help to pinpoint the cause of the vomiting, but also to decide on how aggressive to pursue a diagnosis. Finally, inquiry into the patient’s vaccination status, deworming schedule, and travel history may help in ruling out particular infectious diseases.
Also a “head to tail” physical examination building on the history can pick-up subtle abnormalities. The physical examination is essential for localizing the cause of the clinical signs and ascertaining the severity of disease.
First, the body condition needs to be assessed, along with mentation and gait observed from a distance. Also, special attention should be paid to the presence of cranial abdominal pain or discomfort, a distended colon (especially in cats), linear foreign bodies caught around the base of the tongue (especially in cats), irregular or painful kidneys, organomegaly, thyroid nodules (in cats), abdominal masses, and other signs of systemic disease such as evidence of weight loss, dehydration, altered mentation, icterus, cardiac arrhythmias, mucous membrane pallor, pyrexia, or oral ulceration. Chronically vomiting dogs and cats are most often well hydrated; if the animal is vomiting frequently enough to become significantly dehydrated, the patient will usually present acutely. A digital rectal examination, especially to evaluate the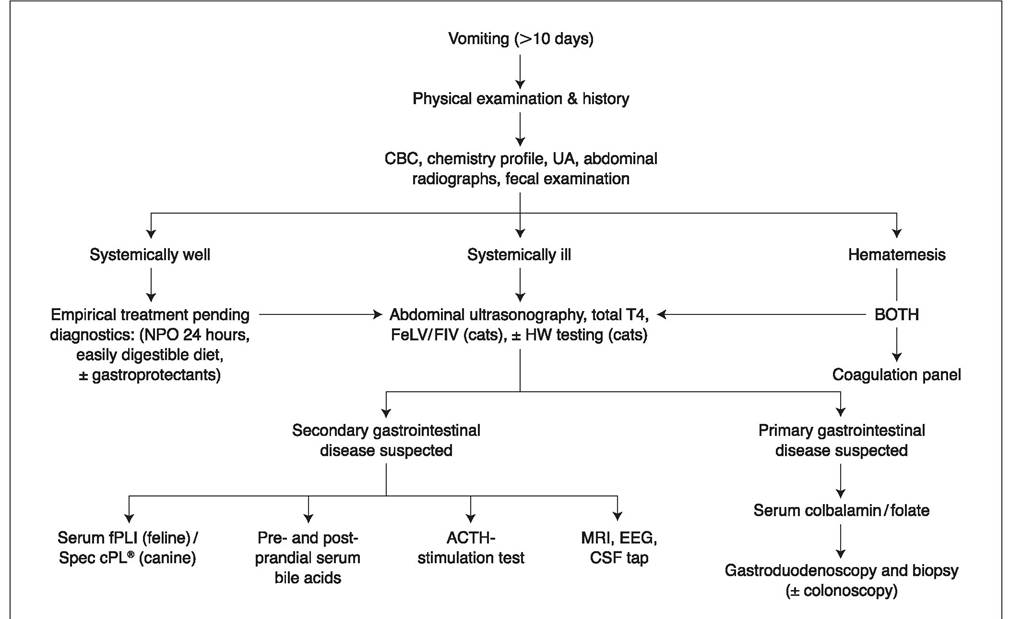
Figure 2.2:
Systematic diagnostic approach to patients with chronic vomiting. This figure shows a suggested systematic workup for dogs and cats with chronic vomiting. CBC = complete blood count; UA = urinalysis; FeLV = feline leukemia virus; FIV = feline immunodeficiency virus; HW = heartworm; NPO = nothing per os; MRI = magnetic resonance imaging; EEG = electroencephalogram; CSF = cerebrospinal fluid; ACTH = adrenocorticotrophic hormone; fPLI = feline pancreatic lipase immunoreactivity; Spec cPL® = canine pancreas-specific lipase.
feces for consistency and signs of occult bleeding, is also crucial. Neurological disease may lead to chronic vomiting and clinical signs of vestibular disease, such as a head tilt, ataxia, or nystagmus may be present. A complete neurological examination may be needed to detect more subtle central nervous system abnormalities. The combined findings from signalment, history, and physical examination allow the clinician to develop a complete clinical picture that will aid in formulating a list of differential diagnoses and necessary diagnostics.
2.2.3