Background Information of Clinical Importance
Anatomy
The comparative anatomy of the ruminant urinary tracts has been reported (Nickel et al. 1973; Sisson 1975; Barone 1978). The paired kidneys of the goat are smooth, elliptically bean shaped, and located retroperitoneally in the abdomen.
They are normally surrounded by perirenal fat, more abundantly so on the left. The location of the right kidney is fixed in the dorsal abdomen, occurring at the level of vertebrae T13 to L3. The left kidney is located more caudally at L4 to L5, with its lateral aspect in contact with the dorsal sac of the rumen. It is frequently pushed to the right of the abdominal midline by a full rumen. Adult
Figure 12.1 Urethral process of the buck extending beyond the glans penis. Source: Reproduced by permission of Dr. C.S.F. Williams.
Urinary calculi are commonly trapped in the urethral process, causing obstruction of urine flow. This is particularly true in males castrated early, where the urethral diameter may be reduced and the urethral process remains adhered to the preputial mucosa because of loss of the developmental effects of testosterone. The urethral process is commonly removed as part of the medicosurgical management of obstructive urolithiasis to restore urine flow. There is no evidence that removal of the urethral process impairs fertility in goats.
Male goats possess a urethral recess projecting caudodor- sally from the spongy portion of the urethra in the region of the ischial arch (Figure 12.2). The paired bulbourethral glands empty their secretions into this recess, which is 0.5 cm deep. In earlier descriptions, the urethral recess was referred to as the urethral diverticulum (Hinkle et al. 1978; Garrett 1987). This structure assumes clinical importance in attempts to catheterize the urethra retrograde to the bladder during clinical management of obstructive urolithiasis.
As the catheter moves dorsally up the urethra in the perineal region and begins to arch cranially over the pubis, the tip invariably becomes lodged in the urethral recess and will not pass to the bladder. Ignorance of the presence of the recess may lead to forceful manipulation of the catheter to reach the bladder. This can cause tearing of the urethral recess, with subsequent accumulation of urine in perineal tissues or trauma, scarring, and contracture of the urethra. In a controlled study in intact male goats, angiographic catheters with a bend at the tip were more successfully and consistently passed retrograde into the bladder without engaging the urethral diverticulum than were straight-tipped catheters (Reppert et al. 2016).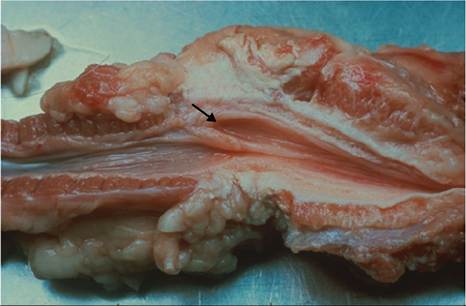
Figure 12.2 Urethral recess (arrow) of the buck at the ischial arch. Source: Reproduced by permission of Dr. C.S.F. Williams.
In contrast to the male urethra, the female urethra is short and straight. The external urethral orifice is on the floor of the vestibule, inside the vulva. There is a suburethral diverticulum inside the external urethral orifice, ventral to the urethra, which must be avoided for successful catheterization of the bladder. The doe has no vestibular glands.
Physiology
As in other species, the kidney serves multiple functions, including water and electrolyte balance, nutrient conservation, maintenance of normal blood pH levels, and regulation of nitrogenous wastes. The kidney also has endocrine functions. It responds to antidiuretic hormone (ADH) for control of water balance, aldosterone for sodium and potassium regulation, and parathyroid hormone to increase excretion of phosphorus. It also produces erythropoietin for stimulation of erythropoiesis, participates in the activation of vitamin D, and produces renin in response to decreased renal perfusion to activate angiotensin. Limited physiologic data reported for the goat is provided in Table 12.1.
The excretion of inulin, creatinine, sodium sulfanilate (SS), and phenolsulfonphthalein (PSP) has been evaluated to assess caprine renal function (Brown et al. 1990). Creatinine clearance was determined not to be a reliable measure of glomerular filtration rate (GFR) in goats, primarily because of the existence of a tubular secretory mechanism for creatinine excretion in this species. Clearance of SS exceeds inulin clearance because of the existence of a secretory mechanism for SS in the proximal portion of the nephron. In addition, SS may be eliminated by routes other than the kidney in the goat. The clearance of PSP also exceeds inulin clearance, presumably because of excretion of PSP by both glomerular filtration and tubular secretion.
Even though SS and PSP clearances from plasma are not exact measurements of GFR, the use of these tests to assess renal function is attractive, in that urine samples are not required to interpret results. This is important in goats, because collecting urine by catheterization can be problematic, especially in males.
Maturation of the caprine kidney may affect functional studies. The efficiency of renal function is relatively low in the newborn kid, but reaches adult capacity by 2 weeks of age, as indicated by increases in GFR and clearance of p- aminohippurate (Friis 1983). Tubular function increases more than glomerular function postnatally.
Goats show marked adaptation to conditions of poor nutrient availability and lack of water. Desert breeds such as the black Bedouin goat have a superior ability to
| Parameter | Type of goat | Special conditions | Unit of measurement | Reported value | Reference |
| Aldosterone in plasma | Adult Bedouin | Normal hydration | ng% | 5.5 ± 4.3 | Wittenberg et al. (1986) |
| Adult Bedouin | Water deprived | ng% | 13.9 ± 2.3 | Wittenberg et al. (1986) | |
| Clearance of creatinine | Young adult, mixed breed | Normal, conscious | mL/min/kg bw | 1.97 ± 0.09 | Brown et al. (1990) |
| Clearance of inulin | Young adult, mixed breed | Normal, conscious | mL/min/kg bw | 2.26 ± 0.08 | Brown et al. (1990) |
| Clearance of Phenolsulphonphthalein | Young adult, mixed breed | Normal, conscious | mL/min/kg bw | 6.88 ± 0.39 | Brown et al. (1990) |
| Clearance of sodium sulfanilate | Young adult, mixed breed | Normal, conscious | mL/min/kg bw | 3.71 ± 0.39 | Brown et al. (1990) |
| Effective renal plasma | General | - | mL/min/m2 | 493 | Fletcher et al. (1964) |
| flow (ERPF) | Adult Bedouin | Fully hydrated | mL/min | 344±146 | Wittenberg et al. (1986) |
| Filtration fraction | General | - | - | 0.18 | Fletcher et al. (1964) |
| Glomerular filtration rate | General | - | mL/min/m2 | 86 | Fletcher et al. (1964) |
| (GFR) | Not specified | 1-3 days of age | mL/min/kg bw | 2.1 ± 0.6 | Friis (1983) |
| Not specified | 14-20 days of age | mL/min/kg bw | 3.3 ± 0.2 | Friis (1983) | |
| Not specified | 69-78 days of age | mL/min/kg bw | 2.8 ± 0.5 | Friis (1983) | |
| Adult Bedouin | Normal diet | l/day/kg bw | 4.85 ± 0.3 | Silanikove (1984) | |
| Adult Bedouin | Low-protein diet | l/day/kg bw | 2.26 ± 0.1 | Silanikove (1984) | |
| Adult Bedouin | Fully hydrated | mL/min | 76 ± 29 | Wittenberg et al. (1986) | |
| Adult Saanen | Normal diet | l/day/kg bw | 6.61 ± 0.4 | Silanikove (1984) | |
| Adult Saanen | Low-protein diet | l/day/kg bw | 4.14 ± 0.3 | Silanikove (1984) | |
| Maximum tubular reabsorption rate (Tmax) | General | - | mg/min/m2 | 248 | Fletcher et al. (1964) |
| Urine chloride | Adult Saanen | Normal diet | mEq/L | 209 ± 55 | Silanikove (1984) |
| Adult Saanen | Low-protein diet | mEq/L | 366 ± 37 | Silanikove (1984) | |
| Urine creatinine | General | - | mg/kg/day | 10 | Brooks et al. (1984) |
| Urine flow | General | - | mL/day/kg bw | 10-40 | Brooks et al. (1984) |
| Adult Bedouin | Normal diet | mL/day/kg bw | 16.7 ± 3.7 | Silanikove (1984) | |
| Adult Bedouin | Low-protein diet | mL/day/kg bw | 2.4 ± 0.07 | Silanikove (1984) | |
| Adult Bedouin | Fully hydrated | mL/min | 0.74 ± 0.4 | Wittenberg et al. (1986) | |
| Adult Saanen | Normal diet | mL/day/kg bw | 26.3 ± 5.9 | Silanikove (1984) | |
| Adult Saanen | Low-protein diet | mL/day/kg bw | 4.8 ± 0.26 | Silanikove (1984) | |
| Urine osmolality | Adult Saanen | Normal diet | mOsm/kg | 1745±183 | Silanikove (1984) |
| Adult Saanen | Low-protein diet | mOsm/kg | 1523±171 | Silanikove (1984) | |
| Adult East African | Water deprivation | mOsm/kg | 2800-3000 | Maloiy (1974) | |
| Urine potassium | Adult Saanen | Low-protein diet | mEq/L | 342 ± 55 | Silanikove (1984) |
| Adult Saanen | Normal diet | mEq/L | 528 ± 47 | Silanikove (1984) | |
| Urine sodium | Adult Saanen | Normal diet | mEq/L | 135 ± 32 | Silanikove (1984) |
| Adult Saanen | Low-protein diet | mEq/L | 46 ± 31 | Silanikove (1984) | |
| Urine urea | General | - | mg/kg/day | 230 | Brooks et al. (1984) |
| Adult Saanen | Normal diet | mM/L | 968 ± 84 | Silanikove (1984) | |
| Adult Saanen | Low-protein diet | mM/L | 241 ± 39 | Silanikove (1984) |
bw, bodyweight.
conserve urea under adverse dietary conditions. In comparative studies with Swiss Saanen goats, both breeds could significantly increase the tubular reabsorption of urea when fed low-protein diets, but the Bedouin goat possessed a superior capacity to reduce GFR, thus lowering the amount of urea filtered by the kidney (Silanikove 1984). Urea thus conserved is available to the rumen microflora for protein anabolism via secretion in saliva.
Typically, desert goats may go without water for two to four days. When offered water, they can consume as much as 40% of their dehydrated bodyweight at one time. The rumen and kidneys work in concert to conserve water so consumed. Five hours after drinking, more than 80% of water taken in remains in the rumen. Effective renal blood flow, GFR, and urine output drop markedly, and urine flow remains below levels recorded in dehydrated goats, even four hours after drinking. At the same time, urine sodium concentration drops to half of that observed in dehydrated goats. There is a concomitant drop in urine potassium and chloride concentrations. Thus, the rumen acts as a water reservoir that is protected by renal conservation of sodium, chloride, and water (Choshniak et al. 1984; Wittenberg et al. 1986; Shaham et al. 1994).
Cold exposure causes goats to reduce their water intake. In lactating goats, there appears to be no compensatory reaction by the kidney and circulating ADH levels remain similar to those of goats in a thermoneutral environment. The net result is a decrease in milk production as a method of water conservation (Thomson et al. 1980). When goats are exposed to heat stress and/or deprived of water, circulating ADH levels increase and the kidney actively participates in water conservation (Olsson and Dahlborn 1989; Mengistu et al. 2007). In one study, excretion of ADH in the urine increased eightfold after 48 hours of dehydration (Lishajko and Andersson 1975).
Diagnostic Methods and Clinical Pathology
Examination of the Penis
Clinical management of obstructive urolithiasis requires examination of the penis. This can be difficult for several reasons. Cases often involve a young, castrated male with a small, poorly developed penis and residual adhesions between the penis and prepuce, making it difficult to manually extend the penis from the sheath. Obstructed goats are often in pain and resist manipulation. Sedation can assist in examination, but must be used cautiously when animals are severely uremic.
A common approach to examination is to sit the animal on its rump, which pushes the penis forward in the sheath. The penis is then grasped just behind the sigmoid flexure and pushed forward until the glans and free portion of the penis breach the preputial orifice. The free portion of the penis is then wrapped securely, but carefully, with a length of gauze to pull the penis farther forward and immobilize it. Use of the gauze helps to resist the opposing action of the retractor penis muscles. Successful examination in this manner usually requires at least one assistant, especially if partial catheterization is to be attempted. This technique can also be applied with the goat in lateral recumbency. In this case the goat may be easier to restrain, but it may be more difficult to achieve extension of the penis.
An alternative method for exteriorizing the penis is to position the goat on its back, with an assistant pulling both the animal's hindlimbs forward as close to its ears as possible. This straightens the penis and controls kicking. The technique works better with intact male goats than with wethers, where the penis may be adhered to the prepuce (Pieterse 1994).
In cattle and sheep, the internal pudendal nerve block, though sometimes considered difficult to perform, is used for anesthesia of the penis and relaxation of the retractor penis muscle to facilitate clinical manipulation (Hofmeyr 1987). While the internal pudendal nerve also controls the retractor penis muscle in goats, the nerve block may not produce the desired effect, because the preputial muscles are under separate neurologic control and their persistent contraction may still inhibit protrusion of the penis (Prakash and Kumar 1983). Alternatively, epidural anesthesia administered at the lumbosacral junction can be used to facilitate examination, but the concomitant loss of locomotor function may complicate patient management.
Chemical restraint and tranquilization are useful adjuncts to examination. Diazepam given intravenously at a total dose of 5-15 mg provides patient relaxation and lowers resistance to manipulation. Xylazine at a dose of 0.05mg∕kg bw intravenously provides similar effects. Xylazine should be used with caution in obstructed goats. The drug elevates blood glucose, thereby promoting diuresis. Increased urine production is undesirable if the obstruction is not successfully relieved. Acepromazine maleate at 0.1 mg/kg intravenously may promote relaxation of the retractor penis muscle, but the results are variable and the potential for phimosis exists. Propryonylpromazine at a dose of 1 mg/kg intramuscularly facilitated protrusion of the penis of goats in lateral recumbency, but spontaneous protrusion from the sheath did not occur (Schontag 1984).
Once the penis has been exteriorized, partial catheterization of the urethra may be attempted when indicated. This is made easier by amputation of the urethral pro - cess, but passage through the sigmoid flexure is still problematic. The urethral recess at the level of the ischial arch makes introduction of the catheter into the bladder practically impossible. These constraints should be recognized to avoid unnecessary effort and trauma. Retractor penis myotomy performed at the median raphe 5 cm ventral to the anus may allow maximal st.ra.ight.en- ing of the penis to assist in getting the catheter past the sigmoid flexure. Normal penis function was reported after reapposition of the muscles and healing (Shokry and Al-Saadi 1980).
Urine Collection
In cattle and sheep, urination can be induced by manual stimulation of the prepuce (male cattle) or skin in the perineal region (cows) or by holding of the nostrils (sheep). None of these techniques is effective in goats. Male goats may urinate frequently during the breeding season as part of mating behavior, but patience is a virtue when waiting for a urine sample from a doe. Goats often urinate immediately after rising from extended recumbency, so the sampler should be prepared with a urine cup at appropriate moments. Introducing the goat to a new pen or stall may promote urination, but this is unreliable. If able, bucks typically urinate after release from restraint for examination.
Catheterization of the female for urine collection is simpler than in the male so long as the suburethral diverticulum at the external urethral orifice is avoided. A 12 French catheter can be used in an adult doe. Experience in other species suggests that administration of bethanechol, a parasympathomimetic drug, at a dose of 75 pg/kg subcutaneously may stimulate urination in goats and not alter the composition of the urine.
For continuous collection of urine, pediatric urine bags have been sutured to the perineal region of female goats and a harness constructed to hold the collected urine (Mount 1984).
Clinical Chemistry and Urinalysis
Normal blood urea nitrogen (BUN) levels are in the range of 10-28 mg/dL, normal creatinine levels from 0.9 to 1.8 mg/dL, and normal uric acid levels from 0.33 to 1 mg/ dL. Breed, sex, and age variations in these normal parameters have not been identified in goats.
Measurement of gamma glutamyl transferase (GGT) in urine is being used in other species as an indicator of renal damage in the proximal tubular epithelium. There is one report of its application in goats. In a study on the nephrotoxic effects of the plant Narthecium ossifragum on goats in Norway, normal control goats had a mean urine GGT concentration of 18.8 U/L, with a range of 10-25 U/L, and a urine alkaline phosphatase concentration of 11.8 U/L, with a range of 5-19 U/L (Wisloff et al. 2003).
General values for urinalysis in the goat are given in Table 12.2. Breed, sex, and age variations are not reported for urinalysis in normal goats. However, urine osmolarity
Table 12.2 Normal caprine urinalysis values.
| Parameter | Normal value |
| Color | Pale yellow |
| Turbidity | Clear |
| Specific gravity | 1.00-1.050 |
| pH level | Alkaline (7.2-8) |
| Glucose | Negative |
| Ketones | Negative |
| Bilirubin | Negative |
| Occult blood | Negative |
| Protein | Negative to trace |
| Sediment (observed per high- powered field) | |
| Red blood cells | occasionally reveal cystic calculi (Figure 12.3). Contrast studies are often more helpful. Intravenous pyelography in the goat has been described (Cegarra and Lewis 1977). Sedation with xylazine facilitates the procedure. Ideally, goats should be fasted for 48 hours to reduce rumen size, but this can be detrimental to sick goats. Sodium iothalamate is given at a dose of 2 mL/kg intravenously in goats up to 28 kg, while in heavier goats the calculated dose is reduced to 75%. The kidneys are opacified within 20 seconds of injection and the entire urinary tract opacified within 15 minutes. The technique is helpful in identifying congenital renal abnormalities and the presence and extent of uroliths, especially in the bladder. Cystourethrography in the goat has also been described, requiring catheterization of the bladder under fluoroscopic guidance. The technique has proven useful for establishing the presence and character of cystic calculi (van Weeren
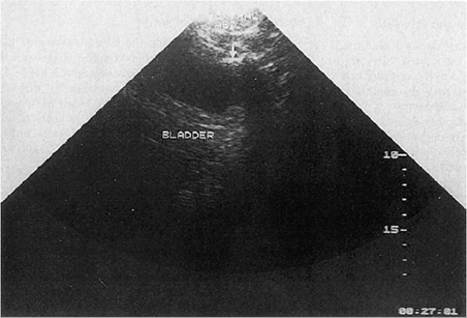
Figure 12.3 Multiple urinary calculi present in a goat urinary bladder as seen by plain radiography. This is an unusually diagnostic film. Contrast studies are often required to identify cystic calculi. Source: Courtesy of the Cummings School of Veterinary Medicine at Tufts University. et al. 1987b). A triple contrast cystography technique, with the addition of pneumoperitoneum, has also been described for use in the goat and is recommended for detailed evaluation of the mucosal surface of the bladder (Tayal et al. 1984). In a review of 26 cases of obstructive urolithiasis, including 20 goats, positive normograde cystourethrography through a tube cystostomy catheter offered the best visualization of the lower urinary tract structures for assessing and subsequently managing the obstructive lesion (Palmer et al. 1998). In that same review, survey radiographs obtained in 23 patients with obstructive urolithiasis were diagnostic for urinary calculi in only one animal. Ultrasonography has proven to be a rapid, useful technique in the diagnosis of urinary tract disease. Cystic calculi are readily identifiable by ultrasound and the technique is more reliable than survey radiography (Figure 12.4). An illustrated discussion of ultrasound techniques used for examination of the urinary tract in small animals is very applicable to the goat (Widmer et al. 2004). Kidney Biopsy Percutaneous biopsy of the right kidney can be accomplished in some goats. The right kidney is readily palpable in the abdomen of thin goats in the anterior portion of the
Figure 12.4 Urinary calculi (arrow at top of picture) in a goat urinary bladder as seen by ultrasound. Source: Courtesy of the Cummings School of Veterinary Medicine at Tufts University. right paralumbar fossa, just medial to the last rib. It can be captured manually, retracted caudally, and held in a fixed position in the right paralumbar fossa during the biopsy procedure. A Vim-Silverman needle is used for the procedure. A series of 300 right kidney biopsies was performed in this manner in thin Angora goats, with bleeding complications noted in under 1% of the goats. This procedure would be more difficult in larger, well-fleshed goats. In dogs, it is reported that kidney biopsies obtained with laparoscopy are of higher quality than those obtained with ultrasound guidance in terms of the number of intact glomeruli in the biopsy specimen (Rawlings et al. 2003).
Source:
Smith Mary C., Sherman David M.. Goat Medicine. 3rd edition. — Wiley-Blackwell,2023. — 976 p.. 2023
More on the topic Background Information of Clinical Importance:
-
Veterinarian -
|