Abnormal Coat Length and Density
Definition
Abnormalities in coat length and density can be subdivided into decreased coat length and density (alopecia, hypotrichosis) and increased coat length and density (hirsutism, hypertrichosis).
Hirsutism, or excessive body hair, is far less common than alopecia, which is an absence of hair from areas where hair is normally present. Alopecias are usually classified as scarring (cicatricial) or nonscarring (noncicatricial). In cicatricial alopecias the hair follicles are destroyed, and hair loss is permanent because neogenesis of the hair follicle does not occur in an adult mammal. In nonscarring alopecias the hair follicles are retained; therefore the potential for regrowth remains. Both alopecia and hirsutism may be complete or partial, diffuse or focal, and congenital or acquired.Mechanisms of Development of Abnormal Coat Length and Density
A basic understanding of the dynamics of hair structure and development is essential to an understanding of the mechanisms associated with pathologic changes in coat length and density.
The hair follicle and the sebaceous and apocrine glands are epidermal appendages. The hair follicle forms during fetal development as a downgrowth of epidermal cells toward a
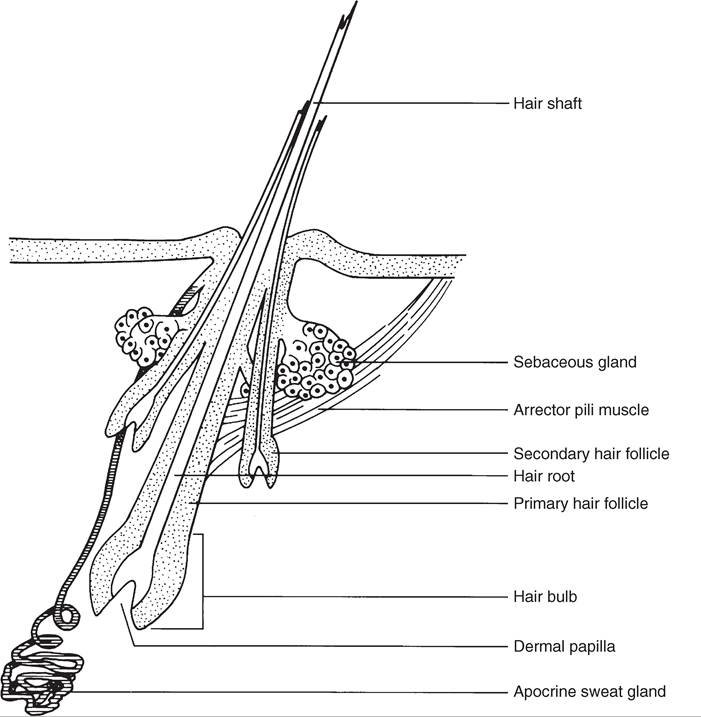
FIG. 11.7 Longitudinal section of a compound hair follicle.
group of mesenchymal cells that ultimately become the dermal papillae. The sebaceous and apocrine glands begin as buds of epithelium from the sides of the developing hair follicle.
Hair is composed of keratin and is the product of the hair follicle. The hair shaft is the part of the hair that emerges from the skin surface. The hair root is the part of the hair in the follicle. The hair bulb is a knob of epidermal cells that attaches the follicle to the dermal papilla. Both the hair follicle and the shaft have distinct layers.
There are two types of hair follicles: simple and compound. A simple hair follicle produces a single hair. A compound hair follicle produces multiple hairs with bundles of hairs sharing a common skin opening and a single follicle down to the level of the sebaceous gland. Below the sebaceous gland the follicle branches so that each hair has its own hair bulb. Horses and cattle have only simple follicles. Goats and sheep have a mixture of simple and compound hair follicles (Fig. 11.7).7,9The normal hair growth cycle is divided into repeating stages: anagen, catagen, telogen, and exogen, with the size and shape of the follicle changing during each stage (Fig. 11.8). The amount of time a follicle spends in each phase varies with the species, breed, individual, and body region. In addition, it is influenced by factors such as photoperiod, stress, and disease. Anagen is the active phase of hair growth. Catagen is the transition stage from the growing to the resting state. Catagen is short, and the hair quickly enters the telogen phase, in which hair growth stops. As the follicle reenters anagen, a new hair grows up beside the old and dislodges it (exogen). The signal that stimulates progression from telogen to anagen is unknown.
Coat abnormalities may result from a multitude of endogenous and exogenous factors that can modify the normal pattern of hair growth and development.
The length, density, and texture of the coat of a normal animal are determined genetically, and a variety of hereditary defects result in coat abnormalities. These defects may cause changes in hair length, density, or quality. Coat quality may be abnormal at birth or may become apparent sometime before 6 months of age. A given defect may alter the number of follicles present in the skin, or the number of follicles present may be normal but there may be genetic alterations in the way the hair is produced. Altered hair production may manifest as an increased or a decreased growth rate or as structural deformities that result in weak hair shafts that break easily.
Nutritional imbalances can affect growth and maintenance of the coat in various ways, depending on the species. Nutritional deficiencies may result in a shift of greater numbers of follicles into telogen, thus increasing shedding. Dietary carbohydrate and protein deficiencies reduce the length, diameter, and strength of hair. Supplementing the diet with carbohydrate and protein releases protein for keratin formation, provides energy to use protein, and maintains mitotic activity in the hair matrix. Fatty acid deficiencies affect lipid production in the skin, leading to a dry coat with increased fragility. A variety of vitamin and mineral deficiencies may also result in poor hair growth or quality.
Inflammatory skin diseases frequently result in hair loss. Infectious inflammatory processes such as dermatophytosis and pyoderma are usually directed specifically at the hair or hair follicle. Inflammatory processes directed elsewhere may still affect the hair follicle by sweeping it up as an “innocent
J r σ r
bystander.”
Hormonal effects on hair growth are complex. Thyroid hormones, corticosteroids, sex hormones, melanocyte-stimulating
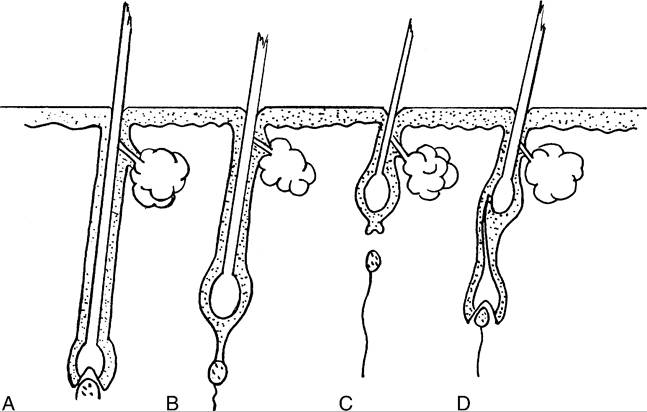
FIG. 11.8 Stages of the hair growth cycle. A, Anagen. B, Catagen. C, Telogen. D, Early anagen/exogen.
hormone (MSH), adrenocorticotropic hormone (ACTH), growth hormone, and prolactin all affect hair growth. The effect of a single hormone may be modified in the presence of other hormones, and the importance or effect of any one hormone on hair growth may differ from species to species. Hormonal variations affect the hair coat quality and length by altering the period of time that hair follicles spend in any given part of the cycle, by influencing the rate of hair growth, and by inducing follicular atrophy. External factors such as changes in the photoperiod influence hair growth by altering hormonal levels.
Trauma to the skin is a frequent secondary cause of hair loss.
Self-trauma induced by pruritus is the most common cause of alopecia. Hairs may be lost either from trauma to the hair shaft, resulting in breakage, or from trauma to the dermis, resulting in destruction of the hair follicle. In the former case, the hair regrows once the source of trauma has been removed. In the latter case, hair loss is permanent.A variety of factors can result in hair loss by causing an abrupt shift of hairs into the telogen phase. Recognized causes of telogen effluvium include stress from high fever or severe illness and parturition.
Approach to Diagnosis of Abnormal Coat Length and Density
The differential diagnosis of abnormalities resulting in increased coat length and density is relatively limited and does not provide much of a diagnostic dilemma for the clinician. In the horse increased coat length and density is an acquired abnormality associated with equine hyperadrenocorticism.7 In ruminants defects are congenital and are the result of either an in utero infection (border disease) or a breed-specific hereditary defect.9,11
The differential diagnoses of decreased coat length and density are extensive. The initial step is to determine if the alopecia is congenital, implying a hereditary defect, or acquired. If the abnormality is acquired, the clinician must determine if it is a primary alopecia or secondary to another cutaneous abnormality such as pruritus or ulceration. If alopecia is the result of another primary cutaneous abnormality, the clinician should focus on the differential associated with that primary abnormality. Finally, to help provide a prognosis for hair regrowth, the clinician should biopsy to determine if the alopecia is scarring (cicatricial) or nonscarring (noncicatricial). Regardless of the underlying cause and its resolution, hair will not regrow with
■ BOX 11.6
Most Common Causes of Abnormal Coat Length and Density in Horses and Ruminants
Alopeciaa
Dermatophytosis
Staphylococcal pyoderma (horses) Alopecia areata (horses, cattle)
Drug reaction
Congenital hypotrichosis (cattle)
Onchocerciasis (horses)
Increased Coat Length
Pars intermedia pituitary dysfunction (horses) Congenital hypertrichosis
aAlopecia without pruritus, crusts, or other clinical signs.
a cicatricial alopecia because by definition the hair follicle has been destroyed. In a noncicatricial alopecia the potential for hair regrowth remains if the underlying cause for hair loss can be identified and resolved (Box 11.6).
The following steps are a guide to the diagnosis of decreased coat length and density in horses and ruminants:
1. History (see Fig. 11.1)
a. Determine whether the lesions are congenital or acquired. If they are congenital, determine if any related animals are affected and if the lesions have progressed since birth.
b. If the alopecia is acquired, determine if the animal is pruritic and if other cutaneous lesions have been observed.
c. Determine if the animal's diet is nutritionally complete.
d. Determine if the animal has been exposed to any toxic substances.
e. Determine if contact animals of the same and/or different species are affected. If contact animals are affected, a contagious problem such as dermatophytosis or der- matophilosis should be considered. Because feed and environment are also shared, dietary deficiencies and toxicities should be included in the differential diagnosis.
f. Determine what medications have been given systemically or applied topically to the patient. Use of certain topical agents, along with a history of an inflammatory stage preceding or coincident with the alopecia, may suggest a diagnosis of contact dermatitis. Administration of systemic medications may suggest that the cause is a drug hypersensitivity.
g. Determine if the animal has been subjected to any stresses that might provoke a telogen effluvium.
2. Physical examination (see Fig. 11.2)
a. Check for evidence of disease in organ systems other than the skin. Does the animal appear thin and malnourished, suggesting hair loss related to a dietary deficiency? Is it febrile or suffering from a severe systemic disease, suggesting a telogen effluvium?
b. Can the hairs be epilated readily from the coat? If not, hair loss may be caused by trauma (self-induced or external).
If so, underlying nutritional, hormonal, or stress-related causes of alopecia are more likely.c. Look for evidence of excoriation, suggesting that selftrauma is the cause of the hair loss.
d. Determine whether the lesions are generalized or localized, either to particular areas of the body or to certain hair colors (e.g., black hair follicle dystrophy). Note if the hair loss has a symmetric pattern.
e. Inspect the coat closely for small but grossly visible parasites such as lice or their eggs.
f. Inspect contact animals for evidence of disease.
3. Microscopic examination of the ends of affected hairs (squared or broken ends suggest that the hair loss is traumati- cally induced; tapered ends suggest an abnormality in the hair follicle, growth cycle, or an inflammatory process such as dermatophytosis)
4. Skin scrapings
5. Acetate tape preparations
6. Dermatophyte culture and KOH preparation
7. Microfilarial preparation
8. Biopsy for routine histopathologic examination (sagittal sections should be evaluated to determine the proportion of hairs in the various phases; for the presence or absence of inflammation and infectious organisms; and for evidence of scarring, which suggests a poor prognosis for hair regrowth; cross-sections of the biopsy specimen should be evaluated in noninflammatory alopecias to determine the number of hair follicles present per given area)
The following steps are a guide to the diagnosis of increased coat length and density in horses and ruminants:
1. Horses demonstrating increased coat length and density should be evaluated with appropriate laboratory tests for hyperadrenocorticism.
2. Lambs with increased coat length and density should be evaluated for evidence of border disease.
3. Cattle with increased coat length and density probably have hereditary hypertrichosis.