Therapeutics
If the mega-colon is secondary and hypertrophic, the underlying cause should be addressed. In the case of pelvic canal stenosis of less than 6-months duration, a pelvic osteotomy is indicated (Washabau 2003; MacPhail 2002).
The primary pathogenesis of idiopathic mega-colon is smooth muscle dysfunction rather than neurological disease leading to dysmotility, which infers that therapeutics should be aimed at stimulating colonic smooth muscle contraction (Washabau and Holt 1999). However, in endstage mega-colon, fiber supplements and prokinetics are unlikely to have much benefit. Medical management comprises of shortterm resolution of the fecal impaction, which requires manual evacuation of the bowels under anesthesia using lubrication and enemas, usually after 24-hours of rehydration, and long-term management by utilizing stool softeners, prokinetics, and dietary changes. Obstipation due to mega-colon exceeding 6months should be managed with a subtotal colectomy (Washabau 2003). This technique,
Figure 18.1 Right lateral abdominal radiograph in a skeletally mature domestic shorthair cat diagnosed with idiopathic mega-colon. The colon is severely dilated and filled with fecal material. (With permission, Dr Carla Chow, Nine Lives, The Cat Hospital, Hong Kong.)
as opposed to a colectomy, is preferred as long-term cats that had the ileocolic junction preserved had improved stool consistency, it is also thought to minimize bacterial ascension (Sweet, Hardie, and Stone 1994). In hypertrophic canine mega-colon, constipation that is refractory to medical therapy for more than 2-months then subtotal colectomy, preserving the ileocecal junction, is recommended with the best long-term outcome (Nemeth et al. 2008).
The first line of treatment should employ enemas and deobstipation.
Hydration of the patient followed by a warm water or 0.9% saline (5-10 ml/kg body weight) enema, with or without a surgical lubricant, is performed in hospital over several days (MacPhail 2002). Dehydration contributes to colonic water absorption, which hardens fecal matter and should be addressed. Thereafter osmotic laxatives can be used, but emollient, lubricant, and stimulant laxatives are not indicated in mega-colon. Lactulose is a poorly absorbed carbohydrate that is hydrolyzed to a fatty acid by the colonic microflora. These metabolites exert osmotic pressure and draw fluid into the colon (Davenport, Remillard, and Carroll 2010). Cats with longstanding mega-colon are unlikely to respond to lactulose laxatives.Dietary intervention is helpful in feline constipation. Key components of the diet that need to be addressed include, water intake, fiber content, and digestibility (Davenport et al. 2010). Emphasis should be placed on providing access to fresh water in multiple locations in the pet's living environment. The inclusion of canned sweet potato and pumpkin, not only increase fiber content but also has over 90% water. Dietary fiber with low solubility, are bulk-forming laxatives, distend motility by distending the colon, and can form dry stool, an unattractive option for mega-colon. It is recommended that the diet not exceed 5% dry matter crude fiber. Soluble fiber including pectins, canned pumpkin, guar gum, and psyllium are options that are more appropriate. The intestinal bacteria, producing short-chain fatty acids, altering colonic microenvironment, will ferment some of these soluble fibers. Short-chain fatty acids are known to have a strong impact on the colonic microenvironment and serve as nutrients for the colonocytes. Psyllium enriched, and chicory pulp, fructo-and mano-oligosacharides containing, dry diets has been trialed in cats for the management of constipation (Freiche et al. 2011). Palatability was considered excellent and most cats were considered to have improved by 2 months with fecal consistency having improved considerably and the use of cisapride and lactulose decreased considerably (Freiche et al.
2011). It is generally recommended that highly digestible diet be fed to cats and dogs with mega-colon, and dividing meals will also limit the amount of ingesta reaching the large bowel (Davenport et al. 2010). In dogs, an additional intervention that can be helpful is post-prandial leash walking, as gastro-colic reflex and exercise will stimulate defecation (Davenport et al. 2010).Various prokinetics can be considered in both cats and dogs (Table 18.1). Cisapride has shown to stimulate smooth muscle contraction along the entire length of the colon (Hasler and Washabau 1997; Washabau and Sammarco 1996). Certain H2-receptor antagonists, ranitidine and nizatadine, but not cimetidine or famotidine, will also stimulate the colon along its
entire length stimulating peristalsis (Hall and Washabau 1997). The mechanism of action is acetylcholinesterase inhibition, increasing the binding of acetylcholine that can bind to smooth muscle muscarinic receptors. Motilin-like drugs including erythromycin accelerate canine colonic transit, and has been shown to stimulate canine, but not feline colonic smooth muscle in vitro (Washabau 2003). Lastly sym- pathomimetics can be considered, bethanechol a cholinomimetic binds muscarinic cholinergic receptors stimulating gastrointestinal motility (Washabau 2003). Misoprostol, a prostaglandin E1 analogue, has been shown in vitro to stimulate feline colonic smooth muscle but there are no in vivo studies (Mosenco, Meltzer, and Kennedy 2003). Medical management alone using cisapride, is estimated to be effective in 35% of cases of dogs with hypertrophic mega-colon (Prokic et al. 2010). Drugs with similar prokinetic effect include prucalopride and tegaserod (Table 18.1). Tegaserod can be administered intravenously, with equal benefit noted at the high and low end of the dose range, and it has no effect on QT interval prolongation. Prucalopride is not registered for use in the United States by the Food and Drug Administration, although approved for use in Europe and Canada.
Table 18.1 List of drugs used in megacolon in the canine and feline patient.
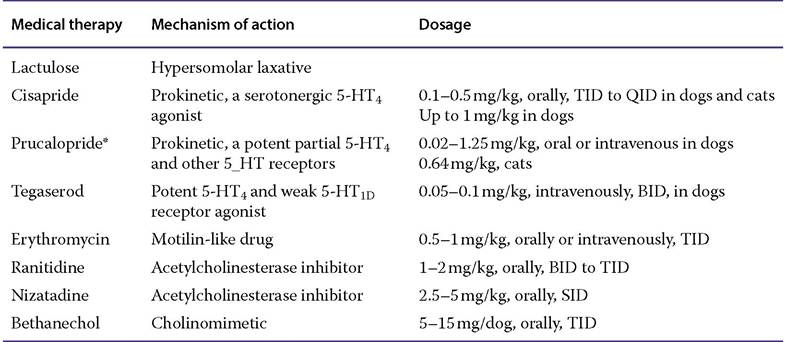
Abbreviations: BID, twice daily; QID, four times daily; SID, once daily; TID, three times daily.
* Not approved in the USA.
Source: Adapted from Washabau 2003. Reproduced with permission of Elsevier.