Transportationof RESPIRATORY GASES
The blood carried O2 from the alveolar air to the body tissues and CO2 from the body tissues to the alveoli.
17.4 Respiratorycentres
(= Collection of neurones in brain stem)
17.4.1 General Function
1.
Responsible for the normal rhythm of respiration.2. Regulation of respiration (rate and depth) according to body conditions.
17.4.2 Location
Brain stem (within its reticular formation) extending from the upper part of the Pons to lower third of the M.O.
R.C. is composed of 5 bilateral centres
1. Inspiratory centre (I.C.) → M.O. (ventral).
2. Expiratory centre (E.C.) → M.O. (dorsal).
3. Pneumotaxic centre → upper Pons.
17.4.2.1 Inspiratory Centre (I.C.)
Location: Bilaterally situated in the ventral M.O. Nerve cells in the I.C. send out streams of impulses which travel down the M.O. to the AHCs of the spinal cord, which gives:
Phrenic N.: from the 3rd, 4th and 5th cervical segments to supply the diaphragm.
Thoracic Ns. (upper 10 intercostal nerves) supply intercostal muscles. These nerve impulses cause the muscles of inspiration to contract.
1. Stimulation of apneustic centre leads to stimulation of IC.
2. Reciprocal relationship: stimulation of one centre inhibits the other.
3. Stimulation of both centres at the same time → inspiration only.
17.4.2.4 Pneumotaxic Centre (PNC.) Location: at upper Pons.
Function:
a) During Eupnoea (normal breathing): Functionless! as PNC. is stimulated by I.C. and APC, whose discharges, during eupnoea, are not enough to stimulate PNC.
b) During deep inspiration or cutting vagi: PNC is stimulated, acting similarly to vagi but in a more powerful manner → inhibit APC and I.C.
→ change their continuous activity into rhythmic (= periodic) one but at a deeper level.I. C. is stronger than E.C.
17.4.2.2 Expiratory Centre (E.C)
Location: Bilaterally situated in the dorsal M.O.
Nerve cells in the E.C. send out streams of impulses which inhibit or interrupt the activity of I.C. → the muscles of inspiration relax → expiration follows passively.
1. Stimulation of apneustic centre leads to inhibition of EC.
2. Reciprocal relationship: stimulation of one centre inhibits the other.
3. Stimulation of both centres at the same time → inspiration only.
I. C. is stronger than E.C.
N.B.: I.C. is inherently active, unless inhibited by inhibitory impulses from:
| vagal fibres from lungs | _____ 1___ | pneumotaxic centre |
| 1 | 1 | |
| Direct | Indirect | |
| 1 | 1 | |
| inhibit I.C. | inhibit apneustic centre | |
| ↑_________________ | ________________ 1 |
17.4.2.5 GaspingCentre
Function:
a) During Eupnoea (normal breathing): Functionless (APC. → inhibit G.C.).
b) Just before death: G.C. is responsible for gasping respiration (= deep spasmodic inspiration), which is repeated for a few minutes before death occurs.
N.B.: G-C. is the last centre to fail.
17.4.3 Regulation of Respiratory Centre Activity
1. Nervous from:
a) Reflexes from respiratory system:
1. Hering-Breuer reflex.
2. Paradoxical reflex.
3. Sneezing reflex.
4. Cough reflex.
5. Afferent impulses from respiratory muscles.
2. b) Reflexes from the circulatory system:
1. From the right atrium (Harrison’s reflex).
2. From the vaso-sensory area.
c) Higher centres:
1. Cerebral cortex.
2. Hypothalamus.
3. d) Other parts of the body:
a. 1. Nervous regulation:
a.
i. Reflexes from respiratory system1. Hering-Breuer reflex: *Respiration is regulated by its own function (i.e., change in lung volume)
Inflation reflex
Deflation reflex
| = Inflation → inhibition of | Excessive |
| inspiration → expiration start | Deflation → |
| inhibition of | |
| expiration → | |
| inspiration start | |
| Stimulus: Normal inspiration Deep | Deep expiration |
inspiration (= excessive deflation of lungs)
Receptors: stimulation of stretch receptors
Inflation (stretch) receptors Deflation
(compression) receptors
Present in lungs (alveoli, alveolar sac, alveolar ducts), bronchi and bronchioles
Send inhibitory impulses Send excitatory
impulses
“more
receptors”
“more
impulses”
| Afferent: | Vagus (inhibitory fibres) | Vagus (excitatory fibres) | |
| Centers: | Inhibition | More | Stimulation |
| APC: | Inhibition | inhibition | Stimulation |
| IC: | --- | More | Inhibition |
| EC: | Functionless | inhibition | -- |
| PNC: | Activation | ||
| Active | |||
| Efferent: | previously mentioned | ||
| Response: | Inspiration is | Insp. is | Expiration is |
| inhibited and | stopped and | inhibited and | |
| exp. follows | expiration | inspiration start. | |
| passively without | follows | ||
| stimulation of | actively. | ||
| EC. | |||
These reflexes stop after cutting the vagus.
17.4.3.1 Mechanism of Deflation During Eupnoea
Deflation (= expiration) → 1) decreases the number of stretch receptors (stimulated inflation receptors) and consequently their discharge as the lung becomes smaller until disappearing by the end of expiration → 2) decreases vagal inhibitory impulses to APC and IC (which recover and restart their spontaneous “inherent” activity).
Inspiration starts, and Expiration is inhibited
N.B.: 1. No excitatory impulses reach respiratory centres in eupnoea.
2. In eupnoea, deflation receptors are not stimulated during expiration (they are stimulated only in deep expiration) because deflation is not sufficient. Therefore, no deflation reflex occurs in eupnoea; only inflation reflex occurs.
17.4.3.2 Importance of Hering-Breuer Reflexes
1. Maintain respiratory rhythm:
• When the lungs expand, it inhibits inspiration and expiration starts.
• When the lung empty → it inhibits expiration, and inspiration start.
2. Prevent excessive distension and collapse of lungs:
• This is important in animals that have no long thoracic cage, e.g., frogs.
N.B. : In some pathological conditions, e.g., pulmonary congestion (=excess blood in the lungs), respiration becomes shallow and rapid.
17.4.4 Para-Doxical Reflex
• = Forced inspiration stimulates more inspiration. This is short because receptors of the reflex are rapidly adapting, i.e., they stop function rapidly.
Mechanism: receptors, afferent, centre, efferent, and response → previously mentioned.
17.4.4.1 Importance of Para-doxical Reflex
1. Newborn infant → help to open his lungs.
2. During muscular exercise → helps to fill lungs maximally.
3. During normal respiration, deep inspiration helps to open any collapsed alveoli.
17.4.4.2 Functions of Pulmonary Vagi
1. Carry afferent impulses of Hering-Breuer and paradoxical reflexes.
2. Responsible for shallow, rapid respiration (during eupnea).
N.B.: cutting the vagi → deep and slow respiration (due to the absence of Hering-Breuer reflex). However, in panting animals (without sweat glands), cutting of the vagi does not cause deep and slow respiration, as the PNC is activated by the hypothalamus (heat-regulating centre). This is because panting aims to keep body temperature constant when these animals are exposed to hot weather.
3. Responsible for the rhythmic discharge of APC and IC.
17.4.4.3 Evidence
Isolation of PNC
Intact *— vagic → Cutted
Does not stop the continuous Apneustic respiration i.e. deep and rhythmic discharge from 1C slow respiration.
and APC.
1. Sneezing reflex
Stimulus: Irritation (chemical, mechanical) of muscles of nasal cavity.
Afferent: Branches of the trigeminal nerve. Response: Deep inspiration followed by rapid and strong expiration.
2. Cough reflex
Stimulus: Irritation (chemical, mechanical) of mm. of the larynx, trachea, and bronchi.
Afferent: Vagus nerve.
Response: Moderate inspiration followed by strong expiration with closed glottis (N.B. pressure inside the air passage reaches more than 100 mm Hg), then glottis opens suddenly → strong ejection of air and irritants (foreign body).
3. Afferent impulses from respiratory muscles:
Produce reflexes similar to Hering-Breuer reflexes, i.e., contraction of inspiratory muscles (diaphragm and intercostal muscles) → affemet impulses (pulmonary vagi) → inhibit IC (which recovers when these muscles relax during expiration).
17.4.4.4 Reflexes from the Circulatory System
1. From right atrium (Harrison’s reflex):
(= Increased venous returns increase respiratory rate)
Receptors: baroreceptors in the wall of the R. atrium, opening large veins (vena cava and pulmonary veins)
Stimulus: Venous return and distension at the opening of large veins
Afferent: Vagus.
Response: Increase respiratory rate.
Significance: helps oxygenation and removal of CO2 from excess venous return (that reaches the lung via pulmonary circulation).
2. From vaso-sensory area:
17.4.4.5 Carotid Sinus
Site: dilatation at the beginning of internal carotid = after bifurcation of carotid artery into the internal and external carotid.
Receptors: baroceptors present in the tunica adventitia in the wall of carotid artery.
stimulated by increase arterial blood pressure (ABP).
Afferent: Sinus nerve passes to MO as a branch of the glossopharyngeal N. or Herring N.
Function:
(1) When stimulated by increasing ABP than normal it send inhibitory impulses along their afferent nerves to respiratory and cardiovascular centres in the MO → inhibiting cardiac and respiratory centres.
(2) Normal ABP:
Baroceptors continuously send inhibitory impulses to MO centres but with little or no effect on RC.
(3) ∣ ABP than normal (e.g. haemorrhage): ∣num- ber of inhibitory impulses from pressor receptors Iactivity of RC → ↑resp. rate
17.4.4.6 AorticArch
• = curve between ascending and descending.
Site: parts of the thoracic aorta.
Receptors: baroceptors present in the tunica adventitia in the wall of carotid artery.
Stimulated by increase arterial blood pressure (ABP).
Afferent: The aortic nerve passes to MO as a branch of the Vagus.
In rabbits, it form a separate bundle = depressor N.:.
Function:
(1) When stimulated by increasing ABP than normal it send inhibitory impulses along their afferent nerves to respiratory and cardiovascular centres in the MO → inhibits cardiac and respiratory centres.
(2) normal ABP:
Baroceptors continuously send inhibitory impulses to MO centres but with little or no effect on RC.
(3) ∣ABP than normal (e.g. haemorrhage): Inumber of inhibitory impulses from pressoreceptors I activity of RC → ↑respiration rate.
17.4.4.7 Carotid Body and Aortic Body
Site: Origin of the carotid artery and aortic arch.
Receptors: Chemoreceptors present in the wall of carotid artery and aortic arch. They are sensitive to CO2, H+, or O2
Afferent: Carotid sinus and aortic arch.
Functions:
1. CO2 or H+ or decreased O2 cause excitatory impulses along their afferent nerves to respiratory and cardiovascular centres in the MO → Stimulate cardiac and respiratory centres.
2. normal CO2 and O2 tension in arterial blood: chemoreceptors continuously send excitatory impulses to RC.
3. ICO2 and ↑O 2 :|resp. rate.
17.4.4.8 Impulses from Higher Centres
1. Cerebral cortex:
Voluntary control for a short period: Voluntary hyperventilation: leads to a washout of CO2 from alveolar air and arterial blood → inhibition of respiration (limited duration).
Voluntary apnoea: Accumulation of CO2 in alveoli and arterial blood up to the level which stimulates respiration against the will.
Occurs during: speech, singing, blowing, sucking, micturition, defecation, and parturition. (Can be maintained for 1-3 minutes.)
2. Hypothalamus:
Emotion: e.g., fear, anger, sexual excitement,... etc.
a) Accelerate respiration:
Moderate, mild stimulation of posterior hypothalamic nuclei (which control sympathetic activity).
Severe, sudden anterior hypothalamic nuclei (which control parasympathetic activity) induce slow respiration.
b) Body temperature: Increase body temperature → increase resp. rate (to get rid of excess heat via evaporation of water vapour through expiration).
c) Panting: (occurs in animals that have no sweat glands, e.g., dogs and cat.)
Respiration rate increases up to 200/min (in hot weather) to increase heat loss via evaporation of H2O from the lungs and air passage through expiration, leading to the cooling of body temperature back to normal. The increased rate of respiration in panting is due to the stimulation of the panting centre in the hypothalamus, resulting in powerful stimulation of the PNC, which becomes more sensitive than the vagus.
17.4.4.9 Reflexes from Other Part of the Body
1. Conditioned reflexes:
Visual, auditory, or olfactory impulses → may accelerate or inhibit respiration. Centres of these reflexes lie in cerebral cortex. e.g.
• ↑resp. rate when the swimmer sees the swimming pool.
• ↑resp. rate when Teaser sees estrous female.
2. During deglutition:
Respiration is reflex inhibited by afferent impulses from the base of the tongue and pharynx along the 5th, 9th, and 10th cranial nerves to the deglutition centre in the MO, which inhibits RC.
3. Pouring cold water on the skin:
Causes apnea followed by deep inspiration. Afferent impulses arise from the cold receptors of the skin and pass along sensory nerves to the RC.
4. Pain sensation:
• Mild pain → accelerates respiration.
• Severe pain → inhibits or even stops respiration.
5. Adrenaline apnoea:
Injection (i.v.) of large dose of adrenaline → generalised vasoconstriction → ↑ABP → temporary stoppage of respiration (apnoea).
17.4.5 Chemical Regulation of Respiration
Generally, CO2, O2, and H+ conc. in arterial blood affect respiration via two mechanisms:
1. Direct: via blood supply to RC in MO and pons.
2. Indirect (reflex): stimulation of chemoreceptors of carotid and aortic bodies → afferent → centres → efferent → response.
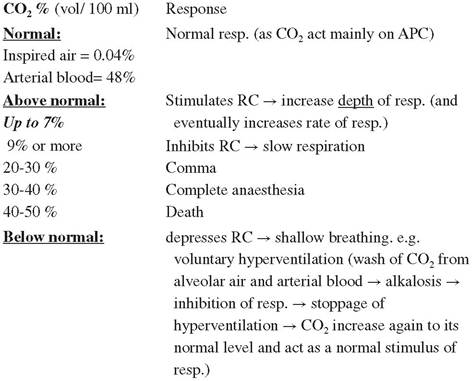
17.4.5.1 Response to Change in CO2 Tension
N.B.: The direct mechanism is more powerful (about 10 times) than reflex
evidence:
Cutting the afferent nerves of carotid and aortic bodies → respiration is little affected.
Deep anaesthesia → decreases sensitivity of RC to CO2.
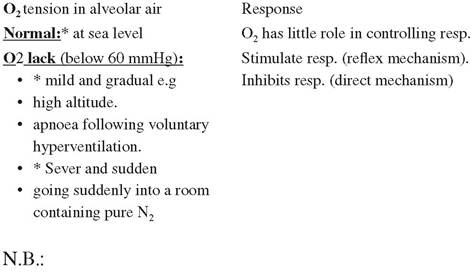
17.4.5.2 Response to Change in O2 Tension
* CO2 excess is more powerful in stimulating respiration than O2 lack. Why? Comment:
CO2 excess O2 lack
Stimulates RC.: Directly and Only reflex (while, directly inhibits) reflex
Evidence:
When a person is allowed to breathe in a bag containing air, after a short time, severe acceleration of respiration occurs due to the accumulation of CO2. When the experiment is repeated but CO2 is always removed by a CO2 absorber, e.g., soda lime, O2 may drop from 21% (normal) to 14% without acceleration of respiration.
* Giving O2 to patients under deep anaesthesia may end their life. Why?
Because giving O2 in this case stops the stimulatory effect of O2 lack on chemoreceptors, which is the main stimulus to the depressed RC (under deep anaesthesia), a mixture of O2 and 5% CO2 is given to keep the stimulation of RC both directly and reflexively.
17.4.5.3 Response to Change in H+
• Same as CO2.
17.4.5.3.1 Hypoxia
It means a lack of oxygen lack in tissues.
1. Hypoxic hypoxia.
2. Stagnant hypoxia.
3. Anaemic hypoxia.
4. Histotoxic hypoxia.
1. Hypoxic hypoxia
It is the defect oxygenation of blood in the lung due to:
a) Decrease air oxygen tension.
b) Defect gas exchange in lung diseases: pneumonia, emphysema, and pulmonary edema.
c) Mixing of arterial and venous blood.
2. Stagnant hypoxia
It is a decrease in blood flow through the tissues. There are two types of stagnant hypoxia:
a) Generalised stagnant hypoxia as in the case of congenital heart failure or polycythemia.
b) Localised stagnant hypoxia as in the case of thrombosis.
3. Anaemic hypoxia
It is a deficiency of Hb capable carrying O2, as in case of :
• Lack in Hb.
• Poisoning by CO (carboxyhemoglobin). CO combines with Hb 210 times more readily than O2.
• Formation of met Hb and sulpha Hb.
4. Histotoxic hypoxia
In which the tissues can’t utilise the oxygen from the blood as in the case of:
• Cyanide poisoning, which blocks cytochrome oxidase.
• Alcohol poisoning that blocks dehydrogenase.
| Types of hypoxia | O2 Tension in blood | O2 Content | O2Supply to the tissue | ||
| Arterial | Venous | Arterial | Venous | ||
| Hypoxic | 1 | 1 | 1 | 1 | 1 |
| Stagnant | Nil | 1 | Nil | 1 | 1 |
| Anaemin | Nil | 1 | 1 | 1 | 1 |
| Histotoxic | Nil | Super Nil | Nil | Super Nil | 1 |