Motility disorders
Gastric emptying is a highly coordinated physiological response to the presence of food in the stomach and can be impaired during a range of different disease processes. In general, there are three separate gastric motility disorders: accelerated gastric emptying, retrograde transit, and delayed gastric emptying.
Delayed gastric emptying can be due to mechanical or functional obstruction of the pylorus. Causes of mechanical obstruction are pyloric stenosis, chronic hypertrophic pyloric gastropathy, foreign bodies, pyloric or duodenal neoplasia, chronic hypertrophic gastritis, or intra-abdominal masses causing external compression of the pylorus. Functional disorders of gastric emptying result from one or more abnormalities of gastric motility. These motility disorders are often not associated with any morphological changes. Many different diseases, such as inflammatory and infiltrative lesions, gastric ulceration, IBD, altered electrolyte concentrations, acid-base disturbances, recent abdominal surgery, diabetes mellitus, and several drugs all can affect gastric motility.52In normal monogastric animals, the pylorus serves as a sieve during the postprandial period. Liquids easily pass through the

Figure 4.15:
Radiographic view of a gastric dilation-volvulus. This figure shows a radiographic view of a 10-year-old male German Shepherd dog. The radiographic image shows a large amount of air in the gastric fundus (dorsal “bubble”) and the pyloric antrum (ventral “bubble”; “double-bubble is trouble”) with gas-filled and dilated intestinal loops.
pylorus and empty relatively rapidly from the stomach by first- order kinetics. The rate of liquid expulsion from the stomach is proportional to its volume and the greater the gastric fluid volume, the more rapidly it is expelled.
Solids are handled differently, requiring reduction to a small particle size (of a mechanical obstruction of the stomach is generally straightforward, whereas a functional obstruction, causing delayed gastric motility, may be more difficult to confirm. Several methods are available for evaluating gastric emptying (Table 4.6). Contrast radiographic techniques are the most commonly available means for diagnosing gastric motility disorders in small animals. Gastric emptying times for liquids, including barium suspension, are relatively short (about 1 hour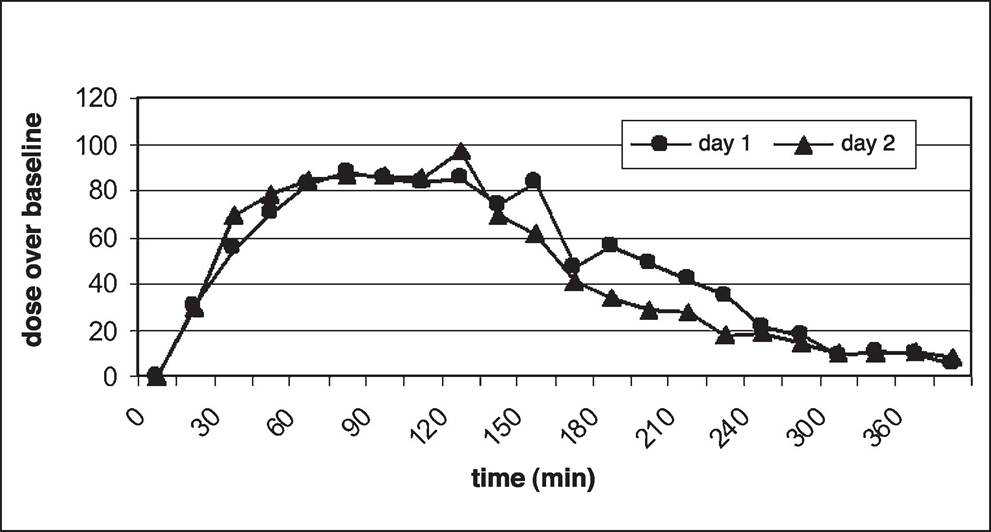
Figure 4.16:
Graph of a 13C-sodium acetate breath test in a healthy dog. The test was performed on two consecutive days in the same dog. Note the repeatability of the curve for both experiments. There is an initial plateau phase at about 90 minutes and a more-or-less linear emptying thereafter. Gastric emptying is complete after 5 hours.
in cats, up to 3 hours in dogs). Studies using barium mixed with food have shown gastric emptying times varying from 4 to 16 hours in the dog and 4 to 17 hours in the cat, depending on the composition of the food, thus making it difficult to diagnose an emptying disorder unless gastric emptying times are markedly prolonged.54 Furthermore, when solid meals are
Table 4.6: Methods for assessing gastric emptying
| Technique | Information gained | Availability in pets |
| Plain radiographs | + | +++ |
| Contrast radiographs (barium) | +++ | +++ |
| Contrast radiographs (BIPS) | ++ | +++ |
| Ultrasonography | + | ++ |
| Endoscopy | ++ | ++ |
| 13C-based tests | ++ | + - ++ |
| Scintigraphy | +++ | + (referral institutions only) |
| Computed tomography (CT) | + | + (referral institutions only) |
| Manometry | ++ | + (referral institutions only) |
BIPS = barium-impregnated polyethylene spheres
mixed with barium granules or suspension, the barium can dissociate from the food and redistribute into the liquid phase of the gastric contents.
A few years ago, barium-impregnated polyethylene spheres (BIPS) were introduced and their use for the assessment of gastric emptying in dogs and cats has been described.55 BIPS are produced in two diameters: 1.5 mm and 5 mm. The small BIPS are designed to empty with small particles, thereby mimicking solid-phase gastric emptying. Large BIPS tend to be retained in the stomach longer than small BIPS, often remaining after the test meal has passed into the duodenum and then leaving the stomach once the migrating motor complex begins. The BIPS should accumulate immediately orad to an obstructing lesion. Interpretation of gastric emptying of BIPS has some of the same limitations as that of barium studies and the use of BIPS may be more helpful in documenting a mechanical rather than a functional obstruc- tion.54Recently, ultrasonography has been used as an alternative method for assessing gastric emptying times.56 Finding more than just a small amount of fluid in the stomach 18 hours after feeding provides evidence for delayed gastric emptying in the dog. Gastric emptying can also be evaluated by means of 13C- breath or blood testing.52 The main advantages of 13C-based
tests are that no radiation is required, the tests are non-invasive and non-operator dependent, and they can be performed several times in the same subject without any biological hazard. 13C-based breath or blood tests involve the detection of an increased fraction of 13CO2 in comparison to 12CO2 after the ingestion of a labeled meal or administration of a labeled substrate. The substrate or meal is rapidly digested and absorbed at the site of interest by enzymatic or microbial digestion and the rate and appearance of the isotope in the breath or blood is a direct reflection of the GI transit of the substrate.
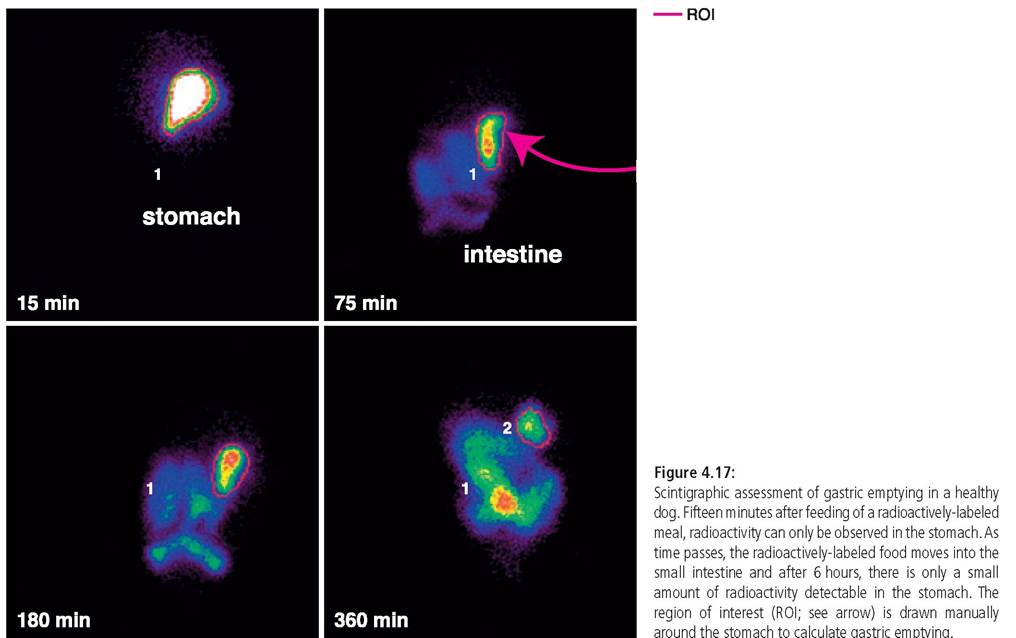
The 13C- octanoic acid breath (13C-OBT) or blood tests and the 13C- sodium acetate breath test are all based on the administration of a substrate with a functional group containing 13C. On leaving the stomach, the 13C-octanoic acid or 13C-sodium acetate is rapidly absorbed in the duodenum and metabolized in the liver. Following oxidation, the resulting 13CO2 diffuses into the blood and is excreted in the breath, either of which can be collected and measured by isotope mass spectrometry. Because gastric emptying is the rate-limiting step in the process of absorption and metabolism of the labeled substrate, the appearance of the 13C in the exhaled breath or blood is a direct reflection of the rate and pattern of gastric emptying (Figure 4.16). Finally, scintigraphy is considered the gold standard technique for assessing gastric emptying (Figure 4.17).52Patients with abnormalities of gastric motility appear normal except for intermittent postprandial vomiting. The vomitus is characteristically undigested or only partly digested, and occasionally contains mucus. It may also have an acidic pH, but bile is absent. The precise interrelationship between pyloric stenosis and pylorospasm is unclear. Signs of gastric outlet obstruction vary with the degree of obstruction. Vomiting is the predominant clinical sign and may occur at any time after a meal. The time for complete emptying of a normal meal from the stomach is 7 to 8 hours in dogs fed once daily. Vomiting of all or part of a meal at periods more than 10 hours after ingestion suggests delayed gastric emptying and the probability of a gastric, pancreatic, or proximal duodenal lesion.
Treatment
In addition to a dietary trial, prokinetic therapy is often needed. A low-fat, highly digestible blended or liquid diet fed over multiple feedings may be beneficial. Dopaminergic agonists (e.g., metoclopramide) have GI prokinetic and antiemetic properties because they inhibit peripheral and/or central dopamine receptors.
The mechanism of the prokinetic activity of metoclopramide is not entirely clear but may also be due toother pharmacological properties (e.g., 5-HT3-receptor or 5- HT4-receptor antagonism).57 Metoclopramide increases the amplitude and frequency of antral contractions, inhibits fundic receptive relaxation, and coordinates gastric, pyloric, and duodenal motility, all of which result in accelerated gastric emptying. Erythromycin, an antibiotic, has motilin-like action and at low doses increases the pressure of the gastroesophageal sphincter and accelerates gastric emptying by inducing antral contractions similar to phase III of the migrating motility complex.57 The prokinetic dose (1 mg/kg PO q 12 h) is much lower than the antimicrobial dose. Some histamine H2-recep- tor antagonists (e.g., ranitidine and nizatidine) also have acetylcholinesterase-inhibiting properties, thereby stimulating gastric emptying and small intestinal and colonic motility.
Cisapride was used to treat several GI motility disorders in dogs and cats throughout the 1990s. Because of unexplained deaths in humans, cisapride has been taken off the market and is currently only available through compounding pharmacies. There has been little clinical experience with the newer pro- kinetic agents, such as tegaserod (Zelnorm [USA], Zelmac [Europe], Novartis) and prucalopride (R093877, Janssen). Te- gaserod is a potent partial nonbenzamide agonist of 5-HT4 receptors and a weak agonist of 5-HT1d receptors with known prokinetic effects in the canine colon. In vitro studies suggest that tegaserod does not delay cardiac repolarization or prolong the QT interval of the electrocardiogram as had been occasionally reported with cisapride. Its clinical efficacy has been demonstrated in human motility disorders. Gastric and intestinal effects of tegaserod have not been reported in the dog and this drug may not prove as useful as cisapride in stimulating proximal GI motility in small animal patients.
Prucalo- pride is also a potent partial benzamide agonist of 5-HT4 receptors but has no effect on other 5-HT receptors and lacks cholinesterase enzyme activity. Unlike tegaserod, prucalopride appears to stimulate gastric emptying in the dog. Prucalopride is not commercially available at this time.The only effective treatment for pyloric hypertrophy is pyloroplasty. In some patients, the outlet obstruction may be sufficiently severe that nutritional homeostasis cannot be sustained on any kind of diet, and enteral or parenteral nutrition will become necessary.
Key Facts
■ Dolasetron and maropitant are highly efficacious as antiemetic agents.
■ A diagnosis of gastritis can only be achieved after a gastric biopsy has been analyzed histopathologically.
■ Gastric ulceration is an uncommon albeit serious complication of NSAID treatment and should be aggressively treated with sucralfate and either a histamine2-receptor antagonist or a proton pump inhibitor.
■ In dogs with gastric dilation-volvulus (GDV), aggressive intravenous fluid therapy should be initiated before the stomach is decompressed.
■ Gastric motility disorders are best diagnosed by scintigraphy or 13C-based breath or blood tests.