PANCREATITIS
From a clinical perspective pancreatitis can be broadly categorized as acute, recurrent acute, or chronic. it can be further classified according to its effect on the patient as mild or severe, nonfatal or fatal, and also by the presence of sequelae such as abscess formation.
Histologically, acute pancreatitis is characterized by findings that range from pancreatic edema to necrosis, variable infiltrates of mononuclear and polymorphonuclear cells, and local changes such as peripancreatic fat necrosis and thrombosis. Acute pancreatitis may resolve or persist and can be complicated by secondary infection and pseudocyst or abscess formation (Figure 10-1). Although it is tempting to equate mild acute pancreatitis with pancreatic edema, and severe or fatal pancreatitis with pancreatic necrosis, this relationship has not been critically examined in patients with naturally occurring pancreatitis, because the pancreas is rarely visualized or a biopsy performed in patients with mild, selflimiting pancreatitis. Chronic pancreatitis is characterized by fibrosis and low-grade mononuclear inflammation and may be a sequela of recurrent acute pancreatitis or a subclinical disease process that may present as diabetes mellitus or exocrine pancreatic insufficiency (EPi).Etiology and Pathogenesis
The etiology and pathogenesis of spontaneous pancreatitis is poorly understood. The major factors that have been implicated (by association) as causes of acute pancreatitis in the dog and cat and the experimental evidence to support their involvement are summarized in Table 10-1.
Acute pancreatitis has only recently been considered a significant disease entity in cats. it is my impression that pancreatitis in cats seems to be more chronically active and severe than in the majority of dogs. Although pancreatitis in cats has been diagnosed as the sole or predominant disease entity in cats at necropsy, it has also been variably associated with diseases in other organs, for example, the liver (cholestasis, cholangiohepatitis, hydropic change, severe lipidosis), the kidney (mild to severe nephritis), the endocrine pancreas (diabetes mellitus), the lungs (pulmonary thrombosis), and the intestine (inflammation, ulceration).
Effusions have also been noted in the pleural and peritoneal cavity. Whether these nonpancreatic abnormalities arise as
Figure 10-1
Schematic diagram of the progression of acute pancreatitis. (From Simpson KW Lamb CR: Acute pancreatitis in the dog, In Practice: J Vet Postgrad Clin Study 17:328,1995.)
| EABDED0Π Factors Associated With the Development of Acute Pancreatitis | ||
| in Dogs and Cats | ||
| Potential Etiology | Clinical | Experimental |
| Hyperlipidemia | Lipemia | High-fat diet |
| Abnormal lipid profiles Lipodystrophy | IV free fatty acids | |
| Diet | Dietary indiscretion | Fat >> protein diet |
| Obesity | Ethionine supplementation | |
| Bile reflux | Concomitant biliary disease (? cats) | Bile infusion |
| Hypercalcemia | Ca infusion | Ca infusion |
| ? Hyperparathyroidism | ||
| Corticosteroids | ? Hyperadrenocorticism | Increased CCK sensitivity |
| ? + Disk surgery? | Pancreatic duct hyperplasia | |
| Drug related | Organophosphates L-Asparaginase Azathioprine, various | Organophosphates |
| Ischemia/reperfusion | Post-GDV | Ex vivo pancreas |
| Hereditary predisposition | ? Miniature schnauzer, miniature poodle, terriers, nonsporting dogs | |
| Infectious agents | Cats: liver flukes, Toxoplasma, FIP | |
| Endocrinopathies | ? Hypothyroidism, diabetes mellitus | |
IV, Intravenous; CCK, cholecystokinin; GDV, gastric dilatation volvulus; FIP, feline infectious peritonitis.
a consequence of pancreatitis or are associated with disease processes that cause pancreatitis or are unrelated to pancreatitis is unclear at this time.
Irrespective of the initiating cause, pancreatitis is generally believed to occur when digestive enzymes are activated prematurely within the pancreas. Experimental pancreatic hyperstimulation with cholecystokinin (CCK, or its analogue, cerulein), dietary supplementation with ethionine, and obstruction of the pancreatic duct lead to the formation of large intracellular vacuoles in acinar cells.Vacuole formation is thought to be a consequence of the uncoupling of exocytosis of zymogens and abnormal intracellular trafficking of digestive and lysosomal enzymes. These subcellular alterations are considered to precipitate the intracellular activation of digestive enzymes. Edematous pancreatitis induced by CCK hyperstimulation in dogs is characterized by a rapid but self-limiting burst of trypsinogen activation. It is of note that pancreatic necrosis in humans is associated with persistent trypsinogen activation, so it may be the ability of the pancreas to limit trypsinogen activation that stops edematous pancreatitis from progressing to necrotizing pancreatitis.
Pancreatic hyperstimulation may also be of direct relevance to naturally occurring pancreatitis in dogs and cats. CCK is normally released by cells in the duodenum in response to intraluminal fat and amino acids and coordinates and stimulates pancreatic secretion and gallbladder contraction during digestion. It is possible that high-fat diets exert their effects via the excessive release of CCK and that hypercalcemia, organophosphates, and high levels of circulating glucocorticoids also facilitate or cause pancreatic hyperstimulation; however, this is not proven.
Often pancreatic inflammation is a self-limiting process, but in some patients reduced pancreatic blood flow and leukocyte and platelet migration into the inflamed pancreas may cause progression to pancreatic necrosis. Secondary infection may arise by bacterial translocation from the intestine. Release of active pancreatic enzymes and inflammatory mediators from the inflamed pancreas, such as tumor necrosis factor-α (TNF-α), interleukin-1 (IL-1), and phospholipid platelet activating factor (PAF), amplifies the severity of pancreatic inflammation and adversely affects the function of many organs (systemic inflammatory response).
Derangement in fluid, electrolyte, and acidbase balance also results (Figures 10-2 and 10-3). It is the development of multisystemic abnormalities that separates mild from severe, potentially fatal pancreatitis.Further study of the cellular mechanisms governing enzyme secretion and activation, leukocyte and platelet recruitment to the pancreas, bacterial translocation, and the development of the systemic inflammatory response in pancreatitis will hopefully provide information that will be useful in treating acute pancreatitis in the patient population in the future.
Diagnosis
There is currently no single specific test for pancreatitis in dogs and cats, and diagnosis is based on a combination of compatible clinical, clinico- pathologic, and imaging findings. Laparoscopic or surgical biopsy may be required to confirm a diagnosis and to distinguish inflammation from neoplasia.
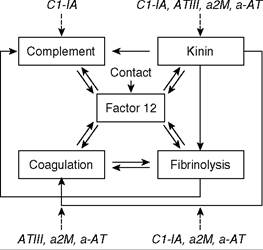
Figure 10-2 The complex interactions of the complement, kinin, fibrinolytic, and coagulation pathways following activation of factor XII by contact or trypsin. Inhibitors are shown in italics. ATIII, Antithrombin III; a2M, alpha2-macroglobulin; a-AT, alpha1-antitrypsin; C1-1A, complement fragment C1-1A. (Modified from Lasson A: Acute pancreatitis in man: a clinical and biochemical study of pathophysiology and treatment, ScandJ Gastroenterol 99:1,1984.)
Clinical Findings
Signalment and History
Dogs. Middle-age to old dogs (more than 5 years of age) that are overweight appear to be at higher risk. Miniature schnauzers, Yorkshire and Silky terriers, nonsporting breeds, and perhaps miniature poodles may be at increased risk of developing pancreatitis. There is no clear sex predisposition. Endocrinopathies such as hypothyroidism, diabetes mellitus, and hyperadrenocortic- ism may also be risk factors.The history may reveal a recent episode of dietary indiscretion or drug administration.
Common clinical signs include lethargy, anorexia, hunched stance, vomiting (with or without blood), diarrhea (with or without blood), increased respiratory rate, and enlarged abdomen. Some dogs have a history of icterus preceded by vomiting.Cats. Acute pancreatitis has been reported in cats from 4 weeks to 18 years of age. Domestic short and long hair cats are most commonly affected. Siamese cats have been overrepresented in some series. No sex bias has been demonstrated. A small number of cases have been associated with trauma, Toxoplasma gondii, pancreatic and liver flukes, feline infectious peritonitis (FIP), and lipodystrophy. Usually there are no obvious associated factors.
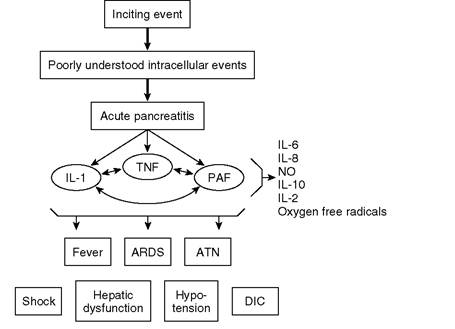
FIGURE 10-3 Inflammatory mediators in acute pancreatitis. Regardless of the inciting event (e.g., alcohol or gallstones), many poorly understood intracellular events lead to the development of acute pancreatitis.The progression of pancreatitis depends on several inflammatory mediators (interleukin [IL]-1, tumor necrosis factor [TNF], and platelet activating factor [PAF] are believed to be the most important). Other mediators (e.g., IL-6, IL-8, and nitric oxide [NO]) are produced, but they are markers of disease severity or regulatory proteins and are not mediators of disease progression. IL-1,TNF, and PAF stimulate the production of each other and mediate distant organ dysfunction such as adult respiratory distress syndrome (ARDS), hepatic dysfunction, shock, and death. DIC, disseminated intravascular coagulation; ATN, acute tubular necrosis. (From Denham W, Norman J:The potential role of therapeutic cytokine manipulation in acute pancreatitis, Surg Clin North Am 79:767,1999.)
The most common clinical findings in cats with acute pancreatitis are lethargy, anorexia, and weight loss. Vomiting, diarrhea, constipation, icterus, dehydration, ascites, and dyspnea are more variably present. Vomiting is not as prominent a sign of pancreatitis in cats as it is in dogs.
Polyuria and polydipsia have been encountered in some cats with diabetes mellitus and pancreatitis. The duration of clinical signs until presentation varies from less than 3 days to 12 weeks.Physical Examination
Dogs. Physical findings in dogs with acute pancreatitis are highly variable and range from depression, to mild dehydration with signs of abdominal pain, to acute abdominal crisis with shock (tachycardia, prolonged capillary refill time, tacky mucous membranes, hypothermia), petechiation, icterus, and ascites. An abdominal mass is palpated in some dogs.
Cats. In cats dehydration and hypothermia have been most commonly observed. Icterus may also be present. Abdominal pain is infrequently elicited. The presence of a palpable cranial abdominal mass or abdominal pain has been reported in a quarter to a third of cats in some clinical series and in cats with experimental and trauma-induced pancreatitis.
Diagnostic Approach and Differential Diagnosis
Dogs. The differential diagnosis of acute pancreatitis in dogs is usually centered around the problems of vomiting and abdominal pain (Box 10-1).
In vomiting dogs the initial approach is to distinguish self-limiting from more severe causes of vomiting on the basis of physical findings and a minimum database (e.g., packed cell volume, total protein,blood urea nitrogen [BUN; e.g.,Azostick], urinalysis, plasma concentrations of sodium and potassium). Where vomiting is associated with systemic signs of illness, or is persistent, the clinician has to differentiate metabolic, polysystemic, infectious, toxic, and neurologic causes from intraabdominal causes. This is usually achieved on the basis of combined historical and clinical findings coupled with a minimum database and the evaluation of hematology and serum chemistry profile, urinalysis, and abdominal radiography. Measurement
BOX 10-1
Differential Diagnosis of Pancreatitis in Dogs
Causes of Abdominal Pain
Gastric
Dilatation/volvulus, ulceration
Intestinal
Obstruction, intusussception, rupture, torsion, enteritis
Pancreatic
Pancreatitis
Hepatic
Acute hepatitis, ruptured bile duct, hepatic neoplasia
Splenic
Torsion, ruptured neoplasm
Urogenital
Nephritis, pyelonephritis, ruptured bladder, ureteral/urethral calculi, pyometra, prostatitis Peritoneum
Primary or secondary peritonitis (e.g., chemical: bile and urine, septic: ruptured viscus)
Pseudoabdominal Pain
Discospondylitis, prolapsed disk
Causes of Vomiting
Intraabdominal
Gastric
Gastritis, ulceration, neoplasia, outflow obstruction, foreign bodies, motility/functional disorders
Intestinal
Inflammatory bowel disease, neoplasia, foreign bodies, intussusception, torsion, rupture, bacterial overgrowth, functional disorders
Non-Gastrointestinal (Non-GI)
Pancreas: pancreatitis, pancreatic neoplasia
Liver: cholangiohepatitis, biliary obstruction
Genitourinary: pyometra, nephritis, nephrolithiasis,
Urinary: obstruction, prostatitis
Peritonitis
Metabolic/Endocrine
Uremia, hypoadrenocorticism, diabetic ketoacidosis, hepatic encephalopathy, hypercalcemia, septicemia
Drugs
Digoxin, erythromycin, chemotherapy, apomorphine, xylazine
Toxins
Strychnine, ethylene glycol, lead
Dietary
Indiscretion, intolerance, allergy
Neurologic
Vestibular disease, encephalitis, neoplasia, raised intracranial pressure
Infectious
Distemper, parvovirus, infectious canine hepatitis, leptospirosis, Salmonella
of serum amylase or lipase activity is often reported on routine serum chemistry profiles. Additional procedures such as ultrasonography, abdominal paracentesis, or pancreatic lipase immunoreactivity (PLI) assay are usually performed on the basis of these initial test results and help to distinguish pancreatitis from other intraabdominal causes of vomiting.
Where abdominal pain is the major finding, localizing abnormalities such as abdominal distention are rapidly pursued with radiography, ultrasonography, and paracentesis. Concurrently, supportive treatment is provided on the basis of physical findings and a minimum database while awaiting the results of hematology, serum chemistry profile, and urinalysis findings. Abdominal pain can arise from any intraabdominal structure. Musculoskeletal disorders such as discospondylitis and prolapsed disks can be hard to distinguish from abdominal causes of pain.
It is of note that diarrhea, which was bloody in some cases, was a more frequent sign than vomiting in dogs with experimental acute pancreatitis. Acute pancreatitis and its complications (infection, pseudocyst or abscess formation) should also be considered in the differential diagnosis of icterus and pyrexia. Some dogs with pancreatitis exhibit few localizing clinical signs. Diagnosis in these patients requires a high index of suspicion and use of versatile diagnostic tests such as ultrasonography.
Cats. In cats, lethargy, anorexia, and weight loss are the usual presenting complaints.Where encountered, localizing signs or findings such as vomiting, icterus, diarrhea, abdominal pain, abdominal mass, polyuria, or polydipsia should be pursued. Because the antemortem diagnosis of acute pancreatitis is rarely made, its overall significance as a cause of these problems is unclear at this time.
Where vomiting is present, it is approached by pursuing localizing findings such as abdominal pain or masses and by ruling out infectious, parasitic, metabolic, and gastrointestinal (GI) causes. Hyperthyroidism should be ruled out in older cats by determination of serum total thyroxine (T4) concentration. Elevated levels of hepatic enzymes, hyperbilirubinemia, hyperglycemia, and glucosuria are frequently encountered in cats with acute pancreatitis, so pancreatitis should be strongly considered in these cats.
The diagnostic approach to feline icterus is first to rule out prehepatic causes and then to pursue hepatic or posthepatic causes. The association of acute pancreatitis and hepatic lipidosis of increased mortality, cholangiohepatitis, and inflammatory bowel disease has been demonstrated in some studies. A high index of suspicion should be adopted for pancreatitis in cats with hepatic, biliary, or intestinal disease. Cats with a confirmed diagnosis of hepatic lipidosis and that have a peritoneal effusion should also be strongly suspected of having pancreatitis.
Pancreatitis may be the cause of diabetes melli- tus in some cats, but the true association between these diseases is unclear. One study suggests that cats with pancreatitis and diabetes mellitus are very sensitive to insulin. Transient euglycemia and reduced insulin requirements after removal of a pancreatic abscess suggest that pancreatic inflammation or infection can exacerbate diabetes melli- tus in cats. Transient diabetes mellitus has also been reported in a cat that was suspected of having pancreatitis.
Where a high index of suspicion for pancreatitis is present, ultrasonography and enzymology (assay of feline PLI) should initially be employed to help to detect pancreatitic inflammation. Pancreatic biopsy is required to achieve a definitive diagnosis.
Clinicopathologic Findings
Hematology
Dogs. Hematologic findings are highly variable, ranging from mild neutrophilia and slightly increased hematocrit, through marked leukocytosis with a left shift, to thrombocytopenia, anemia, and leukopenia with a degenerative left shift. If thrombocytopenia is detected, blood clotting tests (one stage prothrombin time [OSPT], activated partial thromboplastin time [APTT], fibrin degradation products [FDP or D-dimer]) are performed to determine if the patient has disseminated intravascular coagulation (DIC). Where available, the measurement of antithrombin III is useful in the early diagnosis of DIC.
Cats. A mild anemia that may be nonregen- erative and a leukocytosis that is usually not accompanied by a left shift are the most common findings in cats with pancreatitis.
Serum Biochemistry
Dogs. Serum biochemical abnormalities are variable and include azotemia (prerenal and renal), increased levels of liver enzymes (alanine aminotransferase [ALT], aspartate aminotransferase [AST], alkaline phosphatase [AP]), hyperbilirubinemia, lipemia, hyperglycemia, hypoproteinemia, hypocalcemia, metabolic acidosis, and variable alterations (usually decreased) in sodium, potassium, and chloride.
Cats. Increased levels of ALT, AP, bilirubin, cholesterol, and glucose and hypokalemia and hypocalcemia are most common. Azotemia is variably present.
Urinalysis
Urinalysis enables azotemia to be characterized as renal or prerenal. Transient proteinuria occurs in some dogs with acute pancreatitis, possibly as a consequence of pancreatic enzyme-mediated glomerular damage. The absence of white cell casts or bacteria helps to rule out pyelonephritis as a cause of abdominal pain. The presence of glu- cosuria or ketonuria should prompt consideration of diabetes mellitus.
Pancreas-Specific Enzymes
Classically elevations in serum amylase and lipase activity have been used as indicators of pancreatic inflammation in dogs. However, these tests are not very accurate because dogs with nonpancreatic disorders may have elevated enzyme activities. This may occur because both amylase and lipase are normally present in other organs and their serum activities may increase with nonpancreatic disorders, including intestinal obstruction (amylase), corticosteroid administration (lipase), and renal disease (both enzymes). Dogs with confirmed pancreatitis may also have normal amylase and lipase activity. For example, in two recent case series of dogs with histologically confirmed pancreatitis, lipase was normal in 28 dogs (61%) and amylase was normal in 31 dogs (47%). This may be due to exhaustion of enzymes, thrombosis of pancreatic vessels, the presence of inhibitors, alterations in activity, and perhaps increased clearance. In cats it seems fair to state that measuring total amylase and lipase activity is of no utility for diagnosing pancreatitis.
These limitations have stimulated the development of assays for enzymes considered pancreatic in origin. TLI is one candidate. This species-specific immunoassay measures circulating trypsinogen in healthy individuals and trypsinogen and trypsin in those with pancreatitis.
In dogs, circulating TLI is abolished by pancreatectomy and extremely low concentrations occur in EPI. Experimental and clinical studies have documented high concentrations of TLI in dogs with acute pancreatitis. TLI is therefore considered a useful indicator of pancreatic mass and potentially inflammation. Nonpancreatic diseases such as renal disease and possibly corticosteroids may increase circulating TLI. It is important to note that the utility of TLI assay for the diagnosis of spontaneous pancreatitis in dogs has not been thoroughly evaluated, and I have observed both normal and subnormal concentrations in dogs with pancreatitis.
A TLI test has also been developed for cats. Cats with EPI and some cats with spontaneous pancreatitis have abnormal concentrations of TLI. Increased application of this test indicates that high TLI concentrations may occur in the face of normal pancreatic histologic findings in cats with inflammatory bowel disease or lymphoma (Table 10-2).The reason for this is unclear. Nonpancreatic diseases such as renal disease and possibly corticosteroids may increase circulating TLI in cats.
At the present time it seems fair to conclude that the TLI assay is highly accurate for differentiating EPI from small intestinal disease. It appears less accurate in detecting pancreatitis. This is not surprising because pancreatitis is a very dynamic disease, which may influence the synthesis, secretion, elimination, and activity of circulating marker enzymes such as TLI. The tissue specificity of TLI makes it an attractive alternative to amylase and lipase activity tests in dogs, and it is presently the only useful indicator in the cat. The recent development of assays that measure pancreas specific lipase in dogs and cats (cPLI and f PLI) has yielded promising initial results in helping to diagnose pancreatic inflammation and may in time prove to be a useful diagnostic aid.
Radiography
Radiographic findings in cats and dogs with acute pancreatitis may include loss of serosal detail, increased opacity in the right cranial quadrant of the abdomen, displacement of the duodenum ventrally and/or to the right, dilated hypomotile duodenum, and caudal displacement of the transverse large intestine (see Chapter 2). Punctate calcification is occasionally identified in dogs with longstanding pancreatitis; it indicates saponification of mesenteric fat around the pancreas.
Although radiographic signs often are absent and are nonspecific, radiography remains a useful diagnostic method for pancreatitis largely because it may enable detection of other abnormalities that can cause similar signs (e.g., gastric foreign body or intestinal obstruction). Radiography is a logical first-choice imaging modality for patients with vomiting or abdominal pain. Negative or equivo-
| TABLE 10-2 | Evaluation of Pancreatic Disease in Cats With Subnormal Serum Concentrations of Cobalamin | |||
| Pancreatic Ultrasonography | Pancreatic Histopathology | |||
| Trypsin-like Immunoreactivity | Normal | Abnormal | Normal | Abnormal |
| Normal (17-49 μg∕L) | 3 | 3 | 0 | 2 |
| Increased (>49 μg∕L) | 8 | 6 | 3 | 4 |
| Decreased (occurring pancreatitis. Initial Management The initial medical management of dogs and cats with acute pancreatitis is invariably initiated before a diagnosis is confirmed and is based on the presenting clinical findings and the results of an initial database. Where dehydration or hypovolemia are encountered, these are supported with intravenous fluid therapy. Lactated Ringer's solution or 0.9% NaCl are common first choices. Potassium and glucose should be supplemented where necessary. The type of fluid should be tailored on the basis of electrolyte and pH measurements to restore normal electrolyte levels and acid-base balance. For example, dogs with a history of vomiting that are mildly dehydrated are usually given crystalloids such as lactated Ringer's solution at a rate that will provide maintenance and replace both deficits and ongoing losses over a 24-hour period. Dogs with signs of shock require more aggressive support. The volume deficit can be replaced with crystalloids at an initial rate of 30 to 45 ml/lb/hr, then tailored to maintain tissue perfusion and hydration. Plasma (10 ml/lb intravenously) or colloids (e.g., degraded gelatin or hetastarch at 5 to 10 ml/lb/day intravenously) may be indicated in the presence of hypoproteinemia or shock. Colloids such as dextran 70 and hetastarch may also have antithrombotic effects that help maintain the microcirculation. Insulin therapy is initiated in diabetic patients. Stress hyperglycemia has to be differentiated from diabetes mellitus in cats. Where vomiting is a problem, oral intake is restricted, and antiemetics (metoclopramide or chlorpromazine) and gastric acid reduction with an H2-receptor antagonist (e.g., famotidine at 0.25 mg/lb intravenously twice a day) are prescribed when vomiting is persistent or severe. Patients with persistent or severe vomiting are at risk for development of esophagitis (see Chapter 4). H2-receptor antagonist therapy will help in management of both esophageal and gastric erosive conditions. Chlorpromazine is an excellent antiemetic drug that helps provide mild sedation along with its effects of reducing nausea and vomiting. Ondansetron (Zofran) is a potent antiemetic drug that may be more effective in controlling severe and frequent vomiting in dogs and cats when chlorpromazine or metoclopramide is not considered to be effective enough. Ondansetron is administered at 0.05 mg/lb slowly intravenously two to three times a day. Prophylactic broad-spectrum antibiotics (e.g., amoxicillin with or without enrofloxacin, depending on severity) may be warranted in patients with shock, fever, diabetes mellitus, or evidence of breakdowm of the GI barrier. Analgesia is an important aspect of caring for patients with pancreatitis. It can be provided using injectable opioids such as buprenorphine (0.0023 to 0.0045 mg/lb subcutaneously every 6 to 12 hours), oxymorphone (0.023 to 0.05 mg/lb in cats, 0.05 to 0.1 mg/lb in dogs intramuscularly or subcutaneously every 1 to 3 hours), or morphine (0.05 to 0.2 mg/lb in cats subcutaneously or intramuscularly, 0.2 to 0.5 mg/lb in dogs subcutaneously or intramuscularly every 6 hours). It may be necessary to administer low-dose sedation with acepromazine (0.005 mg/lb intramuscularly) to patients that become dysphoric after opioids. It should be borne in mind that buprenorphine is a partial agonist and may antagonize the administration of more potent analgesics in patients with severe pain. A transdermal fentanyl patch (Duragesic) applied to a clipped, clean area of skin is a good way of providing a longer duration of analgesia in dogs (5 to 30 lb, 25 pg/hr patch; 30-60 lb, 50 pg/hr patch; 60 to 120 lb, 75 pg/hr; every 72 hours) and cats (25 pg/hr patch every 118 hours). Adequate fentanyl levels are not attained for between 6 and 48 hours after application (it takes somewhat longer in some dogs than in cats), so another analgesic should be administered in the short term (morphine, oxymorphone). In cats effective levels are reached by 6 to 12 hours and in some by 3 to 4 hours. It is emphasized that each patient should be treated as an individual. Careful monitoring for ongoing signs of pain is very important, and some patients will require more aggressive analgesic therapy than others. Without question, however, analgesic therapy is warranted in patients that have acute pancreatitis.Nonsteroidal analgesics are generally not used in patients with acute pancreatitis because of concerns for GI ulceration, renal failure, and potential hepatotoxicity. Steroids in Cats With Pancreatitis, and Management of Concurrent Diseases The high frequency of intercurrent hepatic and intestinal disease in cats with pancreatitis must be taken into consideration when formulating a treatment plan. Treatment with amoxicillin and metronidazole should be initiated if cholangio- hepatitis is present. Dietary support is broadly similar in hepatic lipidosis and pancreatitis, though jejunostomy tube feeding may be theoretically indicated in the latter. The principal dilemma arises in cats with pancreatitis and inflammatory bowel disease. Should corticosteroids be used? In my experience the use of corticosteroids in cats with pancreatitis and inflammatory bowel disease has enabled resolution of diarrhea and weight gain without exacerbating pancreatitis. Subnormal cobalamin concentrations are frequently present in cats with pancreatitis and GI disease, and cobalamin should be supplemented parenterally (1 mg subcutaneously every 14 days). There is a possibility of adverse effects of chemotherapeutic agents, such as methotrexate and chlorambucil, in the treatment of cats with pancreatitis and intestinal lymphoma or sclerosing cholangitis. Serum folate level should be evaluated before initiating chemotherapy and supplemental folic acid administered if indicated. Specific Therapy Once a diagnosis of pancreatitis is confirmed, potentially more specific therapy can be employed. The majority of dogs with acute pancreatitis respond to fluid therapy and nothing by mouth for 48 hours. Hence, specific therapy is usually reserved for dogs that do not respond to fluid therapy or those with signs of multiorgan system involvement or DIC. Pancreatitis in cats seems to be more chronically active and severe than in dogs; thus cats with a confirmed diagnosis of pancreatitis generally need more support than the majority of dogs. The specific treatment of pancreatitis has evolved along two lines: 1. Stopping further pancreatitis from occurring 2. Limiting the local and systemic consequences of pancreatitis Therapies aimed at inhibiting pancreatic secretion (e.g., glucagon, somatostatin) or the intracellular activation of proteases (e.g., gabexate mesilate), which have been of benefit in ameliorating the severity of experimental pancreatitis, have shown little benefit in the treatment of patients with spontaneous pancreatitis. This lack of success is probably related to the timing of therapy in relation to the development of pancreatitis. Experimental therapy is usually initiated before or shortly after the induction of pancreatitis, whereas most clinical patients are not presented until 24 to 48 hours after the onset of pancreatitis. Support for this hypothesis is provided by the efficacy of somatostatin and gabexate mesilate in reducing pancreatitis in humans undergoing elective procedures, such as endoscopic retrograde cholecystopancre- atography, that are associated with pancreatitis. The lack of success with inhibiting the progression of spontaneous pancreatitis has led to increased emphasis on damage limitation: ameliorating the effects of inflammatory mediators or pancreatic enzymes on the patient and maintaining pancreatic perfusion. Coagulation abnormalities should be pursued, and treatment with parenteral vitamin K can be assessed. If a coagulopathy (e.g., DIC) or hypoproteinemia is present, or if the patient's condition is deteriorating, fresh frozen plasma (5 to 10 ml/lb) may be beneficial in alleviating the coagulopathy and hypoproteinemia and restoring a more normal protease-antiprotease balance. The administration of heparin (35 to 70 IU/lb three times a day) may be potentially useful in ameliorating DIC, promoting adequate microcirculation in the pancreas, and clearing lipemic serum. In experimental pancreatitis, isovolemic rehydration with dextran has also been shown to promote pancreatic microcirculation in dogs. A dopamine infusion had a protective effect when administered to cats within 12 hours of induction of experimental pancreatitis. Therapy to abrogate the systemic inflammatory response with antagonists of PAF (e.g., lexipafant), IL-1, and TNF-α holds promise for the future. Oral pancreatic enzyme extracts have been reported to reduce pain in humans with chronic pancreatitis, though this is controversial. They are less likely to be effective in dogs because they do not appear to have a protease-mediated negative feedback system. Dietary Management Our ability to make precise recommendations for dietary management of acute pancreatitis is limited by the absence of controlled studies of the dietary management of this syndrome. Dogs. In dogs suspected of having acute pancreatitis, oral intake is usually withheld for the initial 48 hours and then gradually reintroduced if tolerated. The rationale for giving nothing by mouth even when vomiting is absent is to “rest the pancreas” by decreasing pancreatic stimulation. Because fats and amino acids are potent stimulators of pancreatic enzyme secretion, their effects are initially avoided by feeding a diet high in carbohydrate and then gradually increasing fat and protein content during the recovery period (the first and second weeks after the onset). Continued fat restriction is usually recommended for dogs that have had pancreatitis and is based on clinical and experimental observations that suggest an association between high-fat meals, hyperlipidemia, and a “high plane” of nutrition and pancreatitis. The protein content of the diet may also be important because dogs fed a choline-deficient ethionine- supplemented diet or a protein-restricted high-fat diet develop pancreatitis. Alternative strategies of minimizing pancreatic stimulation include total parenteral nutrition (TPN) and feeding distal to the CCK-releasing part of the intestine via a jejunostomy tube, but these options are usually reserved for dogs with persistent vomiting or severe pancreatitis. Recent studies in humans indicate that acute pancreatitis may be exacerbated by the early administration of TPN (before 5 days) and that enteral nutrition, administered via a nasojejunostomy tube, can attenuate the systemic inflammatory response and may decrease complications. Feeding tube placement is discussed in Chapter 12. Cats. In contrast to dogs, where vomiting and abdominal pain predominate, pancreatitis in cats is usually associated with anorexia and weight loss. The presence of anorexia and weight loss in cats with pancreatitis may be a significant contributing factor to their poor prognosis. Prolonged fasting (more than 3 days) to avoid pancreatic stimulation may only serve to compound malnutrition. The clinician is faced with the dilemma of having to provide nutritional support to prevent or reverse malnutrition and hepatic lipidosis and fasting the patient to prevent pancreatic stimulation. The surgical or endoscopic placement of a gastrostomy or esophagostomy tube may circumvent anorexia where vomiting is not a problem. Current dogma suggests that a diet that limits pancreatic stimulation and provides adequate nutrients should be fed. However, this ideal may be difficult to achieve because cats are physiologically adapted to diets that are high in fat and protein, and most balanced cat foods contain between 30% and 60% fat on an energy basis. I have had success when feeding commercial maintenance or intestinal diets through a gastrostomy tube. As discussed above, the endoscopic or surgical placement of a jejunostomy tube and feeding a liquid diet distal to the duodenum and TPN are other solutions to providing balanced nutrition and minimizing pancreatic secretion that may prove useful in refractory cases. Patient Monitoring Patients with suspected or confirmed pancreatitis should be carefully monitored to enable early detection of shock or other systemic abnormalities. Minimal monitoring for stable patients includes regular assessment of vital signs and fluid and electrolyte balance. In those with systemic abnormalities, monitoring should be more aggressive and may include vital signs, weight, hematocrit, total protein concentration, fluid intake and output, blood pressure (central venous and arterial), levels of electrolytes and glucose, acid-base status, platelets, and coagulation status. Monitoring amylase, lipase, or TLI on an intermittent sequential basis may also help to support resolution or progression of pancreatic inflammation. Ultrasound-guided fine-needle aspiration of the pancreas may enable infected pancreatic necrosis to be detected. Ultrasonography may also enable detection of delayed consequences of acute pancreatitis such as pancreatic abscessation, pseudocyst formation, and biliary obstruction. Surgical Intervention Surgery is potentially indicated to remove devitalized tissue in patients with infected pancreatic necrosis and to investigate and relieve persistent biliary obstruction. The removal or drainage of abscesses is another indication for surgery. Resection or surgical drainage of pancreatic pseudocysts is not always necessary because these can resolve spontaneously or following percutaneous drainage. Pancreatitis that is recurrent or is unresponsive to treatment may also require surgery to confirm a diagnosis and to exclude pancreatic cancer. Surgery has often been necessary to confirm an antemortem diagnosis of acute pancreatitis in cats. The increased application of ultrasonography and measurement of TLI has led to a reduced dependency on surgery in cats with high TLI and sonographic abnormalities. However, it should be stressed that cats with pancreatitis often have concomitant abnormalities in other organ systems (e.g., liver and intestine), and biopsy of these organs and the pancreas may be indicated to optimize diagnosis and treatment. Transient eu- glycemia and reduced insulin requirements were noted after the removal of a pancreatic abscess in one cat, suggesting that surgical intervention may be beneficial in these cases. Prognosis Dogs. The prognosis for dogs with mild acute pancreatitis is good. Severe or recurrent pancreatitis is associated with a guarded prognosis. Cats. The prognosis for acute pancreatitis in cats must always be considered guarded. Where extensive hepatic lipidosis is present or suppurative pancreatitis is diagnosed, the prognosis is poor. BOX 10-2 Potential Etiologies of Pancreatic Acinar Atrophy in Dogs Hereditary German shepherd dogs, collies, English setters Primary acinar problem Pancreatic secretory trypsin inhibitor deficiency Nutritional Selective malabsorption Vitamin or mineral deficiency (e.g., E or B^ Decreased trophic stimuli Abnormal cholecystokinin (CCK) release Immune destruction Cell-mediated, antipancreatic antibodies Apoptosis
More on the topic PANCREATITIS:
-
Veterinarian -
| ||||