Diagnosis and prognosis of canine cardiomyopathy
Dilated cardiomyopathy (DCM) is a significant cause of congestive heart failure in dogs, characterised by the enlargement and impaired contraction of the left or both ventricles [1-3].
The development of DCM can be classified into three main stages [4, 5]. In Stage 1, the heart appears normal, with no clinical evidence of heart disease and often includes dogs that are genetically predisposed to DCM [6]. Stage2 (the preclinical or occult phase) is characterised by morphological and electrical cardiac changes with a prolonged period without overt clinical symptoms. Stage
3 (the overt phase) includes clinical signs of congestive heart failure [1-3, 7]. It should also be noted that adult DCM clinical signs can vary between breeds.
The gold standard approach to DCM diagnosis relies on echocardiographic and 24-hour electrocardiographic (ECG) assessments (Figure 1), in conjunction with monitoring clinical presentation and signalment [7-9]. The most common early clinical signs include exercise intolerance and heart murmurs/irregular heart rhythms. As the condition develops pulmonary congestion edema may develop and abdominal fluid accumulation and/or pleural effusion may be present. Notable other signs including weakness, inappetence, weight loss, breathlessness, coughing, increased breathing rate, collapse and lethargy are more frequent in dogs with heart failure caused by DCM, as is sudden death [3]. Congenital or acquired cardiac diseases with similar presentations to DCM must be also be excluded [10, 11].
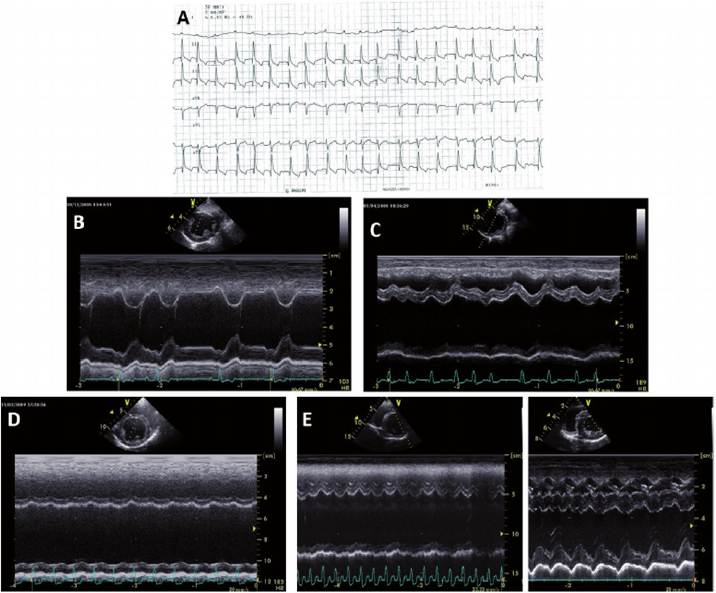
Figure 1.
A) Six lead ECG showingfast atrial fibrillation in a dog with dilated cardiomyopathy (DCM). Motion-mode echocardiogram from dogs that were classified as B) clinically normal, C) DCM showing dilation of the left ventricle and irregular filling associated with atrial fibrillation, D) DCM showing dilation of the left ventricle and a sinus tachycardia, and E) DCM (Left) alongside a motion-mode echocardiogram from a normal dog (Right), note the difference in the size of the ventricles and the amount of movement in the walls.
Echocardiography is used to assess left ventricular (LV) dimensions and function, where a dilated ventricle, based on M-mode or 2D measurements, with reduced contractility is indicative of DCM [9, 12]. M-mode is a time motion technique displaying the movement of structures over several cardiac cycles along a specific plane [13, 14]. The use of M-mode in conjunction with ECG allows LV measurements to be made more reliably (see Figure 1 for examples). The LV end-diastolic internal diameter (LVIDd) should be measured during the onset of the QRS complex and near the end of the T wave for LV internal dimension during systole (LVIDs) [15]. Comparisons are ideally made against breed-specific LV measurements, but where this is not possible values should be compared to breeds of a similar size and weight [9].
Fractional shortening is a major indicator of systolic function, where values less than 20-25% suggest impaired contractility. This is calculated as follows:
FS = [( LVIDd- LVIDs ) / LVIDd] X100 (1)
In some cases, fractional shortening may be misleading, for example in athletic breeds values may appear to be lower, and in dogs with severe mitral regurgitation they can be higher [2, 15, 16], therefore caution is recommended when making a diagnosis. End point to septal separation (EPSS) is the minimum distance between the anterior mitral leaflet (E point) to the LV septal wall, during the rapid filling phase of diastole [17, 18]. An EPSS measurement of >10 mm in any breed is considered abnormal. Increased values can occur in volume overload or reduced fractional shortening resulting in LV dilation [11, 13].
A characteristic feature of DCM is the ventricular chamber becoming more spherical as the ventricle dilates [19]. The index of sphericity (SI) is calculated during diastole by dividing the LV length with the LV width, where a value 80 ml/m2 is a strong indication of systolic dysfunction [2, 8, 22]. Ejection fraction (EF) is calculated in a similar way to fractional shortening, but volume measurements are used as follows:
EF = ( EDV- ESV) /EDV (2)
Thus, EF takes into account both radial and longitudinal cardiac changes, where dogs with EF breeds these may precede echocardiographic abnormalities [25, 26].
Atrial fibrillation (AF) is a common supraventricular tachyarrhythmia in large and giant breeds [3, 27]. Despite the presence of AF in a large percentage of dogs with DCM, the mechanistic and clinical relationship between DCM and AF has not been clarified [16-19]. Figure IA shows an example of a six lead ECG showing fast atrial fibrillation in a dog with DCM. One canine study showed that 80.5% of individuals with DCM also had a diagnosis of AF [20], with another study showing occurrence in 87.6% of the patients [19]. Most individuals were diagnosed with AF at the same time as DCM or in the 2 years prior to the diagnosis of DCM, which indicates that AF may be a precursor to a clinical diagnosis of DCM [20]. Therefore, individuals diagnosed with AF should be carefully monitored and regularly presented for heart testing to check for DCM. There is the potential to improve the survival of individuals diagnosed with AF by treating them with drugs such as pimobendan prior to the development of DCM or heart failure [21].
Ventricular premature complexes (VPC) appear to be more common in the Doberman and Boxer breeds than other breeds. In Dobermans, >300 VPCs/24 hours, or two successive Holter recordings within one year showing between 50 and 300 VPCs/24 hours is considered diagnostic for preclinical DCM, even if echocardiographic findings appear normal [10]. Thus, Holter monitoring is useful in identifying Dobermans that are destined to develop DCM. Similar diagnostic reference ranges are lacking in the Boxer but >50 VPCs/24 hours would be considered to be abnormal [2].
The European Society of Veterinary Cardiology (ESVC) has proposed a scoring system to aid in the diagnosis of DCM, especially for dogs that present with equivocal findings. The following cardiac changes fall into the major criteria and are allocated 3 points each: (i) LV enlargement, (ii) reduced systolic function, and (iii) increased LV sphericity. The remaining findings are considered minor (1 point each): (a) arrythmias in specific breeds; (b) AF; (c) increased EPSS; (d) increased pre-ejection period: ejection time ratio; (e) LV fractional shortening in equivocal range; (f) left or biatrial enlargement.
A total of ≥6 points is indicative of DCM and a score of 1-5 should encourage repeated examination for evidence of disease progression [2].Annual screening using echocardiography and Holter monitoring, has been recommended for breeds genetically predisposed to DCM, including Dobermans, Boxers, Newfoundlands, Great Danes and Irish Wolfhounds (IWH). Detection of the pre-clinical phase allows earlier therapeutic intervention, can improve prognosis, and enables the removal of affected dogs from breeding programmes if appropriate [10, 28, 29]. This is particularly important in Dobermans as 30% die suddenly prior to the onset of congestive heart failure [30, 31]. However, yearly testing can be expensive as it often requires referral to specialists thus restricting accessibility. In some countries, breed groups/welfare groups have set up testing programmes, and some even support these financially or fundraise, due to the concern about the numbers of animals developing cardiovascular problems.
Given the complex nature of diagnosis, that gold standard tests may not always be available for every client, and the financial restraints faced by some owners, development of further and/or potentially cost effective diagnosis tools are always needed [5, 7]. Biomarkers such as N-Terminal pro B-type natriuretic peptide (NT-proBNP) have been used in humans to identify patients with occult LV dysfunction. The NT-proBNP assay is useful to differentiate between cardiac and non-cardiac causes of respiratory distress, where conventional testing alone could lead to ambiguous results [28, 32]. In a study of 328 Dobermans, those that had plasma concentrations of NT-proBNP >400 pmol/L, in the absence of renal dysfunction, were more likely to have echocardiographic abnormalities. However, the results cannot be considered diagnostic as NT-proBNP concentrations overlapped in groups of dogs with and without preclinical DCM [7, 33]. The use of in-house 5-minute ECG has reasonable specificity and in Dobermans the detection of 1 VPC strongly suggests that >100 VPC would be recorded via Holter.
However, due to poor sensitivity, absence of VPC should not rule out the possibility of DCM [6, 23]. The emphasis is that the results from these tests should not be used to establish a diagnosis, but rather to identify dogs that would benefit further from more costly diagnostic tests [34].Two histopathological variations of canine DCM have been identified: “attenuated wavy fibre type” and “fatty infiltration type” [22] indicating that differing types of canine DCM exist. The fatty infiltration type has only been reported in Doberman Pinschers, Estrela mountain dogs, Great Danes, and Boxers [22—25]; whereas the wavy fibre type can occur in all breeds [22, 23]. As the wavy fibre type is found across breeds, and in many individuals, it could be the tissue’s response to the other processes of DCM. In general, atrophy, or attenuation, of muscle fibres is often a result of processes that prevent normal contractile ability: contractile ability is consistently compromised in DCM [26]. The clinical relevance and prevalence of these two histopathological variants remain to be established, and as post mortem tissue is required presently for phenotypic analysis this may not be useful in a clinical setting but could provide valuable research insights into the disorder [27].
The long-term prognosis of canine DCM can be highly variable, with well managed dogs maintaining a good quality of life for many years and others dying within weeks of diagnosis despite careful clinical management [19, 28, 29]. There are some breed specific prognosis trends such as Doberman Pinschers which generally have a poor prognosis. Their mean time to death (from diagnosis) is in the range of 7.4 to
9.7 weeks [29, 30], which is low in comparison to other breeds reported to be about four times that at 34 weeks [29]. Doberman Pinschers also had the lowest upper quartile range for survival time in a study, but analysis carried out by the same research showed that Great Danes also suffer from a poor prognosis, with the lowest median survival time of any breed [17, 28].
Age of onset can also affect prognosis and may be a useful indicator that differing types of canine DCM exist. Portuguese water dogs have a specific juvenile form of DCM, where age of onset is measured in weeks from birth [31, 32], while in most other cases age of onset is measured in years [17]. Great Danes have a mean age of onset of 4.8 (SD ± 2.3) years [33], comparable to Irish Wolfhound mean age of onset of 4.40 (SD ± 2.03) years [34]; but lower than Doberman Pinscher’s at 7.3 years in males and 8.6 years in females [30]. Once identified, knowledge about the differing canine DCM types could benefit current and future potential treatments in addition to elucidating other clinically important factors in canine DCM, such as longevity and prognosis.
3.