Assessment of the Mare During Late Gestation
The per-cycle pregnancy rate in mares has been reported between 60% and 69%, with increasing mare age, breeding at foal heat, and overuse of stallions reported as negative factors at one Thoroughbred stud.1 Approximately 79% and 87% of pregnancies detected at days 15 and 40, respectively, result in a live foal.2 With additional losses in the perinatal period, it has been estimated that between 22% and 40% of mares that are bred do not produce a live foal.2-5 Factors that contribute to this outcome include mare age, infertility, early fetal loss, abortion, and perinatal death.1,4 During late gestation, common causes of reproductive loss are fetoplacental infection, placental dysfunction, maternal illness, and complications of delivery.4,6,7 As mares age, their pregnancy and foaling rates decline and their foals experience higher morbidity and mortality rates and decreased athletic ability.1-3,5
The 2015 National Animal Health Monitoring System (NAHMS) reported that 3.3% of foals died within the first 48 hours after birth.
This compares to the 1998 and 2005 NAHMS studies, where mortality rates of 1.7% and a 2.6% were reported, respectively.8 This includes an estimate of euthanasia and spontaneous deaths. Sepsis, asphyxia, and dysmaturity, including prematurity and postmaturity syndromes, are the leading causes of neonatal foal mortality during the first 2 weeks of life.9 Despite advances in neonatal intensive care, many foals still die, not because their primary problem is untreatable, but because veterinary intervention was delayed, delivery was unattended, neonatal compromise was not recognized in a timely fashion, or critical care was unavailable or not economically feasible. Foals surviving severe peripartum illness often experience increased morbidity associated with chronic infections, suboptimal growth, or developmental orthopedic disease. The three periparturient events that have the most devastating effect on neonatal survival are hypoxia, infection, and derangement of in utero development.Many of the periparturient events associated with increased fetal/neonatal morbidity and mortality have been identified in the mare (Box 15.1).
There are several clinical indications for evaluating the late-term fetus, including a larger than expected maternal abdomen, premature lactation, vaginal discharge, maternal illness, or prolonged gestation.7 Mares that have a history of reproductive failure in late gestation are also candidates for close monitoring in future pregnancies. Biochemical and biophysical techniques for monitoring fetoplacental well-being have been developed for use in the pregnant mare.10-14 Mares with high-risk pregnancies should be identified early, treated appropriately, and monitored closely through the perinatal period. Accurate assessment of fetal well-being is complicated and handicapped by the size of the dam and fetus.
Mares experiencing problem pregnancies can be assigned to one of three categories: (1) mares with histories of abnormal pregnancies, deliveries, or newborn foals; (2) mares at risk for a problem with the current pregnancy due to systemic illness or reproductive abnormality; and (3) mares with no apparent risk factor, which experience an abnormal periparturient event.13 A list of important risk perinatal risk factors is presented in Box 15.2. Ideally, mares with high-risk pregnancies should receive some type of late-gestation fetal monitoring or at least be carefully watched during late gestation and attended at the delivery. Personnel attending the delivery of a high-risk foal should be trained in resuscitation techniques (see later).
The hormones associated with pregnancy and fetal well-being can be divided into several categories.15 These include hormones that control uterine myometrial activity, including quiescent and contractile states, and those that induce fetal maturation.
Progestagens, including progesterone and its metabolites, are important in maintaining uterine quiescence during pregnancy. Progesterone is produced by the ovary until days 120 to 150 of gestation. After this time progestagens are synthesized by the uteroplacental tissues from pregnenolone, which is derived from fetal adrenal glands.16 Pregnenolone is metabolized to■ BOX 15.1
■ BOX 15.2
Common Causes of Abortion, Stillbirth, and Perinatal Death in Horses
Infectious problems (in order of frequency)
Fetoplacental infection
Bacterial
Viral
Fungal
Unidentified
Noninfectious problems (in order of frequency)
Neonatal asphyxia not associated with dystocia
Neonatal asphyxia associated with dystocia Placental edema
Premature placental separation
Twin pregnancies Contracted foal syndrome Other congenital malformations Umbilical cord abnormalities Placental villous atrophy
Eastern Tent (Malacosoma americanum) or Processionary caterpillars (Ochrogaster lunifer) ingestion
From Giles RC, Donahue JM, Hong CB, et al: Causes of abortion, stillbirth, and perinatal death in horses: 3527 cases (1986-1991). J Am Vet Med Assoc 203:1170, 1993.
progesterone in the placenta, which is further converted to 5 α-pregnane,3,20,-dione (5 α-DHP) in the endometrium. 5 α-DHP is metabolized to other progestins in the fetus, while some is passed into the maternal circulation, where it can be measured using commercial progesterone assays, due to endogenous progestagen cross-reactivity with progesterone antibodies. Maternal progestagen concentrations are relatively low and stable between days 150 and 315 of gestation, with concentrations typically between 2 and 12 ng/mL, depending on the assay used. These values rise sharply over the final 15 to 21 days of the pregnancy, before a large fall in the last 1 to 2 days before parturition. The rise is associated with mammary gland development and changes in the electrolyte concentrations of mammary secretions.15
Monitoring progestagen concentrations can provide useful insight into fetoplacental abnormalities, although maternal changes typically lag the early stages of disease.
Measurement of progestagens may therefore be indicated to determine the need for progestin supplementation.17 Three abnormal progestagen patterns have been described, and multiple samples collected at 48- to 72-hour intervals are recommended in high-risk mares.18-21 Precipitous falls in progestagen concentration are seen in circumstances of fetal death and/or imminent expulsion.22 In acute maternal illnesses, such as colic or uterine torsion, the progestagen concentration declines hours to days before abortion. In these mares the concentration may fall to less than 2 ng/mL.21 A premature rise in the plasma progestagen concentration can occur in response to fetal stress and/or placental pathology and can persist for days or weeks before abortion or premature delivery.18 A premature increase in maternal progestagens could reflect hastened or precocious fetal maturation. Removal of the initiating stressful event can lead to normalization in progestagen concentrations and the subsequent delivery of a healthy full-term foal. A third abnormal maternal progestagen profile is found in mares exposed to tall fescue grass infected with an endophyte fungus, where there is a failure in the concentration rise seen in normal mares.Relaxin is a marker of fetoplacental well-being and periparturient complications in the mare.23 The placenta is the sole source of circulating relaxin in mares.24 In healthy pregnant mares, relaxin concentrations increase from about day 80 to
Conditions Associated With the High-Risk Foal
Maternal Conditions
Past history of:
Foals with neonatal isoerythrolysis, perinatal asphyxia syndrome, congenital malformations
Prematurely born, post-term foals that appear premature or asphyxiated foals
Dystocia or premature placental separation
Foal rejection
Recent exposure to infectious diseases associated with abortion and stillbirths, such as equine herpesvirus, viral arteritis, Leptospira spp.
Systemic problems such as:
Fever
Anemia or hypoproteinemia
Endotoxemia
Gastrointestinal crisis, such as large bowel torsion Malnutrition
Severe systemic infection
Laminitis
Prolonged recumbency from a variety of neurologic or musculoskeletal problems
Excessive medication administration
Prolonged transport before parturition
Reproductive, mammary gland, or localized problems, such as:
Severe endometrial fibrosis
Hydrops allantois or amnii
Purulent vaginal discharge
Prepubic tendon rupture
Pelvic injuries
Agalactia, such as from grazing on fescue pastures
Failure to produce good-quality colostrum Premature lactation
Abnormalities of Labor or Delivery in Current Pregnancy
Premature parturition
Abnormally long gestation
Prolonged labor
Induction of labor
Dystocia
Early umbilical cord rupture, umbilical cord abnormality Cesarean section
Premature placental separation
Neonatal Abnormalities
Meconium-stained fluid or neonate
Placental disease (e.g., placentitis, villous atrophy, edema) Twins
Orphan
Delay in or lack of intake of colostrum
Dysmaturity or prematurity
Exposure to infectious diseases, such as influenza
Trauma (birth, predators, mother)
Adverse environmental conditions
Failure to be up and nursing by 2 to 3 hours of age Congenital abnormalities
Weakness, poor appetite
a peak of 80 to 100 ng/mL at day 175, which persists until birth.25,26 There are breed differences in relaxin concentrations during normal pregnancy.27 A study of mares with normal pregnancies reported slightly lower values over the final 7 weeks of gestation.23 Plasma values drop at delivery and are cleared within 48 hours of passage of the fetal membranes. In mares with problematic pregnancies, low relaxin levels during late pregnancy have been indicative of placental insufficiency associated with a variety of causes including twinning, fescue toxicosis, oligohydramnios, placentitis, and pituitary disease.23 The variability in values and breed differences make it difficult to rely on relaxin concentration as a marker of treatment efficacy in problem pregnancies.23
Estrogens regulate contractile properties of the myometrium.
The precursors for estrogen formation are derived from fetal gonads, and metabolism takes place in the placenta. Precursors include estrone, estradiol-17α and estradiol-17β, and the equine-unique compounds equilin and equilenin.15 Removal of the fetal gonads does not affect gestational length, implying that estrogens are not required for maintenance of pregnancy. However, labor is lengthened, foals are growth restricted, and maternal concentrations of prostaglandin F are decreased. It is likely that a prepartum increase in estrogens is associated with increased prostaglandin production and increases in oxytocin receptors, similar to that of other species.15 Measurement of total maternal estrogens may reflect fetal health, with low concentrations associated with fetal compromise or death, but clinical data are lacking.Several studies have demonstrated that ultrasound-guided transabdominal and allantocentesis can be used relatively safely in the late-gestation mare as long as the procedure is performed aseptically and multiple attempts are not made.13,28,29 However, the clinical usefulness of fetal fluid analysis in the horse remains to be determined. Studies attempting to relate the phospholipid profile in amniotic fluid with equine fetal lung maturation have been inconclusive.13,30,31 Transabdominal-guided ultrasound amniocentesis has also been used to detect experimentally induced equine herpes virus (EHV-1) fetal infection in utero.32 The technique holds promise as a diagnostic aid to detect specific fetal diseases and as a potential therapeutic avenue to deliver medication in utero. Preliminary data demonstrated that mares that delivered healthy foals had a significantly higher amniotic fluid lactate concentration at the time of delivery than mares that delivered sick foals.33 The significance of this finding is not known.
Electrolyte concentrations in prepartum mammary secretions may be monitored to predict impending parturition in the mare. As parturition approaches, the mammary concentration of sodium decreases and concentrations of potassium and calcium increase. An elevation in calcium concentration to over 40 mg/dL (400 μg∕mL; 10 mmol/L) is a reliable indicator of readiness for birth and can be used to help determine whether elective induction or cesarean section should be performed. The increase in calcium occurs over the last 72 hours of gestation.34,35 Test strips are commercially available to measure calcium and magnesium concentrations in a field setting (Predict-A-Foal Kit [Animal Health Care Products, Vernon, Calif.] and FoalWatch Kit [Chemetrics, Calverton, Calif.]). The milk calcium test better predicts mares that are not likely to foal rather than accurately determining the timing of foaling.
There are increases in the mammary concentration of potassium and a decrease in the mammary sodium concentration over the final 7 days of the gestational period. The mammary concentration of potassium typically exceeds that of sodium between 1 and 5 days before foaling. This has been used by some as a predictor of birth, although a recent study concluded that the use of mammary electrolyte concentrations was not reliable due to individual variability in both raw concentrations and percent changes.36 The reversal of the milk sodium-to- potassium ratio was more accurate at predicting the day of birth than the milk calcium concentration in Martina Franc jennies, a breed that has longer mean gestational length.37 The ratio reliably reversed 48 to 24 hours before parturition.
An arbitrary scoring system using calcium, sodium, and potassium concentration in the mammary secretions to assess fetal maturity has been described.35 False-positive results (i.e., a value that inaccurately predicts imminent foaling) have been associated with vaginal discharge, placentitis, and premature
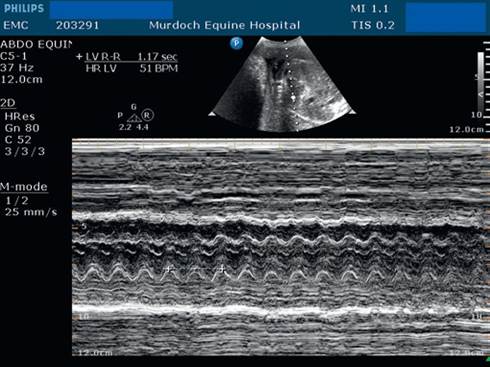
FIG. 15.1 M-mode assessment of a fetal heart to determine fetal heart rate. In this example the rate was calculated using two successive heart beats, resulting in a rate of approximately 102 beats per minute. (Courtesy Dr. Emma McConnell.)
lactation. False negatives occur commonly in mares with systemic illness or animals that have undergone general anesthesia. In many mares the changes in the electrolytes occur only within hours of delivery, so if monitoring is not performed frequently, the changes will be missed.36,38 Recently, a comparison was made among milk calcium carbonate concentration, refractometry index, and pH with respect to prediction of foaling in healthy Thoroughbred mares.39 Milk pH declines from a mean of approximately 7.4 to 6.4 over the final week of parturition. The positive predictive value (PPV) of foaling within 72 hours and the negative predictive value (NPV) of foaling within 24 hours for calcium carbonate concentration (using a water hardness test kit) were 93.8% and 98.3%, respectively. The PPV with 72 hours and NPV within 24 hours for mammary secretion pH (using pH paper 6.2 to 7.6) were 97.9% and 99.4%, respectively. Both techniques were superior to handheld refractometry. The authors used cutoff values of 400 μg∕g for calcium and 6.4 for pH. The decision on whether or not to induce parturition in a mare should not be based solely on the results of this type of testing.
Fetal heart rate (FHR) and fetal heart rate variability (FHRV) are useful tools to assess fetal well-being. The most commonly used technique for assessing FHR is M-mode echocardiography (Fig. 15.1). This requires access to suitable ultrasound equipment including a low-frequency probe and appropriate software. This technique does have several limitations, including difficulty in locating the fetal heart in some cases due to maternal and fetal movement. Also, the heart rate at any time point is influenced by fetal activity, and a single time point observation may not accurately reflect the upper and lower FHR extremes.40
A fetal electrocardiogram (ECG) can be used to assess FHR and FHRV after day 150 of gestation.40-44 The left arm electrode is placed on the dorsal midline of the mare at the lumbar region, and the left leg electrode is placed 15 to 20 cm cranial to the udder on the ventral midline. The hair should be clipped, and ample gel or alcohol should be placed to ensure good contact of the electrodes. Poor fetal signals may result from poor electrode contact or placement, fetal movement, or electrical interference. An alternative method involves placement of the left leg lead on the left neck, the left arm lead in the left flank at the height of the hip, the neutral lead on the mare's croup, and the right arm lead over the linea alba cranial to the udder and then connecting the leads to a Televet 100 Holter ECG (Engel Engineering Services GmbH, Heusen- stamm, Germany) recording system. This configuration allows for simultaneous determination of the maternal and fetal ECG. Calculation of the fetal HRV has merits but remains essentially a research tool. It requires acquisition of a minimum of 5 minutes of good-quality recording and export of an R-R interval file, which is then processed using a dedicated software product (Kubios HRV software [Biosignal Analysis and Medical Imaging Group, Kuopio, Finland]). From a practical perspective, gross examination of the beat-to-beat variability can be done using a standard ECG trace; an absence of variability is a concerning sign, assuming no maternal sedation.
The fetal heart rate peaks around 196 beats per minute at 3 months' gestation, before decreasing over the reminder of the gestational period.11 Heart rate decreases from greater than 120 beats per minute before day 160 of gestation to between 60 and 90 in late gestation.12,40-43,45,46 In late gestation FHRs below 60 bpm are common and are not of concern unless they persist and occur without accelerations.47 Conversely, rates greater than 120 bpm are also common in active foals and are normal unless they do not return to healthy baseline levels. Cardiac accelerations in response to fetal movement are an indicator of fetal well-being. An early study reported an average of 10 heart rate accelerations (25 to 40 beats per minute) in a 10-minute period; 95% of these were associated with fetal movement.48 Ahother study reported that the number and duration of cardiac accelerations and decelerations remained relatively constant over the last 2 months of pregnancy. There were approximately 22 accelerations per hour lasting around 29 to 42 heart beats and around 24 decelerations per hour lasting 24 to 60 heart beats.43
There is an increase in FHRV over gestation.43,46 HRV describes the variability in R-R intervals between successive beats and reflects the influence of the neuroendocrine system. A frequency-domain analysis, reported as a low frequency (LF)∕high frequency (HF) ratio, is an indicator of sympathetic activity and is used as a marker of stress. In stressful states the HF component decreases, producing a lower LF/HF ratio.43 Therefore a healthy state is typically associated with a high HRV40 The FHV and FHRV are relatively constant over the final 10 days of gestation and are not useful indicators of foaling.43
The fetal response to hypoxia is persistent bradycardia and a reduction in movement. If reduced oxygen delivery persists or worsens, tachycardia and arrhythmias result, again with an absence of movement. Ultimately myocardial exhaustion leads to a return of persistent bradycardia immediately before fetal death. Although persistent fetal tachycardia and bradycardia suggest fetal compromise, a normal FHR alone does not guarantee that the fetus is healthy. Prolonged periods of fetal inactivity, in the absence of maternal sedation, are also suggestive of poor fetal health.
Transabdominal ultrasonography allows noninvasive evaluation of the intrauterine environment and fetal well-being. In the mare, transabdominal ultrasonography can be used to evaluate the equine fetus after day 90, when the gravid uterus contacts the ventral abdominal wall. This technique is used more commonly during the second and third trimesters. After 9 months of gestation, most fetuses are in an anterior presentation and are unlikely to change that presentation before delivery.49
Transabdominal scanning has been used to detect twins, document fetal position, estimate fetal size using fetal aortic diameter, evaluate fetal activity, evaluate placental integrity, determine fetal fluid clarity and volume, and monitor FHR and fetal breathing. Phased array or convex transducers with lower frequencies (2 to 4 MHz) are required due to the deep tissue penetration needed (up to 25- to 30-cm depth). Higher-frequency probes provide a clearer assessment of the uteroplacental unit, with depths less than 10 cm typically required. The mare's ventral midline must be cleaned from the level of the umbilicus (xiphoid in late pregnant mares) caudally to the mammary gland, and isopropyl alcohol is applied with or without coupling gel. Clipping provides a better image but is usually not required. Chemical sedation should be avoided because drugs such as xylazine and detomidine induce fetal bradycardia and retard fetal movement. The abdomen should be scanned in both sagittal and transverse planes. The examination typically begins at the front of the udder, moving cranially to detect the characteristic shadowing of the fetal ribs (Fig. 15.2) The aorta is identified and measured as close to the heart as possible (Fig. 15.3). A fetal heart rate is typically calculated using M-mode ultrasound. The position of the foal is verified, and as discussed earlier, after 9 months' gestation the head is directed toward the pelvis and the fetus lies in dorsal recumbency with vertebrae closest to the ventral abdominal wall.12 Abnormal positioning after this time heightens the risk of dystocia. Fluid depths are assessed for both the allantoic and amniotic fluid compartments using multiple measurements from the lateral aspect of the ventral abdomen of the mare.14 The most prominent region of fetal fluid is around the thorax in the area of the elbows.12 In healthy mares the maximum depth of the allantoic fluid has been reported as 13.4 ± 4.4 cm, and the maximal depth of the amniotic fluid as 7.9 ± 3.5 cm. The amniotic membrane is a thin, hyperechoic structure that appears to float freely in between the amniotic and allantoic sacs.

FIG. 15.2 Characteristic rib markings overlying the thorax in a 5-month gestational age pony fetus.

FIG. 15.3 Measurement of the aortic diameter is ideally made close to the heart.
Biophysical profiles that use several parameters to establish an idea of the size and overall health of the equine fetus have been developed.10,11,14,45,48 There is evidence that these profiles are important in high-risk mare pregnancies50 but fall short of similar profiles in human medicine in predicting outcome.14,47 The six parameters typically assessed using transabdominal ultrasonography include fetal weight, as estimated by the fetal aortic diameter in relationship to the mare's weight (mean 2.1 cm at 300 days' gestation to 2.7 cm at full term), FHR (decreases with advancing gestational age), fetal activity (increases with advancing age; graded from 0 to 3), uteroplacental contact and thickness, and maximal amniotic and allantoic fluid depth. Similar to human biophysical profiles, a maximum score of 2 is given to each parameter if it is normal. Low scores predict poor outcomes, but high scores do not guarantee a healthy foal.
Qualitative assessment of the fluid appearance is also useful. The fluid within the allantoic and amniotic spaces is characteristically anechoic, although small floating particles can be observed in the allantoic compartment in late-term mares.45 During late gestation the equine fetus should demonstrate moderate activity (grade 2 to 3/3) with only brief episodes of inactivity (in a diffuse or multifocal placentitis.
Mares with ascending placentitis are typically pluriparous, and many have anatomic defects, including vestibule-vaginal reflux, pneumovagina, and damage to the cervix, including fibrosis, tears and adhesions.15 Most cases of placentitis are the result of bacterial infection caused by typical equine pathogens including Streptococcus equi subspecies zooepidemicus, Escherichia coli, Enterobacter agglomerans, Klebsiella pneumoniae, and Pseudomonas aeruginosa. In some regions a slightly different form of placentitis has been recognized and is characterized by focally extensive placentitis located predominantly at the base of the placental horns at the junction of the horns and body of the placenta.58 The affected area is covered with thick, tenacious brown mucoid exudate, and the underlying chorionic villi are necrotic and absent or reduced in size. This form is associated with infection by a group of gram-positive, branching, filamentous Nocardioform actinomycetes, including Crossiella equi, Amycolatopsis species, and less commonly Cellulosimicrobium cellulans and Streptomyces species.59 There is link between some of these bacteria, which are part of the normal intestinal flora, and ingestion of Eastern Tent caterpillars (Malacosoma americanum) or Processionary caterpillars (Ochrogaster lunifer).6'0'6i The Eastern Tent caterpillar is linked to Mare Reproductive Loss Syndrome (MRLS) in the United States, and the Processionary caterpillar is a causal agent of Equine Amnionitis and Fetal Loss (EAFL) syndrome in Australia.62 It is likely that the barbed setae (hairs) penetrate the intestinal mucosa, thereby facilitating bacterial translocation.
Chlamydophila (formerly Chlamydia) psittaci infects a wide range of wild bird and poultry species around the world. The organism has been documented as a cause of placentitis in mares with associated foal mortality.63 It has the potential to spill over into humans, with clusters of human cases documented after handling of diseased fetal membranes.63,64 The likely modes of transmission in these cases from fetal membranes to humans are either via the airborne route or direct inoculation of the eyes or nose. There is some limited evidence that respiratory protection (P3 mask) and eye protection reduces the risk of disease.65 The potential avian reservoir for equine chlamydiosis is not known, but a pigeon-like variant was isolated in New South Wales.66
Clinical signs of placentitis include vaginal discharge, premature udder development, and precocious lactation. The discharge may be evident on the vulva, tail, or inner thighs. Premature udder development is the result of placental compromise, fetal stress, a precocious increase in maternal progestagen concentration, and enhanced fetal adrenocortical activity. Despite even voluminous vaginal discharge, most mares with placentitis do not become febrile and do maintain a normal appetite. The dam's hematology and fibrinogen concentration usually remain within normal limits. Untreated mares with experimental placentitis due to S. equi subsp. zooepidemicus had significant increases in serum amyloid A (SAA) within 96 hours of inoculation that persisted through to birth or abortion.67 The increase in SAA was prevented in most treated mares.
Transrectal ultrasound is used to identify placental separation and utero-placental thickening of the caudal uterine body. This region is most commonly involved in mares with ascending placental infection. Measurement of the combined thickness of the uterus and placenta (CTUP) is established. The rectal transducer is placed at the cervical-placental junction, where a branch of the uterine artery is seen between the uterus and bladder. This measurement increases from around 4 to 6 mm at 7 months' gestation to 10 to 12 mm at term.45,51 Mare parity has an impact on CTUP during midpregnancy (100 to 250 days), with primiparous mares having a greater thickness than multiparous mares.68 The difference is lost in late pregnancy. A measurement greater than 12 mm at 9 months, or greater than 15 mm at 11 months, is consistent with placental pathol- ogy.45,69 Measurement of CTUP alone can be misleading, and monitoring of the CTUP by ultrasound along with determination of the maternal progestagen concentrations has been recommended.18 Fetal membranes commonly disunite from the uterus, separated by fluid of variable echodensity.
Transabdominal ultrasonography is used to evaluate other areas of the placenta to detect loss of placental integrity or increased uteroplacental thickening. Using transabdominal ultrasound, the uteroplacental unit should be less than 16 mm during late gestation. Other signs suggestive of placentitis include increased fetal fluid echogenicity, which might result from hemorrhage or purulent exudate. If placentitis is severe enough to alter placental function, reduced fetal movement, loss of heart rate variability, and absolute fetal bradycardia collectively indicate fetal compromise.
Samples of vaginal discharge should be cultured, and Gram stains should be performed. The goal of maternal therapy is to treat the placental infection and maintain the pregnancy, provided there is no evidence of severe fetal distress or demise. In many cases, because the infection is of long duration, the fetus has been chronically stressed and therefore is relatively mature for its gestational age and better prepared to tolerate preterm birth. If placentitis is suspected, following delivery, the foal should be considered a high-risk individual. Commonly encountered problems in the newborn foal that was exposed to placentitis are pneumonia, uveitis, growth retardation, incompletely ossified bones, and sometimes systemic sepsis.