Heart
The heart is a cone-shaped hollow muscular structure. The base is directed dorsad or cra- niodorsad and is attached to other thoracic structures by large arteries, veins, and the pericardial sac.
The apex of the heart is directed ventrad and is entirely free within the pericardial sac. In the living animal, the right side of the heart is on the right side of the body but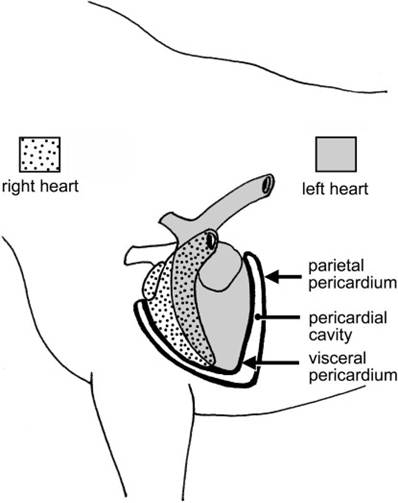
Figure 17-1. Orientation of the heart within the thorax. The right side of the heart lies more cranial than the left. The surface of the heart is covered with visceral pericardium, which the pericardial space separates from the parietal pericardium. The parietal pericardium is attached by fibrous tissue to overlying pericardial pleura (not shown). These three layers constitute the pericardial sac.
oriented more cranial than the left side, which is left and somewhat caudal (Fig. 17-1).
Pericardium
The heart is partially surrounded by a serous membrane called the pericardium. The pericardium, like other serous tissues (the pleura and peritoneum), creates a closed cavity (the pericardial space) that contains only a small amount of fluid for lubrication. The heart is invaginated into the pericardium much like a fist thrust into an inflated balloon (see Fig. 1-9). This arrangement results in two distinct layers of pericardium (Fig. 17-1). The inner layer, which is intimately adherent to the outer surface of the heart, is called visceral pericardium, or epicardium. The outer layer, called parietal pericardium, is continuous with the visceral layer at the base of the heart and is reinforced by a superficial fibrous layer (the fibrous pericardium), which in turn is covered by a layer of mediastinal pleura (also called pericardial pleura). The parietal pericardium, fibrous pericardium, and mediastinal pleura together form the pericardial sac, which is grossly identifiable as a thin but tough tissue surrounding the heart.
In cattle, the apex of the heart contacts the dome of the diaphragm, and the reticulum in the abdominal cavity lies on the caudal side of the diaphragm. Sharp metallic objects (most commonly, bits of wire) that are swallowed often accumulate in the reticulum. The contractions of this organ can cause these foreign bodies to penetrate the adjacent diaphragm and the pericardial sac, resulting in an infection of the sac called traumatic pericarditis, one manifestation of hardware disease. The tissues of the pericardium thicken, and fluid builds up within the pericardial sac, which leads to heart failure in affected cattle. Hardware disease is usually prevented by administering a magnet by mouth; the magnet, which tends to remain in the reticulum, gathers swallowed metallic objects and prevents them from migrating through the wall of the forestomach.
Cardiac Anatomy
The heart wall consists of three layers: an outer serous covering called epicardium, an inner endothelial lining called endocardium, and a thick muscular layer called myocardium.
The epicardium is the same as the visceral layer of pericardium. The endocardium is a layer of simple squamous endothelial cells that lines the chambers of the heart, covers the heart valves, and is continuous with the lining of the blood vessels. The myocardium consists of cardiac muscle, described in Chapter 8.
The heart is divided into right and left sides, which correspond to the low-pressure (pulmonary circulation) and high-pressure (systemic circulation) systems mentioned earlier. Each side has two chambers: an atrium, which receives blood by way of large veins, and a ventricle, which pumps blood from the heart through a large artery (Fig. 17-2). The atria are thin-walled chambers, each of which features an appendage called an auricle.
The myocardium of the ventricles, which pump blood back into vascular beds, is much thicker than that of the atria. The wall of the left ventricle is also thicker than that of the right; blood ejected from the left side during its contraction is under higher pressure than that ejected from the right ventricle. The right ventricle does not quite reach the apex of the heart, as the apex is formed entirely by the more muscular left ventricle.
The myocardium between the two chambers is the ventricular septum.Between the atrium and the ventricle of each side is an atrioventricular valve, or A-V valve (Fig. 17-2). The left A-V valve is occasionally called the bicuspid valve, because in humans it has two distinct flaps, or cusps. Another more commonly used synonym is mitral valve, because of its imagined resemblance to a bishop’s miter, or two-sided hat. The right A-V valve is also called the tricuspid valve because in humans it has three flaps or cusps. The thin valve leaflets are attached to the inner wall of the ventricle at the junction of atrium and ventricle. The free margins of the cusp are tethered to the interior of the ventricular wall by fibrous cords called chordae tendineae. The chordae tendineae attach to small muscular protrusions called papillary muscles that project into the lumina of the ventricles. These chordae tendineae prevent the valve from everting into the atrium when the ventricle contracts and closes the A-V valve by forcing blood against the ventricular side of the valve (Fig. 17-3A).
Each ventricle’s outflow tract features a semilunar valve that ensures blood flows only from the ventricle into the artery and not in the opposite direction. The semilunar valves have three cuplike leaflets, with convex side facing the ventricle (Fig. 17-3B). The aortic valve lies at the junction of the left ventricle and aorta; the pulmonary valve is at the junction of the right ventricle and pulmonary trunk.
Blood returning to the heart from the systemic circulation is delivered to the right atrium by the cranial and caudal venae cavae (singular vena cava) (Fig. 17-4). From the right atrium, this deoxygenated blood passes through the right A-V valve into the right ventricle. From the right side, the right ventricle wraps around the cranial side of the heart and terminates as the funnel-shaped conus arteriosus. The conus arteriosus is the origin of the pulmonary trunk, from which it is divided by the pulmonary valve.
Just distal to the pulmonary valve, the pulmonary trunk divides into right and left pulmonary arteries, carrying deoxygenated blood to the respective lungs.
A variable number of pulmonary veins return blood from the lungs to the left atrium. From the left atrium, blood passes through the left A-V valve into the thick-walled left ventricle. The left ventricle pumps the blood past the aortic valve into the aorta. The aorta and its branches carry oxygenated blood to all parts of the body (Fig. 17-4).
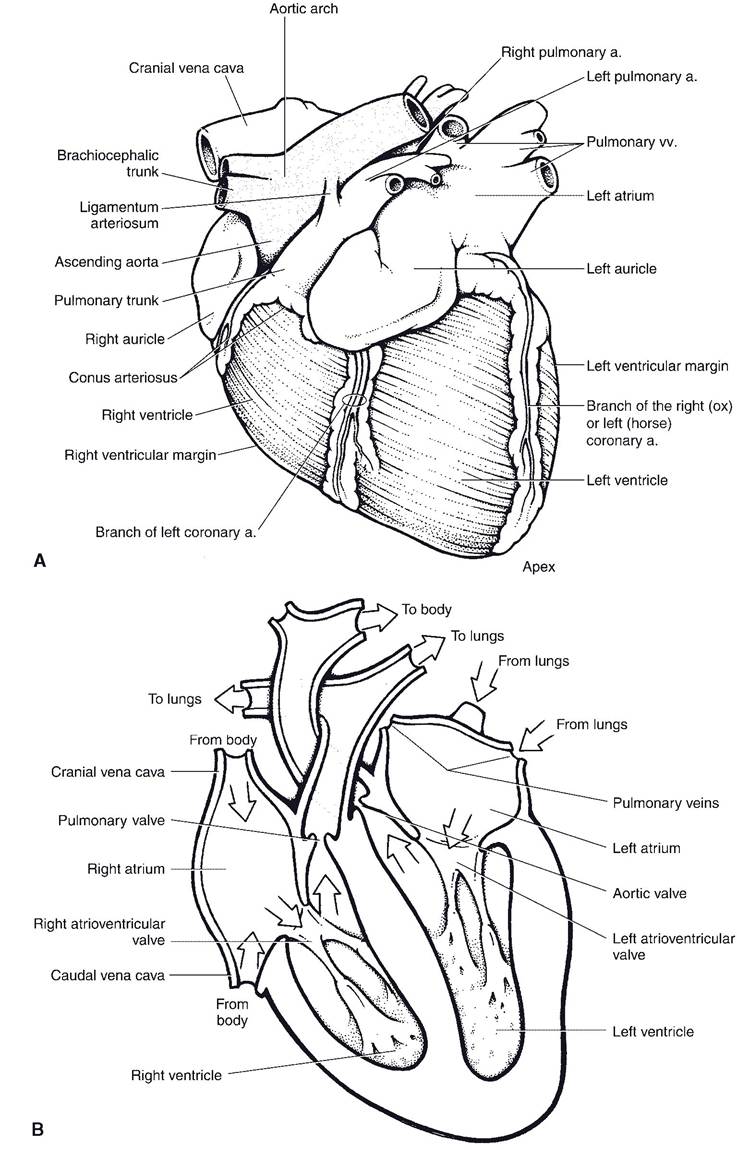
Figure 17-2. A) Left lateral view of the heart. B) Internal anatomy of the heart. Arrows depict the direction of blood flow. (Adapted with permission of Wiley-Blackwell from Smith B.J. Canine Anatomy. Baltimore: Lippincott Williams & Wilkins, 1999.)
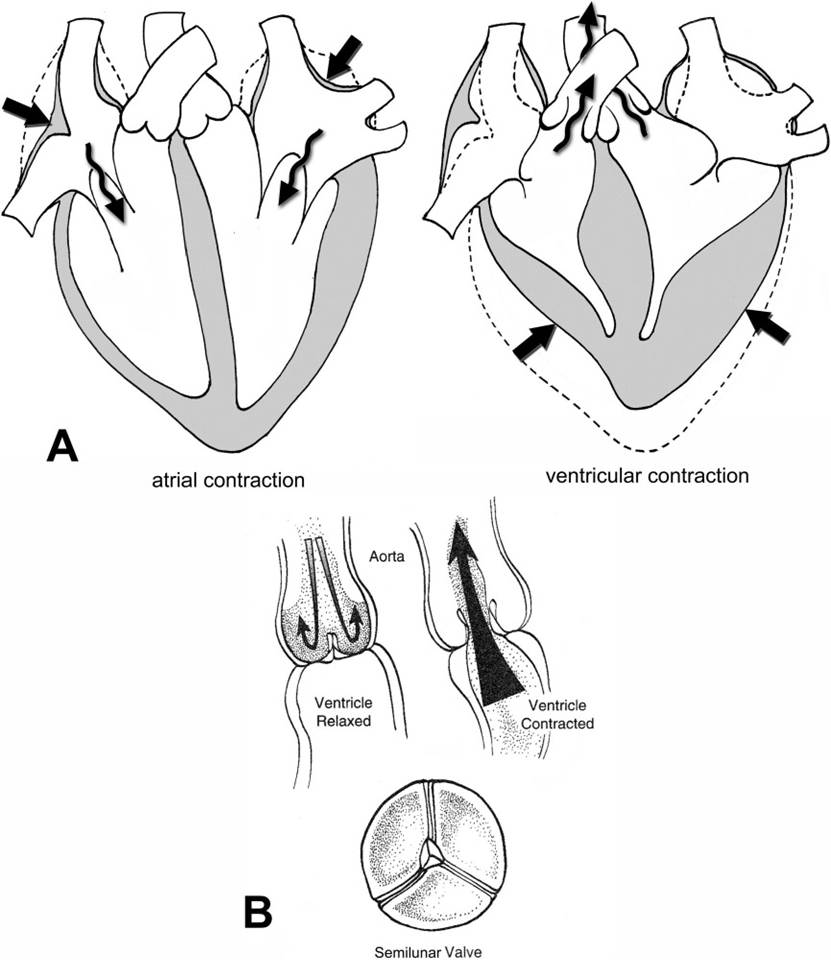
Figure 17-3. Cardiac valves. A) Function of A-V valves. During relaxation of the ventricle (left), the valve leaflets open to allow blood to flow from the atrium into the ventricle (arrow). During ventricular contraction (right), valve leaflets are forced closed. The chordae tendineae prevent the margins of the valve from everting back into the atrium. B) A semilunar valve. Viewed from above, the valve consists of three cuplike leaflets. During relaxation of the ventricle, the greater pressure within the vessel closes the valve. When the ventricle contracts, leaflets part and blood flows through the valve (arrow).
172" class="lazyload" data-src="/files/uch_group31/uch_pgroup304/uch_uch7233/image/image172.jpg">
Figure 17-4. Flow of blood through the heart. Broken lines indicate deoxygenated blood in the pulmonary circulation. Solid arrows indicate oxygenated blood in the systemic circulation. Blood flowing into the brachiocephalic trunk supplies primarily the cranial half of the animal, whereas that flowing into the main continuation of the aorta (arch and then thoracic aorta) supplies the caudal half of the animal.