Laboratory assessment of gastric disease
Jan S. Suchodolski
1.4.1.1 Introduction
While routine laboratory tests are nonspecific for gastric disease, they should always be performed in a patient with clinical signs consistent with gastric disease in order to rule out conditions that can lead to similar clinical signs or systemic disorders that can affect the stomach (e.g., renal failure).
Determination of packed cell volume and total protein allow for evaluation of blood and protein loss in patients with gastric ulcers and also allow evaluation of the hydration status in patients that vomit. Animals with gastric ulcers may show a regenerative anemia and decreased total protein concentration. Chronic vomiting may lead to loss of electrolytes (mainly sodium and potassium) and acid-base disturbances (metabolic alkalosis or acidosis). Anemia, hypoglycemia, and increased liver enzymes may be observed in animals with gastric tumors.Gastroscopy is currently the gold standard for diagnosis of gastric disease (see 1.5). In recent years, several new diagnostic tests for gastric disease have been developed. However, at the current time most of these new tests are employed predominantly in a research setting.
1.4.1.2 Evaluation for parasitic infestation
The feline stomach worm (Ollulanus tricuspis) can be detected during microscopic examination of vomitus. Eggs of the feline and canine stomach worm (Physaloptera rara) can be detected in fecal smears or by fecal sedimentation.1
Diagnosis of Helicobacter spp. infection
Bacterial culture for isolation of Helicobacter spp. only has a limited yield. Gastroscopy allows direct visualization of gastric lesions and also enables the collection of samples for indirect detection of these organisms. Helicobacter spp. can be detected in biopsy specimens obtained during gastroscopy by means of histopathology (Warthin-Starry or modified-Steiner stain), immunohistochemistry, polymerase chain reaction, or rapidurease tests.2 Alternatively, an impression smear can be taken from the gastric mucosa using a cytology brush.
The brush is then rolled across a microscope slide and the slide is stained either with May-Grunwald-Giemsa, Gram, or Diff-Quick stain.2 Many animals show a patchy distribution of Helicobacter spp. infestation and it is crucial that biopsy specimens or impression smears are obtained from several areas of the sto- mach.3Minimally-invasive detection methods for Helicobacter spp. infection are easy to perform but have the limitation that they do not allow for identification of the presence of gastric disease. Detection of antibodies directed against Helicobacter spp. in serum has a relatively low sensitivity. In addition, antibodies circulate for up to 6 months after eradication of the organism and thus these antibody tests can not be used for the monitoring of therapeutic success.4 The 13C-urea breath or blood test is based on the detection of metabolic activity of Helicobacter spp.5 The organisms produce the enzyme urease, which catalyzes the metabolism of orally administered 13C-urea. The 13C is released from the urea, incorporated into 13CO2, and can be quantified in either breath or blood samples.5 This test can be used for both diagnosis and monitoring of therapy, but is not offered commercially at this time.
1.4.1.3 Sucrose permeability testing
Increased gastric permeability has been observed in human beings with gastric ulcers and NSAID- or Helicobacter-pylori- associated gastritis. Gastric permeability has traditionally been evaluated using radioactive markers (51Cr-EDTA). Alternatively, the disaccharide sucrose can be used as a specific nonradioactive marker for gastric permeability.6 Orally administered sucrose is too large to permeate the intact gastric mucosa and an increase in the urine (validated for dogs and cats) or serum (validated for dogs only) concentration of sucrose is indicative of an increased gastric permeability and is highly suggestive of gastric mucosal damage.
1.4.1.4 Minimally-invasive markers for gastric disease
Serum concentration of gastrin can be measured in both dogs and cats using an assay developed for measurement of gastrin in human serum. Gastrin is very labile and the serum must immediately be separated from the blood cells, frozen, and shipped on ice. It has been suggested that a 24-hour fasting serum gastrin concentration that is increased above 10-fold of the upper limit of the reference range is suggestive for a gastrinoma in dogs. However, this recommendation is based on human beings where atrophic gastritis is a common cause of moderate increases in serum gastrin concentrations. In contrast, atrophic gastritis has only been reported in the Norwegian Lundehund and other diseases that are associated with an increased serum gastrin concentration can easily be ruled out in the dog. However, if any uncertainty remains, a secretin stimulation test should be performed (see 9.4).
C-reactive protein, a highly sensitive but nonspecific marker of inflammation, correlates well with the degree of experimentally induced damage of the gastric mucosa.7 Also, an increased plasma lactate concentration (>6.0 mmol/L) has been shown to be a negative prognostic marker for post-operative survival time in dogs following gastric dilation/volvulus.8 Further studies evaluating the correlation of plasma lactate concentrations with long-term survival are warranted. Measurement of immunoreactive pepsinogen has been useful as a research tool for the diagnosis of gastritis in dogs, but has no diagnostic value in individual patients with spontaneous di- sease.9
1.4.1.5 Analysis of gastric juice
Analysis of gastric juice is performed rarely in veterinary medicine. This is due to the technical complexity and limited standardization. Also, analysis of gastric juice shows poor correlation with endoscopic and histopathological findings. The pH of gastric juice and concentrations of hydrochloric acid and pepsin can be evaluated either at baseline or after stimulation with pentagastrin.
Gastroduodenal reflux can be demonstrated by use of a radioactive marker that is excreted in bile.101.4.1.6 Evaluation of gastric emptying time
Scintigraphy is currently the gold standard for evaluation of gastric emptying but requires the use of a radioactive marker. Alternatively, a radiopaque marker, such as barium-impregnated polyethylene spheres (BIPS), can be used. These markers have the disadvantage that, depending on their size, they only mimic emptying of either solid or liquid food.11 Recently, 13C-octanoic acid breath tests have been introduced to assess gastric emptying time in dogs and cats.12 These tests allow labeling of a complex meal with 13C-octanoic acid, a mediumchain fatty acid that is absorbed in the duodenum and oxidized in the liver, where the 13C is released. A rise in 13CO2 in the expiratory air indicates that gastric emptying has occurred.
cat exclusively synthesizes intrinsic factor in the exocrine pancreas.3,4
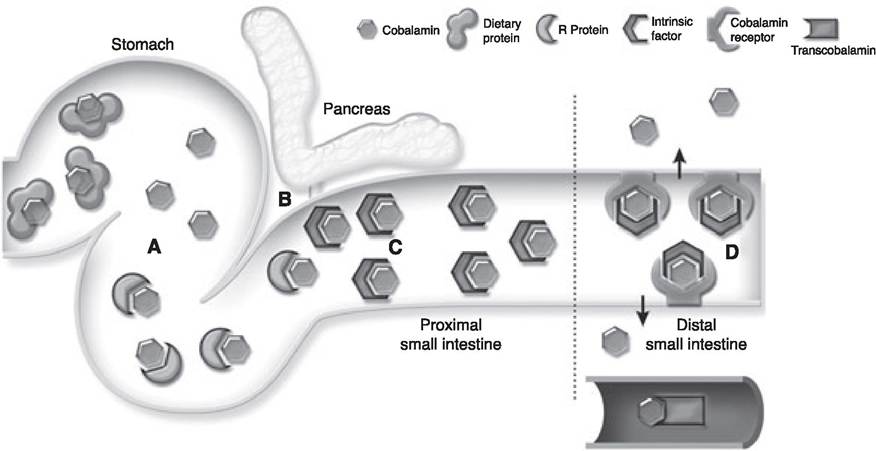
Figure 1.42:
Cobalamin absorption. Dietary cobalamin is bound to dietary protein. In the stomach, pepsin and hydrochloric acid degrade the dietary protein, releasing the cobalamin (A). The cobalamin is immediately bound by R-protein, which is produced in the gastric mucosa. In the duodenum, pancreatic proteinases digest the R-protein, releasing the cobalamin. Free cobalamin in the duodenum is bound by intrinsic factor (B). In dogs and human beings, intrinsic factor is produced by both the stomach and the pancreas, but in the cat 99% of intrinsic factor is synthesized by the exocrine pancreas. Cobalamin remains bound to intrinsic factor during its passage through the cranial small intestine (C). In the distal small intestine, the cobalamin / intrinsic factor complexes are taken up by specific receptors found only on enterocytes in the ileum (D).
These enterocytes process the cobalamin / intrinsic factor complex and release cobalamin into the circulation, where a final set of binding proteins (transcobalamins) complex the vitamin and carry it to the cells. Reprinted from Clinical Techniques in Small Animal Practice, 18(4): Suchodolski and Steiner, “Laboratory assessment of gastrointestinal function” page 207, © 2003, with permission from Elsevier.The final site of cobalamin absorption, in all species studied to date, is the ileum. Highly specialized cobalamin-intrinsic factor complex receptors are expressed on ileal mucosal enterocytes. Cobalamin that is not in complex with intrinsic factor is not readily absorbed, even if given orally in high doses.
As the exocrine pancreas is the only source of intrinsic factor in cats and an important source for intrinsic factor in dogs, exocrine pancreatic insufficiency is commonly associated with cobalamin deficiency in dogs and especially cats, and should be ruled out in patients with gastrointestinal signs and a decreased serum cobalamin concentration (see 1.4.4).5
Two other major mechanisms can reduce cobalamin availability from the small intestine, decreased mucosal absorptive capacity or excess utilization of cobalamin by the intestinal microflora. Some bacterial species commonly present in the intestinal tract, particularly some members of the Clostridium and Bacteroides genera, are able to absorb and utilize cobalamin after it has been complexed with intrinsic factor. In the normal individual with a healthy intestinal microflora, there is sufficient cobalamin in the diet to supply the needs of both the host organism and the intestinal microflora. If the numbers of bacteria present in the intestine are increased, and particularly if Clostridium and Bacteroides spp. numbers are increased in the cranial part of the small intestine, the intestinal flora can effectively compete with the host for the available cobalamin, ultimately leading to a reduced serum cobalamin concentration in the host.
Mucosal disease in the ileum reduces expression of the cobalamin-intrinsic-factor complex receptor. With reduced expression of this receptor, mucosal uptake of cobalamin in the ileum is reduced, leading to cobalamin malabsorption, depletion of body stores of cobalamin, and ultimately a reduced serum cobalamin concentration. The same is true for diffuse intestinal disease as long as the ileum is involved in the disease process. Cobalamin normally undergoes enterohepatic circulation. In gastrointestinal disease the ability of the intestine to reabsorb cobalamin secreted in the bile is reduced, which can lead to dramatic shortening of the half-life of cobalamin in circulation, particularly in cats.6
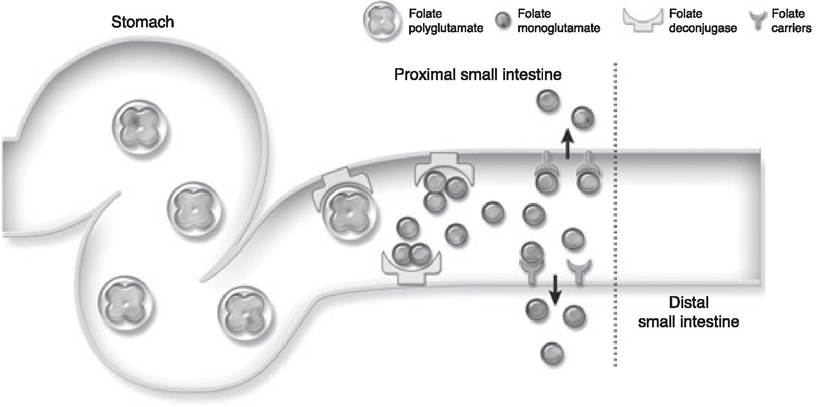
Figure 1.43:
Folate absorption. Dietary folate enters the gastrointestinal tract predominantly in the polyglutamate form. Folate deconjugase, a brush border enzyme in the cranial small intestine, deconjugates the folate polyglutamate to folate monoglutamate. Specific folate carriers present on enterocytes located in the cranial small intestine subsequently absorb folate monoglutamate. Both the deconjugase and folate carrier molecules are restricted to the cranial small intestine. There is no appreciable absorption of folate in the distal small intestine or the colon. Reprinted from Clinical Techniques in Small Animal Practice, 18(4): Suchodolski and Steiner, “Laboratory assessment of gastrointestinal function” page 208, © 2003, with permission from Elsevier.
Serum cobalamin concentration is not only of diagnostic importance. Cobalamin is essential for many cell functions and cobalamin deficiency can lead to gastrointestinal abnormalities, such as inflammatory infiltration of the mucosa, villous atrophy, and cobalamin malabsorption, as well as systemic abnormalities, such as peripheral and central neuropathies, or immunodeficiencies. Thus, patients with cobalamin deficiency may not respond to therapy of the primary disease process unless supplemented with cobalamin, and measurement of serum cobalamin is crucial in planning a rational therapy for these patients.
The normal mechanism of folate absorption is illustrated in Figure 1.43. Most folate in the diet is present in a poorly absorbable, polyglutamate form. Folate deconjugase in the jejunum removes most of the glutamate residues, leaving folate monoglutamate. Specific folate carriers in the upper small intestine then absorb folate monoglutamate.
Gastrointestinal disease may either increase or decrease serum folate concentrations, depending upon the type of pathology present. Mucosal disease in the upper small intestine or diffuse intestinal disease involving the upper small intestine may reduce folate absorption either by interfering with folate polyglutamate deconjugation or reducing the presence of folate carrier proteins. Also, many intestinal bacteria, particularly those present in the lower bowel, are able to synthesize folate. These organisms release excess folate into the intestine. Thus, overgrowth of bacteria in the small intestine can lead to increased serum folate concentrations.7
Measurement of serum concentrations of cobalamin and folate is clinically indicated during the assessment of any patient with chronic diarrhea, particularly in those with clinical signs and history suggestive of small intestinal disease. Differential diagnoses to be considered with altered serum cobalamin and folate concentrations are summarized in Table 1.8. In order to rule out exocrine pancreatic insufficiency, concurrent measurement of serum trypsin-like immunoreactivity concentration is strongly recommended. Red blood cells have very high intracellular concentrations of folate, thus it is important to avoid hemolysis of samples for serum folate determination to reduce the chance of falsely elevated results.
Table 1.8: Interpretation of serum concentrations of cobalamin and folate in companion animals with gastrointestinal diseas
| Serum Cobalamin Elevated Normal Subnormal | |||
| Serum Folate Subnormal Normal Elevated | ■ Increased bacterial numbers in cranial small intestine ■ Consider small intestinal bacterial overgrowth | ■ Increased bacterial numbers in cranial small intestine ■ Consider small intestinal bacterial overgrowth | ■ Small intestinal bacterial overgrowth or ileal mucosal disease ■ Measure serum TLI concentration to rule out EPI |
| ■ Elevated serum cobalamin with normal serum folate has no known significance | ■ Normal serum cobalamin and folate does not rule out small intestinal disease | ■ Ileal mucosal disease ■ Measure serum TLI concentration to rule out EPI | |
| ■ Disease affecting the cranial small intestine ■ Consider IBD, lymphoma, or fungal disease | ■ Disease affecting the cranial small intestine ■ Consider IBD, lymphoma, or fungal disease | ■ Diffuse mucosal disease ■ Consider IBD, lymphoma, or fungal disease | |
1.4.2.3 Assessment of gastrointestinal protein loss
Many small intestinal diseases can lead to loss of protein into the gastrointestinal tract. Examples include inflammatory bowel disease, infiltrative diseases of the mucosa/submucosa, such as lymphoma, and lymphatic drainage abnormalities (lymphangiectasia). Protein loss into the intestine is a significant metabolic drain on the patient, and may alter bacterial numbers in the intestine by increasing available substrates for bacterial growth. Excess protein loss into the small intestine can lead to loss of plasma oncotic pressure and systemic pathology such as ascites, thoracic effusion, and edema.
Assessment of protein loss into the small intestine is complicated by the digestive function of the intestine and the presence of bacterial proteolytic enzymes. It is important to be able to quantify the loss of albumin into the GI tract, as albumin is a major contributor to the colloid oncotic pressure of the plasma. Unfortunately, albumin present in the gastrointestinal tract is rapidly degraded by the animal’s own digestive proteases as well as bacterial proteases; therefore, it is not possible to accurately measure albumin in feces or intestinal fluid.
The traditional, gold-standard method for assessing gastrointestinal albumin loss is the 51Cr-EDTA test.8 Radioactive chromium bound to EDTA is administered parenterally to the patient, and subsequently binds to circulating plasma proteins, predominantly albumin. By collection of all fecal matter passed over 72 hours, and measurement of the accumulated radioactivity passed in the feces, the total intestinal protein loss can be measured. This technique is methodologically complex, requires consideration of radiation safety and the handling of radioactive waste, and is expensive. Consequently, this test is usually only used in institutional or research settings.
Alpha1-proteinase inhibitor (α1-PI) is a serum protein that is similar in molecular mass and size to albumin, and thus is lost into the intestine at a similar rate to albumin. As it is a proteinase inhibitor, it is able to resist proteolytic degradation in the intestine and is passed undamaged in the feces.9 Following extraction from fecal samples, α1-PI can be measured by use of an enzyme-linked immunosorbent assay. Species-specific assays for the measurement of α1-PI are avaible for both dogs and cats (www.cvm.tamu.edu/gilab).
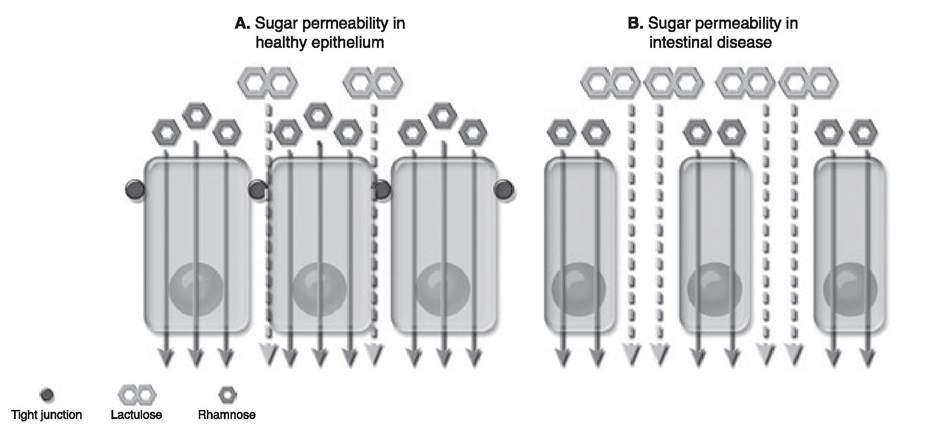
Figure 1.44:
Lactulose / rhamnose permeability testing. (A) Normal gastrointestinal mucosa has limited permeability to lactulose through tight-junction-associated paracellular channels, while rhamnose is taken up via a transcellular route. With gastrointestinal disease (B), the surface area of the mucosa available for rhamnose permeability is reduced and the integrity of the paracellular tight junctions is altered. The result is increased permeability to lactulose with a decreased permeability to rhamnose, leading to an increase in the L/R ratio in serum or urine. Reprinted from Clinical Techniques in Small Animal Practice, 18(4): Suchodolski and Steiner, “Laboratory assessment of gastrointestinal function” page 204, © 2003, with permission from Elsevier.
Ideally the loss of α1-PI should be measured over 24 hours by collection of all feces, followed by thorough homogenization and extraction. However, this is not feasible under practice conditions. Thus the current recommendation is to collect three samples of 1 g each from three different bowel movements. It is important to keep the samples frozen from the time of collection until they are delivered to the laboratory. The average and maximum concentrations of fecal α1-PI measured from the three samples are determined. At the time of writing, the presence of an average α1-PI concentration ≥9.4 μg∕g feces, or in any one sample ≥15 μg∕g is considered suggestive of a protein-losing gastroenteropathy in the dog. The fecal α1-PI test can detect significant protein loss before serum/plasma proteins are markedly reduced and before the onset of severe clinical signs related to hypoproteinemia. For example, Soft-coated Wheaten Terriers that have a familial PLE / PLN have increased fecal α1-PI concentrations long before any clinical signs are present. Also, some patients with PLE may not show signs of gastrointestinal disease and measurement of fecal α1-PI concentrations may help to diagnose the presence of gastrointestinal disease in these patients.
1.4.2.4 Assessment of intestinal absorptive capacity and barrier function
Recently, the use of sugar probes to measure intestinal mucosal permeability and absorptive capacity has been described in dogs and cats. The most common probes used for this type of study are mixtures of simple sugars, with quantification of either urinary or serum recoveries of these sugar probes.10-12
Measurement of the relative recoveries of the sugars lactulose and rhamnose can be used to assess the permeability of the small intestine. This technique has been described in both the dog and the cat.10-12 Rhamnose is believed to be absorbed across the intestinal epithelium via a transcellular route, entering via small pores on the mucosal cell surface (Figure 1.44). Lactulose, a larger molecule, is unable to penetrate these small transcellular pores. Small quantities of lactulose are absorbed through paracellular pores that are apparently located in the area of the intercellular tight junctions (Figure 1.44). Absorption and recovery of lactulose and rhamnose can be expressed as a lactulose / rhamnose (L/R) ratio. When the mucosa is di-
seased, there is usually a reduction in the surface area of the mucosa (thus less transcellular pores are available) and an increase in the permeability of the tight junctions (Figure 1.44). Thus, with diseases of the gastrointestinal mucosa, the L/R ratio is increased.
Mucosal absorptive function can be measured by measuring the uptake of sugars that are absorbed through carrier-mediated mechanisms. Xylose and 3-O-methylglucose have been used to evaluate the intestinal absorptive capacity for fructose and glucose, respectively.12 Absorptive capacity can be assessed for xylose and 3-O-methylglucose separately or can be expressed as the X/M ratio.
Currently, gastrointestinal permeability and mucosal function testing ideally requires the collection of all the urine produced over a 6-hour period in order to determine the urinary recovery of each sugar marker. Alternatively, a spot urine sample 4 to 6 hours after sugar administration can be utilized to calculate urinary sugar recovery ratios. A serum test, utilizing the ratios of serum sugar concentrations at a single time point is currently under development.
O Key Facts
■ Non-invasive serum and urine tests often yield clinically useful information for assessment of the small intestine.
■ Functional assessment of the intestine may reveal disease when histopathology is normal.
■ Serum concentrations of cobalamin and folate can aid in localization of intestinal disease, and may indicate the presence of an altered intestinal flora.
■ Fecal concentrations of alpha1-proteinase inhibitor (α1-PI) are often elevated in animals with protein-losing enteropathy before hypoproteinemia develops.
References
1. Willard MD, Jergens AE, Duncan RB et al. Interobserver variation among histopathologic evaluations of intestinal tissues from dogs and cats. J Am Vet Med Assoc 2002; 220: 1177—1182.
2. Batt RM, Horadagoda NU, McLean L et al. Identification and characterization of a pancreatic intrinsic factor in the dog. AmerJ Physiol 1989; 256: G517-G523.
3. Fyfe JC. Feline intrinsic factor (IF) is pancreatic in origin and mediates ileal cobalamin (CBL) absorption. J Vet Intern Med 1993; 7: 133 (abstract).
4. Ruaux CG, Steiner JM, Williams DA. Metabolism of amino acids in cats with severe cobalamin deficiency. AmerJ Vet Res 2001; 62: 1852— 1858.
5. Steiner JM, Williams DA. Feline exocrine pancreatic disorders. Vet Clin North Amer 1999; 29: 551-575.
6. Simpson KW Fyfe J, Cornetta A et al. Subnormal concentrations of serum cobalamin (Vitamin B12) in cats with gastrointestinal disease. J Vet Intern Med 2001; 15: 26-32.
7. Batt RM, Needham JR, Carter MW. Bacterial overgrowth associated with a naturally occurring enteropathy in the German Shepherd dog. ResVet Sci 1983; 35: 42-46.
8. Hall EJ, Batt RM, Brown A. Assessment of canine intestinal permeability, using 51Cr-labeled ethylenediaminetetraacetate. AmerJ Vet Res 1989; 50: 2069-2074.
9. Melgarejo T, Williams DA, Asem EK. Enzyme-linked immunosorbent assay for canine «1-protease inhibitor. AmerJ Vet Res 1998; 59: 127-130.
10. Rutgers HC, Batt RM, Proud FJ et al. Intestinal permeability and function in dogs with small intestinal bacterial overgrowth. J Small Anim Pract 1996; 37: 428-434.
11. Papasouliotis K, Gruffydd-Jones TJ, Sparkes AH et al. Lactulose and mannitol as probe markers for in vivo assessment of passive intestinal permeability in healthy cats. Amer J Vet Res 1993; 54: 840844.
12. Steiner JM, Williams DA, Moeller EM. Kinetics of urinary recovery of five sugars after orogastric administration in healthy dogs. AmerJ Vet Res 2002; 63: 845-848.
1.4.3