Therapy
Long-term administration of antibiotics (doxycycline) together with glucocorticoids (oral or topical) and/or non-steroidal antiinflammatory agents usually control the condition, but recurrence following cessation of medication is common.
Generally speaking the best response to therapy is seen in the dogs that undergo desensitization therapy (complete resolution), followed by corticosteroids and cyclosporine (marked reduction and duration of response). Doses for cortisone and cyclosporine are 1 mg/kg SID and 3-5 mg/kg SID, respectively. If the dog will tolerate a spray, intra-nasal cortisone spray would be the best for long-term treatment. In dogs where only corticosteroids are used, clinical signs are merely controlled and tend to return once the corticosteroids are discontinued. The use of antibiotics appears to be neither effective nor sustained in eliminating clinical signs but helps to reduce the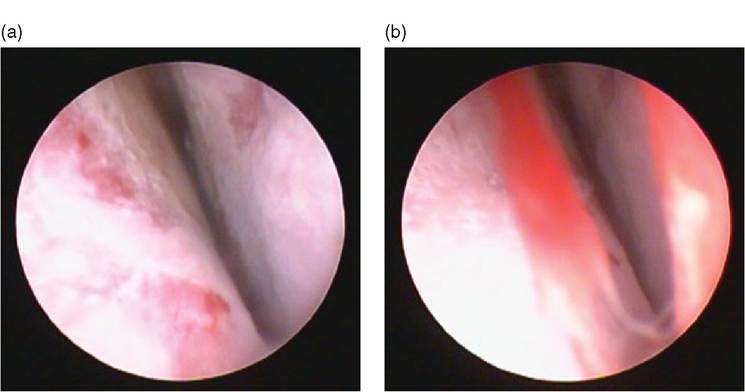
Figure 35.1(a, b) Rhinoscopy image from a dog with lymphoplasmacytic rhinitis showing hyperemic and swollen nasal mucous membranes.
nasal discharge and the type in some dogs - from a muco-purulent to serous. Thus, it is most likely that antibiotics merely reduce secondary bacterial colonization without diminishing the nasal discharge caused by idiopathic LPR (Windsor et al. 2004). In people with CRS and allergic rhinitis the use of topical corticosteroids is more beneficial than antihistamines and antibiotics for achieving symptomatic improvement both in children and adults, with systemic corticosteroids indicated in severe cases (Mori et al. 2010).
Idiopathic LPR needs to be managed with long-term corticosteroids and cyclosporine therapy if the underlying triggers are not identified and suppressed with desensitization therapy.