Treatment of Acute Heart Failure
Regardless of the cause of left heart failure with pulmonary edema, the treatment is similar. The emergency presentation of a patient in acute congestive heart failure requires prompt and appropriate investigation and treatment.
Detailed investigation may have to be delayed due to the unstable nature of the patient and treatment instituted urgently. Patients can vary in their presentation depending on the severity from mildly tachypneic to severely dyspneic, coughing up the pink froth of pulmonary edema. Initial treatment involves stabilization of the patient (Figure 5.1 and Figure 5.2). The following protocol is a guide:1) Cage rest: This reduces oxygen consumption by the tissues.
2) Oxygen supplementation: This can be delivered using an oxygen cage. If the temperature is not regulated, large dogs tend to become hyperthermic. A nasal oxygen tube, nasal prongs or flow by may also be used (Figure 5.3). In cats, a brief thoracic ultrasound is appropriate, as if a large pleural effusion is detected, it must be drained by thoracocentesis. This can be life-saving in severely dyspneic cats.
3) Diuretic: Typically a loop diuretic such as furosemide is given intravenously. This route is used as it is faster acting and the furosemide has a venodilating action. In fractious patients when catheter placement would be too stressful, an intramuscular route can be used pending control of heart failure. Doses of 2-4 mg/kg furosemide are used initially. The patient's respiratory rate should be reviewed at 30 minutes and then one hour. If the rate has not decreased, repeat the dose or consider using a continuous rate infusion of furosemide at 1 mg/kg/hr. As soon as the respiratory rate starts to fall this dose rate should be decreased or serious side effects could occur.
4) Positive inotrope: Pimobendan should be given at 0.3 mg/kg p.o.
as patients benefit from inotropic support. In Europe, an intravenous preparation is available. However, given orally, it is rapidly active.5) Monitor: Recording the respiratory rate and effort is a good guide to response. As the pulmonary edema resolves, the respiratory rate and effort should decrease. The production of a large volume of dilute urine is also a sign that the diuretics are effective. Radiographs can also be helpful, showing resolution of pulmonary edema.
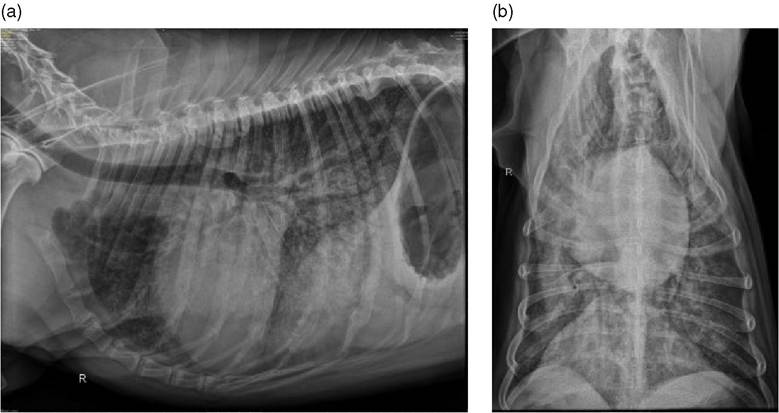
Figure 5.1 X-ray of acute pulmonary edema pre treatment. Lateral and DV radiographs of a 7 year old Doberman pinscher with dilated cardiomyopathy dog with pulmonary edema and after treatment. In Figure 5.1a, the extensive interstitial/alveolar pattern can be seen especially in the perihilar region on the lateral and in the right caudal lung field on the DV.
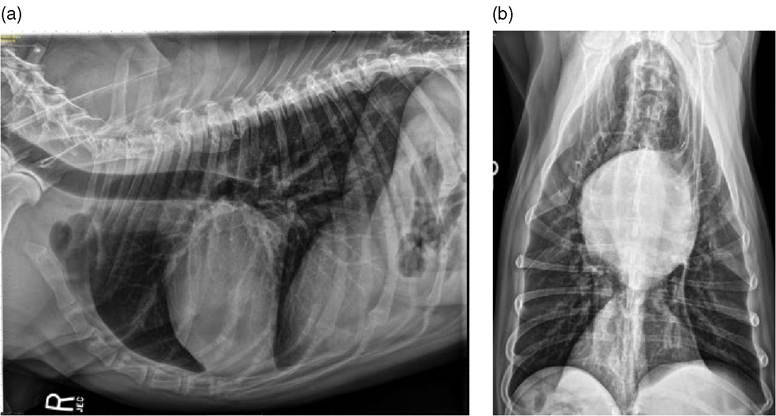
Figure 5.2 X-ray of acute pulmonary edema post treatment. After treatment with diuretics, the lung pattern has normalized and the outline of the left atrium is clearer as it is now surrounded by air. Notice the heart size is smaller.
6) Blood pressure: Assessing blood pressure may help in decision making regarding ongoing treatment options. Generally the optimum blood pressure in acute congestive heart failure is 90-100 mmHg and vasodilators can help decrease the afterload, encouraging forward flow and offloading the ventricle. Sodium nitroprusside, hydralazine, and an ACE inhibitor can help. Sodium nitroprusside is the most

Figure 5.3 A dog with acute heart failure being administered oxygen. It is important that this does not stress the dog or cat.
effective and is given as a constant rate infusion with the dose titrated to blood pressure.
Unfortunately, cost makes it prohibitive in most settings and the patient needs careful monitoring. If the blood pressure is low as in some DCM dogs, a pressor may be needed to increase pressure as well as provide inotropic support. In these cases, a constant rate infusion of dobutamine is often helpful. Venodilators such as nitroglycerine used to be recommended to decrease the preload although recent evidence suggests that they are not effective. The effect of ACE inhibitors on blood pressure is minimal with a decrease of 5-10 mmHg expected.6) Sedation: Some patients are stressed by their disease or hospitalization. Opiates can help alleviate this anxiety and reduce oxygen consumption although low doses are preferred due to their depression of the respiratory centers. Buprenorphine or butorphanol are frequently chosen.
As the patient improves, the oxygen concentration can be gradually decreased to that of room air with monitoring of the respiratory rate and the medication switched to oral drugs for discharge. Radiographs are helpful to document to resolution of the pulmonary edema.