Diagnostic Imaging in Equine Patients
Ultrasonography, performed transrectally, is utilised routinely for assessment of a mare's reproductive tract, to diagnose pregnancy and to stage the oestrus cycle in mares. Small portable ultrasound machines facilitate this use in ambulatory practice, while larger more powerful machines are used for transcutaneous abdominal ultrasound.
Thorough assessment of the abdomen requires low-frequency (3-5 MHz) ultrasound transducers that can scan up to depths of 20-25 cm. Numerous abdominal ultrasound protocols have been published detailing effective abdominal screening for horses with abdominal pain (colic), and abdominal ultrasound is considered routine in equine hospitals for assessment of horses with colic. Ultrasound has high diagnostic specificity and sensitivity for the identification of horses with strangulating intestinal lesions (colon volvulus and small intestinal strangulation), nephrosplenic entrapment (Figure 10.1) of the large colon, gastric impactions, displacement of the large colon and diaphragmatic hernia. Ultrasound can also detect peritoneal effusions and is commonly used in the investigation of the genitourinary systems. Ultrasound is also utilised to identify the location of retained abdominal testis and is performed routinely in horses with weight loss and/or diarrhoea. Due to the fundamental principles of ultrasound, it has limited capacity in the presence of gas-filled viscus, and imaging deep to the gas is impossible.Gastroscopy in adults is performed with a 3m flexible video endoscope and is indicated in horses with suspected oesophageal and gastric disease. The procedure is performed in standing, often lightly sedated horses following at least 12 hours of fasting to ensure that the stomach is empty. Gastric ulcers are the most commonly reported gastric disease in horses and are found in the squamous portion of the stomach near the margo plicatus (Figure 4.1) or in the glandular portion of the stomach around the pylorus.
Gastroscopy is also useful for diagnosing and monitoring response to treatment of gastric impaction and in younger horses with gastric outflow obstruction. Bot fly larvae (Gastrophilus) are infrequently encountered attached to the squamous portion of the stomach but are considered incidental.Laparoscopy (Figures 18.8-18.10) is performed in adult horses in the standing position to access the dorsal parts of the abdomen and, under general anaesthesia, to access
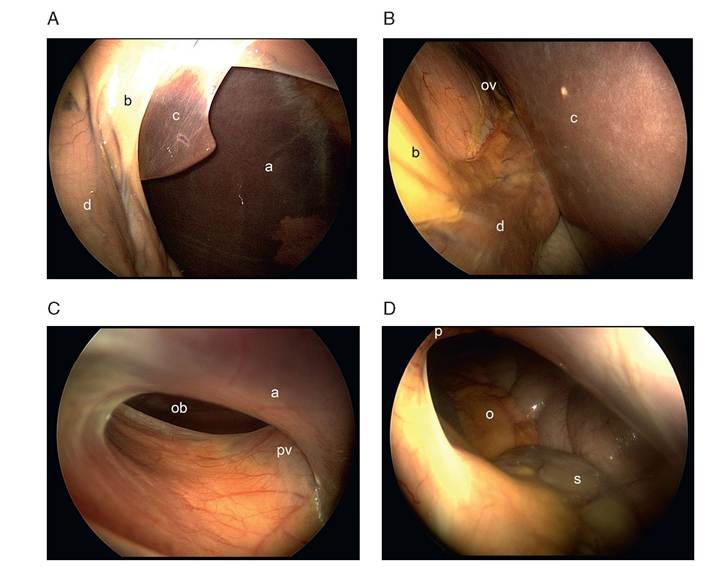
Figure 18.8 Laparoscopic examination of the epiploic foramen. Images were obtained from the right side of the abdomen. (A) The right lobe (label a) and caudate lobe (label c) of the liver lie cranial to the duodenum (label d) suspended by the hepatoduodenal ligament (label b). (B) The laparoscope is advanced between the caudate lobe (label c) of the liver and the hepatoduodenal ligament (label b) to visualise the omental vestibule (ov). (C) The laparoscope is advanced into the omental vestibule where the omental bursa (ob) is seen beyond the epiploic foramen. The portal vein (pv) lies in a ventral position at this location and is covered by serosa. (D) The laparoscope is placed through the epiploic foramen to the left side of the abdomen where the lesser curvature of the stomach (s) and omentum (o) are visible. The edge of the pancreas within the hepatopancreatic fold (p) can just be seen dorsally.
the ventral parts. Laparoscopy is performed with rigid 10 mm wide forward or forwardoblique (30°) endoscope placed through an 11 mm diameter cannula positioned in the paralumbar fossa or the 17th intercostal space. Typically, the abdomen is distended slightly with medical grade CO2 to improve visualisation (pneumoperitoneum). Horses undergoing laparoscopy under general anaesthesia are often positioned in the Trendelenburg position (dorsal recumbency with the head down) or reverse- Trendelenburg position (head up) if greater access is required to the caudal or cranial abdomen, respectively.
The main indications for laparoscopy in adult horses are ovariectomy of diseased ovaries (granulosa cell tumour or haemorrhaging follicles) and cryptorchidectomy. Closure of the epiploic foramen with mesh implants is performed in horses with previous history of epiploic foramen entrapment (see Section 3.2 and Figure 3.1). Closure of the nephrosplenic space is undertaken in horses at risk of nephrosplenic entrapment of the colon by suturing the spleen to the nephrosplenic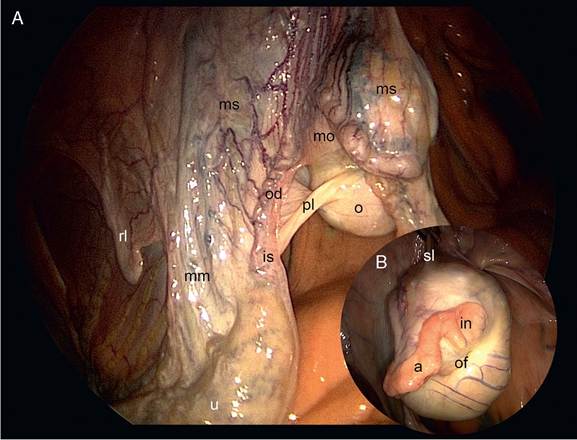
Figure 18.9 (A) Laparoscopic view of the right ovary and cranial aspect of the right uterine horn of a mare. The laparoscope has been inserted through the right flank. (B) The inset is an image of the medial aspect of the right ovary. The ovary (o) is supported from the dorsal body wall by the suspensory ligament (sl) and mesovarium (mo) and is attached to the cranial aspect of the uterine horn by the proper ligament (pl). The uterus (u) is suspended to the dorsal body wall by the broad ligament/mesometrium (mm) and connected to the lateral body wall by the round ligament (rl). The ovulation fossa (ov) is visible on the medial side of the ovary (o) adjacent to the infundibulum (in) of the oviduct (od). The infundibulum continues as the ampulla (a) of the oviduct (od) as it wraps around the caudal aspect of the ovary (o). The oviduct continues as a convoluted tube supported by the mesosalpinx before widening at the isthmus (is) where the oviduct joins the cranial uterine horn.
ligament, and the inguinal canal of stallions can be partially closed by a variety of laparoscopically guided methods. Other less common indications for laparoscopy in adult horses include Uteropexy (fixation of a displaced uterus), or imbrication of the broad ligament (surgical overlapping of the ligament) of the uterus in mares with a pendulous uterus and treatment of obstructed oviducts with prostaglandin.
With the advent of larger-bore CT scanners, imaging of the caudal abdomen and pelvis is possible in the horse, but this technique has not been investigated for this purpose to date. It is probable that abdominal CT scanning in horses will be reported in the future.
18.7