Vascular diseases of the liver
7.4.2.1 Congenital portosystemic vascular
anomalies
Pathogenesis
Congenital portosystemic vascular anomalies or shunts (PSS) are congenital vessels that connect the portal vein and a large vein outside the splanchnic venous system; usually the vena cava or the azygos vein.4 Portosystemic shunts occur in many different dog breeds.
Cairn andYorkshire Terriers, Maltese Terriers, Dachshunds, Labrador Retrievers, Bernese Mountain dogs, Hovawarts, and Irish Wolfhounds are frequently af- fected.72 In a number of breeds, the incidence reported is between 1-5% of dogs born and it is likely that this number applies to most affected breeds.9,13-14 Small dog breeds commonly have extrahepatic shunts, while large breeds more frequently have intrahepatic shunts, but presumably they are inherited in all dog breeds. Shunts also occur in cats (see 7.6.2.1). In both dogs and cats, PSS affect both females and males.Portosystemic vascular shunts are large-diameter vessels leading to a preferential flow of portal blood through the shunt, thereby bypassing the liver. Quantitative measurements have revealed that, in most cases, >95% of the portal blood bypasses the liver. This is in part compensated for by an increased arterial blood supply to the liver. The oxygen supply for the hepatic parenchyma is therefore maintained. However, toxic compounds such as ammonia are not cleared adequately from the portal blood, which results essentially in autointoxication, in turn leading to neurological signs, as the brain is most sensitive to this autointoxication. In addition, endotoxins that are not cleared by the liver can cause vomiting. Portal blood also contains hormones and growth factors that induce the pro-
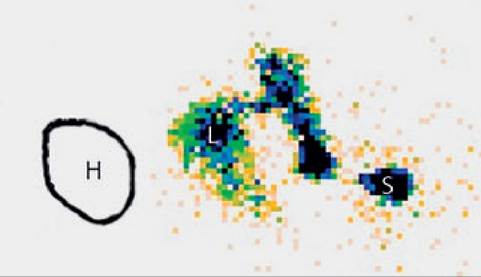
Figure 7.12:
Splenic scintigraphy - normal dog.
A small amount (2 mCi) of 99mTc was injected into the splenic pulp (S) of this dog under ultrasound guidance and the patient was imaged for a period of 4 minutes. This image is a reformatted image of the first 7 seconds of the study. The heart (H) has been drawn into the image. Note that all of the radioactivity reaches the liver (L) and none the heart (H), demonstrating normal portal blood flow. (Image courtesy of Dr. Robert C. Cole, Texas A&M University.)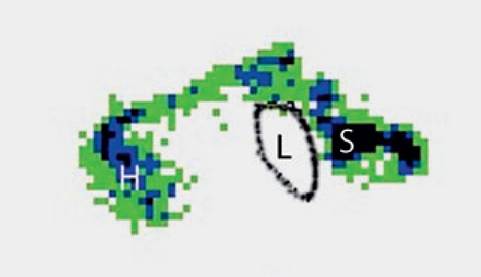
Figure 7.13:
Scintigraphy - portoazygos shunt. A small amount (2 mCi) of 99mTc was injected into the splenic pulp (S) of this dog under ultrasound guidance and the patient was imaged for a period of 4 minutes. This image is a reformatted image of the first 7 seconds of the study. The liver (L) has been drawn into the image. Note that the radioactivity bypasses the liver and appears first within the heart (H), indicating the presence of a portosystemic shunt. With this type of study, it is possible to determine whether a single shunt vessel or multiple shunt vessels are present and also whether the shunt vessel or vessels drain into the caudal vena cava or the azygos vein. In this case, a portoazygos shunt was suspected and confirmed during surgery. (Image courtesy of Dr. Robert C. Cole, Texas A&M University.)
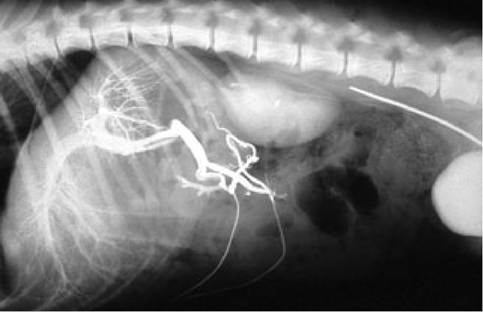
Figure 7.14:
Normal portal blood flow. This figure shows an angiography of the normal portal blood flow in a healthy dog. Note that all the dye injected through the catheter reaches the portal blood directly and evenly distributes throughout the tributaries of the portal vein.

Figure 7.15:
Portocaval shunt. This figure shows an angiogram of a dog with a congenital extrahepatic portocaval shunt.
Note that none of the dye injected reaches the liver, but instead immediately reaches the caudal vena cava. In most cases, a diagnosis of a portocaval shunt can be made by abdominal ultrasonography and scintigraphy, and angiography is usually not needed for routine clinical cases.duction of local hepatocyte growth factor (HGF), which is essential for normal hepatic growth. Impaired regulation of hepatic growth results in poor growth and development of the liver, which stays very much behind as the animal as a whole grows more or less normally. With increasing age, this discrepancy becomes more and more severe, which explains why clinical signs usually do not develop until the patient has reached an age of around 6 months. Histologically, the liver shows signs of hepatocellular atrophy and an increased number of tortuous arterioles in the portal areas. The portal vein branches are so poorly developed that they are usually not histologically distinct. Macroscopically, the portal vein and its branches cranial to the shunting vessel are very narrow.4
In many cases of PSS, the kidneys are enlarged and also hyperfunctional. The poor liver function often results in hypoalbu- minemia, which, however, is usually not low enough to cause ascites. Poorly soluble ammonium urate crystals are present in the urine in over half of the cases. These crystals can form bladder, kidney, or urethral stones. Such concrements are small, rough, yellow, and radiolucent.
Portosystemic shunts can be localized inside or outside the liver. Intrahepatic shunts usually originate from the left main branch of the portal vein (i.e., persistent ductus venosus), but in some cases they also can originate from the right branch. Intrahepatic shunts occur mostly in large breed dogs. Extrahepatic portocaval shunts are seen in toy or medium-sized breeds, and may originate from the gastroduodenal vein, the gastrosplenic vein, or the mesenteric vein. Most extrahepatic shunts in dogs end in the vena cava just cranial to the right kidney, but others terminate in the azygos or hemiazygos veins.
Because the azygos vein is much smaller than the vena cava, the flow through a porta-azygos shunt is much lower and these dogs usually have less severe clinical signs, often becoming apparent at a later age. It is not unusual to be presented with a dog with a porta-azygos shunt that is 5-7 years of age. In rare cases, the portal vein is only connected with a systemic vein, without any normal continuation to the liver cranial to the branch of the shunting vessel.Symptoms
In almost all cases, the clinical signs include apathy, excessive sleeping, and rapid fatigue. The animal may or may not be underweight, but stunted growth is rarely seen. Polydipsia occurs in many cases (> 50%), as well as occasional vomiting, and a variable appetite. Usually, there are neurologic abnormalities with HE varying between stages 1-4. The symptoms are usually periodic and days with clinical symptoms are followed by gradual improvement and a period without apparent clinical signs, lasting for one to several weeks. The neurological symptoms of HE are discussed in detail in 7.4.3. Some male patients may present with acute dysuria as ammonium urate stones may lead to urethral obstruction. Although the symptoms usually develop in patients at an age of around 6 months, some patients may develop signs as late as 10 years of age.
Diagnosis
Serum activities of hepatic enzymes and serum concentrations of albumin may or may not be in the abnormal range, but if abnormal the changes are mild. Also, patients with portosystemic shunts never develop icterus. Abdominal radiographs or ultrasound reveal a small liver and large kidneys.73,74 The measurement of plasma ammonia concentration is the first step to confirm the diagnosis, as it is highly elevated in most cases.9,16 If there are any doubts as to whether the patient has a PSS, an ammonia tolerance test can be used to confirm the diagnosis. Serum bile acids concentrations, especially postprandial ones, are also increased in most cases,75 but they have recently been reported to be less sensitive than ammonia.16 Also, serum bile acids concentrations are nonspecific.
There is usually a distinct increase of postprandial serum bile acids concentrations in both dogs and cats with PSS,75 but such increases can also be seen in patients with cholestatic diseases.16 In contrast, plasma ammonia concentration is only increased in cases of shunting or with hepatic failure. Also, with the availability of a good table-top analyzer (e.g., blood ammonia checker, Me- narini; http://www.menarini.com), ammonia has become a practical parameter to measure. As much as an abnormal plasma ammonia concentration is a useful diagnostic tool for the diagnosis of a PSS, it can not be used to discriminate a single congenital from multiple acquired shunts.45Abdominal ultrasonography may be used to directly visualize the shunt vessel and it is advisable to try to find the localization of the shunt before surgery.76-81 If ultrasonography is inconclusive, the shunt may be definitively demonstrated by rectal or splenic scintigraphy.76 Splenic scintigraphy requires a smaller amount of radioactive material than rectal scintigraphy, so that less time is required until the patient can be cleared for surgery (Figures 7.12 and 7.13). Contrast angiography by catheterization of the portal or splenic vein is more invasive and usually not necessary (Figures 7.14 and 7.15). Changes seen with liver histology are not specific for PSS and are similar to those seen with portal vein hypoplasia.4
Management
Surgical closure of the shunt is the treatment of choice for patients with PSS. The shunt is closed partially, permitting some portal blood to bypass the liver so that the portal pressure does not suddenly increase too much. There are several techniques such as the traditional method of placing a suture ligature, cellophane banding, or the use of an ameroid constrictor. With all these techniques, the shunt is only closed partially and
it then usually closes completely on its own over time (48 weeks).72-82-86 After partial closure of the shunt, more portal blood reaches the liver, so that production of local growth factors commences, followed by rapid growth of the liver, less resistance to portal blood flow, and further improvement of liver perfusion and growth.
Such a positive outcome is achieved in about 60% of all cases. Suboptimal results may be due to inadequate development of the portal vein and /or incomplete hepatic growth.86It is important to evaluate blood glucose concentrations before, during, and after surgery, since some of these animals may develop hypoglycemia due to poor liver function. Coagulation should also be checked before surgery and if necessary be corrected by a blood or plasma transfusion.
The surgical results in cats are less optimal than those in dogs.87 Cats have more problems with the large changes in blood flow and pressure, and often die in the immediate postoperative period.
Especially in small breed dogs, a sudden derangement of brain function (cerebrocortical necrosis) may occur 2-3 days after surgery. The pathogenesis of this complication is unknown, but increased intracranial pressure and cerebral edema is most likely an important cause. In our experience, immediate osmotic diuresis with mannitol may prevent permanent brain damage. The onset of this complication is seen as a sudden mental derangement after an initially good post-operative recovery. If not detected and treated immediately, this complication leads to severe neurological signs very similar to those seen with HE, but without periodic changes and not accompanied by hyperammonemia.
In approximately 20% of patients, incomplete hepatic growth following surgery leads to increased portal pressure, which may initiate the development of acquired portosystemic collaterals. Such patients only show a partial improvement, followed by a recurrence of HE after approximately 6-8 weeks. Even with this complication, such patients usually benefit from surgery. They often need permanent dietary management and lactulose and /or antibiotic therapy, and can often be maintained very well with these measures. Complete recovery usually occurs within 3-4 weeks. Even severe neurological signs are completely reversible in most cases. The prognosis of surgical intervention depends on the type of the shunt.
Some owners opt not to pursue surgical therapy and supportive care may consist of a low protein diet, lactulose, and/or antibiotic therapy with a poorly absorbable antibiotic (i.e., neomycin, see 7.4.3).44,73,88 The long-term prognosis for conservatively managed patients has not been studied in detail, but it is generally assumed that conservative management is less than ideal.
7.4.2.2 Hepatic congestion
Pathogenesis
Hepatic congestion is usually caused by congestive heart disease such as atrial fibrillation or pericardial effusion. An obstruction of the thoracic part of the caudal vena cava by a tumor or thrombus can also cause hepatic congestion. Ascites caused by hepatic congestion is always hemorrhagic, because erythrocytes escape from the congested capillary bed. In contrast, ascites due to primary liver disease is usually clear and colorless.
Hepatic congestion has no important functional consequences for the liver.4 Hepatic enzymes, bile acids, and albumin are usually not or only mildly abnormal.
The congested liver is enlarged, darkly colored, and usually has a layer of fibrin attached to the capsule. In chronic cases, the capsule becomes thick and fibrotic. There is no formation of portosystemic collaterals because there is no pressure gradient between the portal vein and the systemic circulation.
Symptoms
The symptoms of hepatic congestion are those of the underlying disease process. As the liver functions remain largely unchanged, there are generally no signs of liver disease or failure.
Diagnosis
Ultrasonographic changes are typical of hepatic congestion and reveal congested branches of the hepatic vein. A severely congested liver should not be biopsied because of the increased risk of hemorrhage.
Management
No treatment for hepatic congestion is required, but hepatic congestion resolves when the underlying disease process is treated.
7.4.2.3 Primary portal vein hypoplasia
Pathogenesis
There has been much confusion about this condition in the literature, mainly because different names have been used for it, including microvascular dysplasia and congenital liver fibro- sis.4,45,89-93 However, the name primary portal vein hypoplasia
has recently been adopted by the WSAVA standardization panel for hepatic diseases and should thus be used exclusively. Primary portal vein hypoplasia is characterized by an insufficient development of the terminal intrahepatic branches of the portal vein. Consequently, portal blood does not reach the hepatocytes. This disease may vary from a slight reduction of the number of terminal portal branches to a complete absence of them. In the latter case, there is usually also an abnormal extrahepatic portal vein, which may have a very thick fibrotic wall. There is a tendency for the formation of portal fibrosis, the degree of which may also vary from virtually absent to severe. There are many subclinical cases that may only be identified by chance after blood work reveals increased serum bile acids or plasma ammonia concentrations. More severe cases may present for ascites and HE, and may reveal acquired portosystemic collaterals upon abdominal ultrasound examination. Severe cases are usually presented at a young age, most often within the first year of life. There is reduced portal blood flow to the liver, which, depending on the severity of the condition, does not increase adequately as the patient is growing. In contrast to dogs with PSS, the kidneys are not enlarged in dogs with primary portal vein hypoplasia. Primary portal vein hypoplasia is congenital and is not progressive.

Figure 7.16:
Primary portal vein hypoplasia. This figure shows an angiogram in a dog with primary portal vein hypoplasia. Note that none of the injected dye appears to reach the liver but instead is shunted away from the liver. Such hepatofugal blood flow can also be documented by abdominal ultrasound.
Histologically, there is hypoplasia of the terminal branches of the portal vein, and arteriolar hyperplasia. There may also be a variable amount of portal fibrosis. These changes are, however, not specific and may also be present in dogs with PSS or arteriovenous fistulas.
fore, also depends on the experience of the ultrasonographer. Ascites may be present in dogs with portal vein hypoplasia (colorless), arteriovenous fistula (colorless), hepatic congestion (hemorrhagic), and portal vein thrombosis (hemorrhagic), but not in dogs with congenital shunts.
Symptoms
Patients with primary portal vein hypoplasia can present with ascites, HE, polydipsia, and occasionally vomiting. Symptoms may be mild or absent in less severe or subclinical cases, respectively.
Diagnosis
Blood work may show hypoalbuminemia, increased serum bile acids and plasma ammonia concentrations, and an abnormal ammonia tolerance test. Elevation of liver enzyme activities may or may not be present. The differentiation of primary portal vein hypoplasia from chronic hepatitis /cirrhosis can only be made by a histological examination of a liver biopsy. In cases with portal vein hypoplasia, the histological findings are identical to that of PSS. Therefore, the differentiation from PSS is based on the histological interpretation in combination with ultrasonography and /or scintigraphy. Dogs with severe portal vein hypoplasia show hepatofugal flow (i.e., flow in the portal vein that is directed away from the liver; Figure 7.16) when examined by Doppler ultrasonography. Ultrasonographic exclusion of PSS is part of the diagnosis; which, there-
Management
There is no specific therapy for primary portal vein hypoplasia and recovery is not possible. Only symptomatic treatment can be employed to reduce HE (i.e., diet, lactulose, and /or neomycin) and limit the formation of ascites (i.e., potassium-sparing diuretics).
7.4.2.4 Portal vein thrombosis
Pathogenesis
Thrombosis of the portal vein is a rare disease, seen in patients that are hypercoagulable, as occurs in patients with nephrotic syndrome or in those with an abnormal intima of the portal vein.4,38 In some cases, it is associated with pancreatitis or with chronic exposure to corticosteroids (endogenous or exogenous). Depending on the degree of obstruction of the portal vein, portal vein thrombosis can lead to acute portal hypertension if the obstruction occurs suddenly or portal hypertension and formation of collaterals when there is gradual occlusion. Thrombosis may occur in the left or the right main branch of the portal vein. This may lead to a one-sided atrophy of the liver and compensatory hyperplasia of the other side, which in turn may result in dislocation of the stomach. The liver, which is deprived of portal blood, develops atrophy of the portal venous branches and concurrently compensatory hypertrophy of the arterioles. This histological picture is usually indistinguishable from that seen in patients with congenital shunts, primary portal vein hypoplasia, or an arteriovenous fistula.
Hemorrhagic ascites is only seen in patients with portal vein thrombosis and hepatic congestion. Patients with chronic portal vein thrombosis may develop portosystemic collaterals and may show clinical signs of HE.
Symptoms
Many patients with portal vein thrombosis have hemorrhagic ascites. In chronic cases there may also be signs of HE. In the acute phase, there is general malaise and apathy, and often also nausea and vomiting.
Diagnosis
Blood work often reveals increased serum liver enzyme activities and serum bile acids concentrations. In chronic cases with portosystemic collateral formation, hyperammonemia may also be present. The diagnosis can be made during abdominal ultrasonography by direct visualization of the thrombus. Doppler examination reveals a reduced portal blood flow, which may be hepatofugal in chronic cases. One-sided thrombosis of a main branch of the portal vein is usually accompanied by an asymmetric liver.
Management
Therapy depends on the underlying disorder (e.g., nephrotic syndrome). Acute thrombosis may be relieved surgically. Platelet inactivation by aspirin (0.5 mg/kg PO q 12 h) has been advised, but a beneficial effect has not yet been documented. Patients with a one-sided thrombosis of a main branch usually recover spontaneously when the perfused side of the liver hypertrophies in compensation and normal liver function is restored. In chronic cases with HE, symptomatic therapy for HE may be required.
7.4.2.5 Arteriovenous fistulas an abnormally high arterial pressure in the portal system, thus leading to portal hypertension. The fistulas are usually located within a liver lobe and consist of multiple tortuous, pulsatile vessels, which may be recognized during abdominal ultrasonography. Dogs with this disease often also have portal vein hypoplasia, which is associated with a guarded prognosis for surgical correction, but hepatic lobectomy may be sufficient to remove the fistula. Portal hypertension leads to the formation of multiple portosystemic collaterals and ascites. Intrahepatic fistulas cause a reversal of blood flow in the portal system, also known as hepatofugal blood flow (i.e., blood flow away from the liver). Hepatofugal blood flow can be diagnosed by Doppler ultrasonography. It can also be seen in patients with primary portal vein hypoplasia and in some patients with portal vein thrombosis.
Patients with arteriovenous fistulas usually have multiple fistulas that are distinctly visible as wide, tortuous, and pulsatile vessels. Intrahepatic fistulas result in an enlarged liver lobe that contains many cavernous vessels. Histologically, the portal areas show many arterioles and hypoplastic portal veins.
Symptoms
Patients with arteriovenous fistulas present with the same clinical symptoms as those with portal hypertension, including HE, ascites, depression, anorexia, and vomiting.
Diagnosis
The laboratory evaluation of patients with arteriovenous fistulas shows increased serum bile acids concentrations and usually also an increased plasma ammonia concentration that is due to the formation of the portosystemic collaterals. Ultrasonography reveals wide tortuous pulsatile vessels.
Management
Surgical removal of the affected liver lobe or the extrahepatic fistula has been found to be beneficial. However, if the patient also has congenital portal vein hypoplasia, lobectomy may only lead to a partial improvement and these patients will need permanent management with a low protein diet, lactulose, and /or antibiotic therapy. Appropriately managed dogs can be well maintained for many years.
Pathogenesis
Arteriovenous fistulas are shunts between the hepatic artery and the portal venous system and represent a rather uncommon congenital disorder.4,94 Arteriovenous fistulas will lead to
7.4.3