MANAGEMENT OF SPECIFIC ACUTE SMALL INTESTINAL DISEASES
Acute Viral Enteritis
General Considerations. The viral causes of acute small intestinal disease in dogs include parvoviruses 1 and 2, canine distemper virus, coronavirus, astrovirus, and rotavirus (see Box 6-2).
Disease due to coronavirus, astrovirus, and rotavirus infection is rare. The disease caused by parvovirus in dogs (destruction of intestinal crypt epithelium, lymphocyte depletion, neutropenia) is much more severe that that caused by coronavirus (destruction of tips of intestinal villi). The severity of disease associated with parvovirus infection of dogs is subjectively greater in some breeds, such as Doberman pinschers, rottweilers, and pit bull terriers. These breeds may have an inherited immunodeficiency, but this has not been proved conclusively to date. Coronavirus is generally associated with disease only in very young puppies.In cats, panleukopenia virus and enteric coronavirus are the two most common viral causes of intestinal disease. However, the panleukopenia-like syndrome associated with feline leukemia virus (FeLV) and feline immunodeficiency virus (FIV) enteritis cause acute diarrhea in some cats. Feline panleukopenia is caused by a parvovirus closely related to canine parvovirus, and the intestinal lesions are similar. In contrast to dogs, many parvovirus-infected cats have vomiting without diarrhea.
Clinical outcome following exposure to parvoviruses depends largely on the degree of prior maternal immunity, virus strain, host immune responses, and infecting dose of virus. Onset of signs is usually within 3 to 5 days of exposure. Small intestinal disease results from intestinal mucosal injury that induces a combination of secretory and malabsorptive diarrhea. Sepsis occurs commonly in both dogs and cats with parvoviral enteritis as a result of absorption of preformed bacterial toxins, as well as intact bacteria, across the damaged intestinal epithelium.
Bacteremia is more likely to occur in severely leukopenic patients.Diagnosis. Acute onset of vomiting, fever, diarrhea (often bloody), and leukopenia (variable finding) in a previously unvaccinated dog is consistent with parvovirus infection. Parvovirus antigen can be detected in feces by enzyme-linked immunosorbent assay (ELISA),[****] but results can be falsely negative based on timing of the infection or can be falsely positive due to modified live vaccine administration. Coronavirus usually induces milder disease, and leukopenia, if present, is generally less severe than in parvovirus infection. Diagnosis of viral enteritis from organisms other than parvovirus can be confirmed by fecal electron microscopy.
Feline panleukopenia is tentatively diagnosed in a young, previously unvaccinated cat with initial acute onset of vomiting and fever that progresses to bloody diarrhea and leukopenia (especially neutropenia) within 24 to 48 hours. Diagnosis is confirmed by fecal electron microscopy or paired serology. A primary differential diagnosis for dogs and cats exhibiting findings consistent with parvoviral infection is salmonellosis.
Treatment. Fluid losses, potassium deficits, and hypoglycemia should be corrected as described. In patients with signs of advanced sepsis, short-term administration of a glucose-insulin-potassium mixture (3 g glucose/1 unit regular insulin/0.5 mEq potassium chloride/kg, to be infused over 4 to 5 hours) may be warranted. If possible, once-daily measurement of serum electrolyte concentrations and blood glucose monitoring at least twice daily are recommended while the patient remains critically ill. Both food and water are withheld for at least the first 48 to 72 hours of treatment and are usually not reinstituted until vomiting and diarrhea have subsided. Small amounts of water (or water plus electrolytes) are offered first over a 24-hour period and, if well tolerated, are followed by small meals of solid, easily digestible, bland food over the next several days.
Broad-spectrum antibiotics are indicated for treatment of dogs and cats with severe gastroenteritis (especially those with hemorrhagic diarrhea), particularly if clinical findings consistent with sepsis are detected. However, routine use of antimicrobial therapy in all patients with acute viral enteritis is not indicated, because many with milder disease can be effectively managed without antibiotics, thus avoiding the unnecessary expense and risk their use entails. Studies have shown that bacteremia is most likely to occur in patients with enteritis and concurrent severe leukopenia, and it is these patients that are most likely to benefit from antimicrobial therapy. Bacteremia occurs uncommonly in patients with acute enteritis and normal white blood cell counts.
The GI tract has a rich normal flora, and so broad-spectrum coverage is necessary to cover for both aerobic bacteria (especially E. coli) and facultative anaerobic bacteria (especially Bacteroides and Clostridium). Adequate coverage for both types of bacteria can usually be attained by administration of a penicillin or first-generation cephalosporin parenterally. Addition of an aminoglycoside or quinolone is indicated for treatment of severely septic patients. Maintenance of normal blood volume is essential when using aminoglycoside antibiotics, and patients should be monitored carefully by means of a daily urinalysis for signs of possible aminoglycoside-induced nephrotoxicity. Once- daily aminoglycoside protocols should be used, and this drug class should not be administered until hypovolemia and hypokalemia have been resolved. Development of proteinuria or urine casts is often the first warning of renal injury; aminoglycoside treatment should be discontinued at this point. Cefoxitin, a second-generation cephalosporin, provides single-agent broad-spectrum coverage for patients with severe sepsis and avoids the potential toxicity of aminoglycocides. In general, antibiotic treatment is administered for short periods of time (usually until the white blood cell count returns to normal); follow-up treatment with orally administered antibiotics is not indicated.
Leukocyte rebound is a favorable sign and usually indicates that the patient will recover.Flunixin meglumine (Banamine) has been shown experimentally to increase survival of dogs after endotoxin administration and has been recommended for treatment of dogs with sepsis due to parvoviral enteritis. Because of potential for gastric injury, only a single dose for emergency management of sepsis in dogs should be used.
In some parvovirus patients with severe leukopenia, recombinant granulocyte colonystimulating factor (Neupogen) has been shown to be effective in increasing white blood cell counts. However, use of these products has not correlated to increased survival or decreased morbidity. Thus granulocyte colony-stimulating factor may not be indicated for treatment of parvoviral enteritis.
Passive immunotherapy with serum or plasma from hyperimmune dogs or cats may lessen the morbidity of acute viral enteritis, especially parvovirus. Administration of antiparvovirus antibody in this fashion may lessen viremia. Use of fresh plasma has the added advantage of potentiating opsonization of bacteria by fibronectin. On day 1 of hospitalization, 0.5 ml/lb of hyperimmune serum or plasma should be given intravenously, subcutaneously, or intramuscularly. Vaccinated blood donor animals or survivors of parvovirus infection are excellent donors. Red blood cells should not be administered unless needed.
Hypoproteinemia often develops rapidly in patients with severe diarrhea and serious small intestinal injury. As a consequence, plasma oncotic pressure drops and fluid losses via the bowel are accelerated. Plasma or hetastarch should be used to help restore normal oncotic pressure (see Table 6-1). Plasma has the advantage of supplying passive immunotherapy. Sufficient plasma is administered to increase total protein concentration to at least the low-normal range. An in-line filter is used to remove particulate material during plasma infusion.
Sequelae. Intestinal intussusception is the most serious sequela that may develop during treatment for viral gastroenteritis.
Altered intestinal motility is implicated. Careful abdominal palpation for the presence of an abdominal mass should be performed daily. Persistent vomiting after apparent clinical recovery should prompt a careful search for intussusception. Abdominal radiographs, ultrasound, or contrast studies may be necessary to diagnose intussusception. Other potential complications include bacterial embolization and metastatic abscessation (joints, subcutis, kidney) and intravenous catheter infection. Catheters should be maintained in a sterile manner under a bandage that completely covers the catheter, and catheters should be rotated to a different vein every 72 hours (up to 5 days for jugular catheters).Gastrointestinal Parasitism
General Considerations. Parasitism is common in dogs and cats, and, depending on the parasite, can occur regardless of age, breed, or sex. Although outdoor animals are more likely to be parasitized than indoor animals, indoor animals can be exposed to some parasites from transmission by transport hosts such as rodents, flies, and cockroaches. Predominant clinical signs of disease vary by the parasite (see Box 6-2), but most can induce vomiting and diarrhea.
The most common helminth parasites causing GI tract disease in dogs and cats are listed in Box 6-2. Toxocara spp., Toxascaris leonina, Ollulanus tri- cuspis, and Physaloptera are generally found in the upper GI tract and are commonly associated with vomiting. The hookworms Ancylostoma spp. and Uncinaria stenocephala are found in the intestines and cause diarrhea and significant blood loss, particularly in small dogs or cats. Trichuris spp. live in the large intestine and cecum and can result in large bowel diarrhea. Dipylidium caninum, Taenia spp., and Echinococcus spp. are the most common cestodes that infect small animals. Dogs and cats are infected with D. caninum after ingesting infected fleas and with Taenia spp. and Echinococcus spp. by carnivorism. Clinical signs are minimal but may include failure to thrive.
The most common protozoal agents potentially causing GI tract disease in dogs and cats are Giardia spp., Cryptosporidium spp., Isospora spp., and Pentatrichomonas (see Box 6-2). Giardiasis and cryptosporidiosis most commonly induce small bowel diarrhea; Isospora spp. and P hominis are most commonly associated with mixed or large bowel diarrhea. Isospora spp. infection usually causes disease only in puppies and kittens. Only cats complete the coccidian life cycle of T. gondii; oocysts in dog feces are from the ingestion of cat feces. This parasite rarely induces diarrhea and is only associated with the short-term oocyst shedding period (generally less than 14 days).
Diagnosis. All dogs and cats with acute vomiting or diarrhea should be evaluated for parasites (see diagnosis section). Diagnosis of helminth infections is based on demonstration of ova after fecal flotation. Ova detection can be used to document cestode infection, but proglottid detection occurs most commonly (D. caninum and Taenia spp.). Trophozoites of protozoans are best demonstrated by wet mounts performed on fresh feces. For parasites that are commonly occult, such as Trichuris vulpis, Giardia, and Cryptosporidium spp., performance of multiple fecal evaluations improves sensitivity. Physaloptera and Ollulanus rarely shed eggs in feces and frequently are diagnosed only by endoscopy or therapeutic trials. Giardia can be found in duodenal aspirates of dogs but lives in the distal small intestine of cats. Antigen ELISA is being assessed as a diagnostic aid for giardiasis and cryptosporidiosis (see diagnosis section).
Treatment. There are multiple antiparasite drugs that can be effective (Table 6-2). Anthelmintics such as pyrantel pamoate should be routinely administered to all puppies and kittens on initial examination and again 2 to 3 weeks later because of zoonotic health risks. In heartworm endemic areas, use of preventatives that also control helminths is indicated. Because T. vulpis infection is commonly occult, all dogs with large bowel diarrhea with no obvious cause should be given fenbendazole or other anthelmintic with activity against T. vulpis. Praziquantel is one drug with activity against the three major canine tapeworms. Fenbendazole can be effective for the treatment of Taenia spp. infection. Entamoeba, Giardia, Balantidium, and Pentatrichomonas generally respond clinically to metronidazole, but Pentatrichomonas and Giardia may not be cleared from the GI tract. Fenbendazole, albendazole, paromomycin, and febantel-pyrantel-praziquantel (dogs) are alternate anti-Giardia drugs. If Giardia infection alone is suspected, fenbendazole is superior to metronidazole. Albendazole has been associated with neutropenia in dogs and cats, and so fenbendazole appears to be safer. Addition of insoluble fiber to the diet may aid in the control of giardiasis. Sequential administration of clindamycin followed by tylosin blocked oocyst shedding and resolved diarrhea in one cat with chronic, clinical cryptosporidiosis. Tylosin alone was apparently successful in blocking
TABLE 6-2
Drugs Commonly Used in the Management of Parasitic Diseases Associated With Acute Gastrointestinal Disease
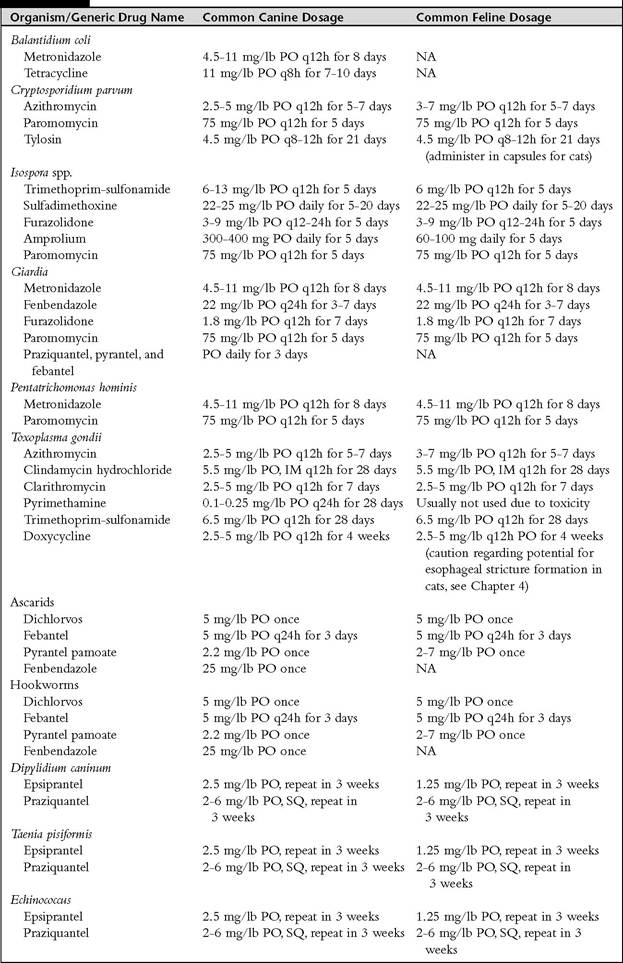
PO, Orally; NA, not applicable; IM, intramuscularly; SQ, subcutaneously.
oocyst shedding in 12 other dogs or cats with diarrhea. Paromomycin,[††††] an orally administered aminoglycoside, has effect against Pentatrichomonas, Cryptosporidium, and Giardia but has been associated with acute renal failure in cats with hemorrhagic diarrhea. The T gondii oocyst shedding period in cats can be shortened by administration of clindamycin. Clinical signs from Isospora spp. generally respond to the administration of sulfadimethoxine; alternatives include other sulfas, clindamycin, and paromomycin. Drugs used to treat Isospora spp. are static, and so cysts may still be seen after treatment.
Sequelae. Severe blood loss anemia may occur from hookworm infestation. Some intestinal parasites such as Giardia or Cryptosporidium may be difficult to clear. In addition, chronic vomiting or diarrhea from secondary inflammatory cell infiltrates into the GI tract may occur (see other sections). Some parasitic infections are zoonotic. Visceral larva migrans can occur in humans following infection by Toxocara spp. eggs. Following human ingestion of infectious eggs, larvae penetrate the intestinal wall and migrate through the tissues, leading to eosinophilic granulomatous reactions involving the skin, lungs, central nervous system, and eyes. Ocular larva migrans most commonly involves the retina and can cause reduced vision, strabismus, uveitis, and endophthalmitis. Cutaneous larva migrans in humans can be induced with infection by all three species of hookworms infecting dogs and cats in the United States. Larvae are released from eggs passed into the environment in feces; infectious larvae infect humans by skin penetration. Larval migration results in the development of an erythematous, pruritic cutaneous tunnel. Occasionally larvae will reach the lungs and cornea. Ancylostoma caninum also causes eosinophilic enteritis in humans. Transmission of small animal cestodes to humans occurs following ingestion of the intermediate host (flea, Dipylidium) or by the ingestion of eggs (Echinococcus). Dipylidium infection is most common in children and can lead to diarrhea and pruritus ani. Following human ingestion of eggs, Echinococcus enters the portal circulation and spreads throughout the liver and other tissues, causing hydatid disease. Prevention and/or control is primarily by use of taeniacides and sanitation procedures. To lessen human risks, dogs and cats should not be allowed to hunt and flea control should be maintained. Giardia, Cryptosporidium, Entamoeba, Balantidium, and Pentatrichomonas should be considered potentially zoonotic. Not all Giardia or C. parvum isolates cross-infect other species, but this cannot be determined by microscopic examination. Cats have not been shown to be infected by Balantidium and are unlikely to give Entamoeba to people because it is rare in cats and cats are unlikely to form cysts.
Acute Bacterial Gastroenteritis General Considerations. The most commonly recognized primary bacterial pathogens of the GI tract of dogs and cats include Salmonella spp., C. jejuni, C. perfringens, Helicobacter spp., and enterotoxigenic E. coli. Each agent can cause vomiting; all but Helicobacter spp. are commonly associated with the clinical signs of large, small, or mixed bowel diarrhea. C. perfringens—assodated disease appears to be less common in cats than in dogs. Each of the bacterial infections can be associated with contaminated environments, direct contact with infected animals, or potentially ingestion of infected prey species. Salmonellosis and campy- lobacteriosis are commonly associated with ingestion of undercooked poultry products. It is also possible that each of the organisms could be carried by healthy animals only to overgrow and induce disease because of other stimuli such as stress, diet change, or antimicrobial therapy. Salmonellosis is commonly associated with poly- systemic clinical signs such as fever, as well as neutropenia, in the sepsis stage of infection. Approximately 50% of the cats with salmonellosis are seen for evaluation of fever without GI tract disease signs; the owner may report a recent history of songbird ingestion. Campylobacteriosis is most common in puppies and kittens, and the organism is less likely to cause polysystemic signs than salmonellosis. Small animals can also be infected by other potential bacterial pathogens such as Shigella and Yersinia enterocolitica but seem to be relatively resistant to disease induced by these organisms.
Diagnosis. Helicobacteriosis is diagnosed clinically by the combination of demonstration of spirochetes by cytologic or histologic studies, positive urease test results, presence of inflammation, exclusion of other causes of inflammation, and response to treatment (see Chapter 5). Presence of large numbers of neutrophils on rectal cytologic examination suggests but does not prove bacterial disease induced by Campylobacter spp., Salmonella spp., or C.perfringens enterotoxin production but is a relative indication for fecal culture (see diagnosis section). C.perfringens are large rod-form bacteria; pathogenic strains generally have an unstained spore. A positive C.perfringens culture or presence of large, spore-forming rods does not prove enterotoxin production; enterotoxin measurement in feces is available at most large commercial laboratories. Because C. perfringens enterotoxin can be detected in healthy patients, as well as those that are clinically ill, positive results cannot be used to definitely confirm a disease association. Campylobacter spp. are spirochetes but are small and so difficult to identify cytologically; definitive diagnosis is based on culture.
Treatment. Supportive care and nonspecific therapy as discussed for acute viral diseases should be given as indicated. Holding the patient off food for 24 hours may speed resolution of clinical disease. C. perfringens generally responds to treatment with ampicillin, amoxicillin, tylosin, or metronidazole. The drug of choice for campy- lobacteriosis is erythromycin; alternative drugs are tetracyclines, chloramphenicol, and potentially tylosin. Salmonellosis should be treated only parenterally because of rapid resistance that occurs following oral administration of antibiotics. Appropriate antibiotics for the treatment of salmonellosis include chloramphenicol, trimethoprimsulfonamide, and amoxicillin; quinolones are effective but should be reserved for resistant infections. Helicobacter spp. infection is usually treated with the combination of metronidazole and tetracycline or amoxicillin and metronidazole with acid reduction therapy (e.g., omeprazole, famotidine). Clarithromycin can be effective and can be used once daily in cats.
Sequelae. Chronic gastritis is associated with Helicobacter spp. infection in some cases. It is possible that some chronic diarrheas are associated with bacterial infections. There appears to be minimal zoonotic risk associated with Helicobacter infections of small animals. However, dogs and cats infected with Salmonella and Campylobacter will shed the organisms into the human environment for a period of time after acute infection. Thus feces of these patients should be handled carefully.
Acute Hemorrhagic Gastroenteritis
General Considerations. Hemorrhagic gastroenteritis (HGE) is a disease of unknown cause that occurs most often in small-breed dogs. The pathophysiology of the disease most closely resembles that of acute hemorrhagic enteritis of humans induced by certain enterotoxigenic strains of E. coli. Anaphylactic reaction to as yet undetermined toxins also has been implicated. The clinical course of the disease is frequently peracute, progressing rapidly to death if not treated aggressively and promptly. Early signs are vomiting and depression, progressing to hematemesis and copious, malodorous, bloody diarrhea, often of currant-jelly consistency. Recovery after treatment is usually equally rapid.
Diagnosis. Diagnosis is based on the presence of significant hemoconcentration (packed cell volume may approach 70% to 80%), with little to no increase in total protein concentration, in a small dog with typical clinical signs. Hypovolemia is thought to account for the increase in hematocrit, whereas gut losses of serum proteins serve to prevent a corresponding increase in serum total protein concentration.
Treatment. Early, aggressive replacement of fluid volume deficits is critical to successful management of dogs with HGE. Either normal saline or lactated Ringer's solution (9 to 18 ml/lb) is infused rapidly intravenously over 1 to 2 hours, followed by slower infusion of a sufficient volume of fluids to correct dehydration, replace ongoing losses, and provide for maintenance needs (see previous discussion of fluid therapy) over the next 24 hours. Electrolyte concentration and body weight should be monitored closely during treatment. To date, evidence has not been presented to indicate that administration of antibiotics is beneficial, although patients with evidence of severe leukopenia or presence of a left shift on complete blood count should probably receive antibiotic treatment. Antiemetic drugs may be warranted if vomiting is severe or prolonged.
Sequelae. Coagulation abnormalities, especially thrombocytopenia, may develop but are usually reversed once fluid deficits are corrected. Recovery typically occurs rapidly over 24 to 48 hours, and residual effects from HGE are rare.
Acute Gastrointestinal Disease Resulting From Ingestion of Garbage and Intoxicants
General Considerations. Development of acute GI disease after ingestion of garbage or decayed organic matter occurs commonly in dogs. In most instances illness is manifested by acute onset of vomiting, often accompanied by profuse, watery diarrhea. Animals are rarely febrile, and significant leukogram abnormalities are uncommon. Illness is thought to result either from osmotic overload with nondigestible substances or from ingestion of preformed bacterial toxins. There are multiple drugs associated with vomiting.
Diagnosis. Occasionally the toxicant ingested is known, especially if iatrogenic. Definitive diagnosis of food poisoning requires laboratory identification of the offending enterotoxin. Because this is rarely performed, most cases are presumptively diagnosed by history and physical examination findings and treated nonspecifically.
Treatment. Supportive care designed primarily to prevent dehydration is generally the mainstay of treatment for acute garbage enteritis in dogs. Food and water are withheld for 12 hours, and then only water (or water plus electrolytes) is given for the next 12 to 24 hours, depending on the course of the disease. If vomiting and/or diarrhea persist for longer than 24 hours, more serious GI disease is likely. Antidiarrheal drugs should be administered cautiously if the source of intoxication is unknown, because they may potentially worsen, by slowing elimination, disease caused by bacterial enterotoxins. Antiemetic drugs can be given by injection to control severe vomiting, provided clinical evidence of dehydration or hypovolemia is not present. Intestinal protectants (kaolin, activated charcoal) are likely to be of little benefit.
Sequelae. For most cases, clinical signs resolve quickly, without sequelae. Some intoxicants cause severe gastric ulcers (glucocorticoids, aspirin) or disease of other organ systems such as the kidneys or liver (nonsteroidal antiinflammatory agents).
Acute Small Intestinal Obstruction
General Considerations. Causes of acute mechanical small bowel obstruction in dogs and cats include bowel impaction by foreign bodies, bowel-constricting lesions (volvulus, hernias), and lesions that compress the bowel lumen (tumors). Signs are variable, depending on the location of the obstruction: proximal obstruction is more likely to cause vomiting, whereas more distal obstruction is most likely to cause diarrhea or constipation. Intussusception should be considered in any young dog with acute onset of bloody diarrhea and a firm, tubular abdominal mass. Mechanical small intestinal obstruction has several important consequences. Experimentally, 6 to 12 hours of small bowel obstruction in dogs results in distention and decreased absorption from the bowel proximal to the lesion. If obstruction persists, net secretion of sodium and water quickly ensues. These changes are thought to occur as a consequence of increased intraluminal pressure, increased portal venous and lymphatic pressures, and liberation of toxins by bacteria that rapidly proliferate in the obstructed bowel. Bacteria figure prominently in the pathogenesis of changes occurring in bowel obstruction, because mortality is greatly reduced and survival prolonged in newborn or gnotobiotic dogs with experimental intestinal obstruction. If obstruction persists, blood supply to the obstructed bowel is compromised and edema, hemorrhage, and eventually necrosis of the bowel wall develop. Intestinal mucosal permeability increases, allowing plasma proteins to leak into the bowel lumen and at the same time promoting uptake of bacteria and bacterial toxins into the portal circulation. Bacterial peritonitis frequently accompanies untreated, complicated small bowel obstruction.
Metabolic complications of prolonged small bowel obstruction include hypovolemia, hyponatremia, and hypochloridemia. Significant hypovolemia may develop rapidly in distal small bowel obstruction, because fluid is sequestered within the bowel lumen.Within 24 hours of obstruction, 50% or more of total plasma volume may be lost; additional fluid also may accumulate within the peritoneal cavity. These losses may be sufficient to precipitate hypovolemic shock. Because fluid losses are isotonic, plasma electrolyte concentrations may initially be normal. Hyponatremia may, however, become apparent when a patient drinks water in an attempt to replace volume losses. Chloride loss occurs through vomiting, although vomiting occurs in only approximately 10% of dogs with complete proximal small bowel obstruction. Mild metabolic acidosis may develop as a result of bicarbonate loss (vomiting) and renal functional impairment (hypovolemia). Outcome after correction of bowel obstruction depends largely on whether complications occur (sepsis, peritonitis, bowel perforation, and acute renal failure).
Diagnosis. Abdominal palpation and radiographic evaluation are the two primary methods of diagnosis of obstruction. Survey abdominal radiographs are obtained first, and if evidence of obstruction is observed (see Chapter 2), contrast material (e.g., liquid barium or barium-impregnated polyethylene spheres [BIPS]) may be administered to enhance visualization of possible obstructive lesions and to evaluate intestinal motility. Abdominocentesis and cytologic evaluation of any fluid obtained also may be helpful in determining whether bowel leakage and subsequent peritonitis have occurred.
Treatment. If acute small intestinal obstruction is diagnosed, immediate surgery is nearly always indicated, because delay in surgical correction of an obstructing lesion may lead to further ischemic injury and possible intestinal necrosis and perforation. Thorough abdominal exploration is done at the time of surgery, even if an obvious lesion is initially identified. If a lesion cannot be identified grossly, intestinal biopsy (at least jejunum and ileum) is warranted, because certain intestinal infectious or inflammatory diseases may induce signs that mimic intestinal obstruction. If bowel perforation with severe peritonitis has developed, delayed body wall closure with sterile open packing of the abdomen may be used to facilitate drainage. The abdomen is closed after several cycles of abdominal lavage and when the infection appears to be under control (usually 1 to 2 days). If there is any question as to bowel viability at the time of initial exploratory laparotomy, a second laparotomy 24 hours later may be indicated to better assess intestinal viability. Serosal patching of bowel segments (especially colon) that have perforated or that have undergone ischemic injury may be helpful in enhancing intestinal healing and guarding against bowel leakage.
Sequelae. Complications after intestinal surgery, although generally uncommon, include peritonitis, stricture formation, abscessation, formation of adhesions, and malabsorption syndromes following resection of large segments of small bowel.
References
Bornay-Llinares FJ et al.: Identification of Cryptosporidium felis in a cow by morphologic and molecular methods, Appl Environ Microbiol 65:1455,1999.
Cubeddu LX et al.: Efficacy of ondansetron and the role of serotonin in cisplatin-induced nausea and vomiting, N Engl J Med 322:810,1990.
Hill S et al.: Prevalence of enteric zoonoses in cats, J Am Vet Med Assoc 216:687, 2000.
Lappin MR, Calpin JP: Laboratory diagnosis of protozoal infections. In Greene CE, ed: Infectious diseases of the dog and cat, ed 2, Philadelphia, 1998, WB Saunders.
Marks SL et al.: Evaluation of methods to diagnose Clostridium perfringens-associated diarrhea in dogs, JAm Vet Med Assoc 214(3):357, 1999.
Macintire DK et al.:Treatment of dogs naturally infected with canine parvovirus with lyophilized canine IgG. ACVIM Proceedings,June 10,1999, Chicago.
Obradovich JE et al.: Evaluation of recombinant canine granulocyte colony-stimulating factor as an inducer of granulopoeisis, J Vet Intern Med 5:75, 1991.
Pieniazek NJ et al.: New Cryptosporidium genotypes in HIV-infected persons, Emerg Infect Dis 5:444,1999.
Rewerts JM et al.: Recombinant human granulocyte colony-stimulating factor for treatment of puppies with neutropenia secondary to canine parvovirus infection [see comments], JAm Vet Med Assoc 213:991, 1998.
Sargent KD et al.: Morphological and genetic characterisation of Cryptosporidium oocysts from domestic cats, Vet Parasitol 77:221, 1998.
Triolo AJ: Clinical use of hypertonic saline. ACVIM Proceedings, June 10, 1999, Chicago.