Bacterial Diseases
Listeriosis
Listeriosis is an important zoonotic bacterial infection of mammals, birds, and other animals caused by Listeria monocytogenes. In goats, it is most commonly associated with neurologic disease, but can also cause septicemia and abortion.
The organism can be shed in the milk of healthyappearing carrier goats as well as in the milk of sick goats. Listeriosis is recognized as a serious disease in people and the potential of transmission of L. monocytogenes to humans from milk, cheese, and other dairy products is a growing concern, particularly when milk is unpasteurized. The elderly, pregnant women, newborns, and the immunocompromised are especially at risk.Etiology
L. monocytogenes is a motile, aerobic, and facultative anaerobic, small, Gram-positive rod. Colonies produce a narrow zone of beta hemolysis on blood agar. It is capable of growth over a wide pH range of 5.5-9.6 and a temperature range of 3-45 °C (37.5-113 °F), but optimal growth occurs at pH 7-7.2 and a temperature range of 20-40 °C (68-104 °F). Isolation of the organism from tissues and organic materials such as animal feeds can be difficult, so dispersion of tissues in a blender, cold enrichment of samples, subculturing from tryptose phosphate enrichment broth, and use of selective media such as trypaflavine nalidixic acid serum agar have been recommended (Dijkstra 1984a). Newer selective plating media are now available, including polymixin acriflavine LiCl cetazidime esculin mannitol (PAL-CAM) and Oxford agar, which isolate Listeria on the basis of esculin hydrolysis, as well as chromogenic media, which allow rapid visualization of Listeria colonies and differentiation of L. monocytogenes and Listeria ivanovii from other Listeria spp. PCR, targeting the hly gene, has been demonstrated to be a sensitive and rapid technique for confir - mation of the identification of suspect L.
monocytogenes isolated on selective/differential agar plates (Gouws and Liedemann 2005).L. ivanovii is considered non-pathogenic to humans but is pathogenic for mice and has been associated with abortions in sheep and cattle (Low and Donachie 1997). In one report, abortions due to L. ivanovii occurred in sheep in a mixed sheep and goat flock, but the goats were not affected (Santagada et al. 2004).
Though easily killed by common disinfectants, L. monocytogenes can survive in feces, silage, and tissue for five or more years (Dijkstra 1984b). There are now 16 known serotypes with numerous subtypes. Serotype 4, especially type 4b, and to a lesser extent serotype 1 have been associated with encephalitis and septicemia in goats. Abortion is associated primarily with serotype 1 (Deligaris et al. 1975; Kummeneje 1975; Loken et al. 1982a; Dijkstra 1984c). In one outbreak of listeriosis in goats, the same serotype, 4b, was recovered from goats with encephalitis and from goats with abortion (Wiedmann et al. 1999). It was hypothesized that transmission in this herd outbreak was by the venereal route. Serotypes 1/2a, 1/2b, and 4b are the serotypes most commonly isolated from human cases of listeriosis and from livestock cases.
Because L. monocytogenes is widely distributed in nature, characterization of environmental isolates by serotyping or phylogenetic analysis is necessary to confirm the association with disease outbreaks. Techniques such as ribotyping, pulse field gel electrophoresis (PFGE), and PCR have become useful tools of molecular epidemiology to improve understanding of the ecology and transmission of L. monocytogenes on farms and in food-processing facilities, and to track the origin of pathogenic strains associated with food- borne outbreaks of listeriosis (Sauders et al. 2003). There is growing evidence that strains of the organism are not host specific and that food animals and farms may serve as a reservoir for strains of L. monocytogenes that can lead to human infections (Nightingale et al.
2004; Okwumabua et al. 2005). Additional information on the various procedures and protocols currently in use for the identification of Listeria spp. in food products is available in the OIE Manual of Diagnostic Tests and Vaccines for Terrestrial Animals (OIE 2018f).Epidemiology
As many as 40 species of birds and mammals, including humans, can be infected with L. monocytogenes and the organism has been isolated on six continents. Listeriosis is a well-known, sporadic clinical problem in intensively managed dairy goats in North America and Europe. In France, 4.9% of fecal samples from sheep and goats in 98 flocks yielded L. monocytogenes (Nicolas et al. 1974). A seroepidemiologic study in Spain identified infection in 5% of goat herds tested (Perea-Remujo et al. 1984). Caprine listeriosis has also been reported from Japan (Asahi et al. 1954), South Africa (Du Toit 1977), Australia (Baxendell 1980), India (Phadke et al. 1979; Chattopadhyay et al. 1985), Brazil (Rissi et al. 2006), and Turkey (Borku et al. 2006). In New Zealand, it was reported as the most common neurologic disease of goats identified at necropsy (Thompson 1985).
Factors predisposing to clinical listeriosis in goats are similar to those reported for other farm animals and include sudden changes in weather, feeding regimens, or general management procedures; confinement in winter, particularly if overcrowded and with poor sanitation; increased stress from poor nutrition, parasitism, or other concurrent disease; advanced pregnancy; and the feeding of silage, particularly poor-quality silage. The feeding of silage is often emphasized as a key predisposing factor in ruminant listeriosis (Morin 2004). However, a history of silage feeding is not a prerequisite in outbreaks of caprine listeriosis (Wood 1972; Du Toit 1977). The author (DMS) has been engaged in several outbreaks of encephalitic listeriosis in goats in which there was no history of silage feeding. Johnson et al. (1996) reported on the occurrence of encephalitic listeriosis in goat herds in Missouri.
None of the herds in which the disease was diagnosed had access to silage; all of the affected herds had woody browse as their main source of feed; and Angora goats were the most commonly affected breed.An increased occurrence of listeriosis in fall and winter has also been observed in goats, though cases can occur year-round. The disease is most common in adult goats. Based on experimental challenge studies, goats are more susceptible to L. monocytogenes infection than are sheep (Gupta et al. 1980). A survey from Greece based on microbial cultures of brains from animals with neurologic signs of disease also found that goat herds were affected with encephalitic listeriosis more frequently than sheep flocks, with serotype 4b being predominant (Giannati-Stefanou et al. 2006).
The source of infection in herds is not always clear. Wild mammals and birds may be original sources of the bacteria, which then persist in soil and on plants. Goats exposed to such soil and crops may become latent carriers. During periods of stress they may become clinically ill, or shed large numbers of organisms in the feces, spreading the infection to other goats, particularly under intensive rearing conditions. Purchase of latent carrier animals may introduce the infection into previously naive herds.
Active proliferation of the bacteria in silage occurs in silage-associated outbreaks, resulting in heavy challenge to animals eating the material. Proliferation of bacteria is enhanced by poor silage quality, with pH levels above 5. In one caprine outbreak, pieces of a pheasant were found chopped into the silage and the tissues of the bird were positive for L. monocytogenes (Dijkstra 1984c). In addition to the presence of the bacteria, the feeding of silage has been shown to have some intrinsic immunosuppressive effect in sheep, leading to decreased circulating lymphocyte numbers and reduced serum total protein. This may additionally aggravate susceptibility to Listeria organisms present in the feed.
Recent studies have identified some differences in the ecology and transmission of L. monocytogenes on cattle farms compared to sheep and goat farms in upstate New York. Cattle farms had a higher level of environmental contamination with L. monocytogenes than did small ruminant farms, whether the cattle had a history of clinical listeriosis (case farms) or not (control farms). When small ruminant case farms were compared with bovine case farms, isolation of L. monocytogenes in small ruminant fecal samples was significantly less common than in bovine fecal samples. However, the organism was significantly more common in feed samples from small ruminant case farms than from bovine case farms, indicating that listeriosis on goat and sheep farms is more likely transmitted via feed than via feces. On all farms, soil samples were positive more commonly than were feed samples, indicating that soil is an important source of feed contamination with L. monocytogenes.
These findings suggest that small ruminants are less likely to appreciably amplify ingested L. monocytogenes than are cattle (Nightingale et al. 2004). In a related study (Nightingale et al. 2005), it was noted that the prevalence of L. monocytogenes on small ruminant farms peaked during the winter and the prevalence of L. monocytogenes in all samples collected from small ruminant farms was notably lower during the summer and fall. The number of healthy animals on cattle and small ruminant farms that were shedding L. monocytogenes in feces was most affected by season, with the prevalence of fecal shedding peaking in the winter and spring. Confinement housing and the quality of feeds fed in winter were believed to contribute to this pattern.
While direct transmission of L. monocytogenes from animals to humans can occur, it is uncommon. In such cases, human symptoms are usually limited to localized cutaneous infections. Much more common is the transmission of the infection to humans via foods of animal origin.
Zoonotic infection from goat milk and goat milk products is a very real concern. L. monocytogenes can be shed in the milk of clinically affected goats as well as in the milk of normal-appearing latent carriers with subclinical mastitis (Delhalle et al. 2012; Addis et al. 2019). Shedding is less likely in the encephalitic form of the disease than in the septicemic or abortion forms. In latent carriers, the intensity of shedding is increased toward the end of gestation (Gr0nst0l 1984). L. monocytogenes has resisted pasteurization at 61.7 °C (143 °F) for 35 minutes, but is killed by high-temperature short-time pasteurization at 71.6 °C (160.9 °F) for 15 seconds. The intraleukocytic location of some of the organisms in milk presumably contributes to this pasteurization resistance (Blenden et al. 1987). Experimentally, the organism has been reisolated from semi-soft, aged, goat milk cheeses made from unpasteurized, L. monocytogenes-inoculated goat milk as long as 18 weeks after preparation (Tham 1988). The organism has been isolated from pasteurized, fluid goat milk (Roy 1988) and raw goat milk (Willis et al. 2017) retailed in the United Kingdom. In a study in Sri Lanka, L. monocytogenes was recovered from raw goat milk, standard pasteurized milk, and cheese, but not from sterilized milk, ultra-high temperature (UHT) milk, yogurt, or curd (Jayamanne and Samarajeewa 2001). L. monocytogenes also was identified in traditional, homemade, fresh goat cheeses in Morocco (El Galiou et al. 2015).Not all listerial contamination of processed dairy products has the original milk as its source. Cross-contamination or recontamination after pasteurization can occur in processing plants if the strictest sanitation and hygiene are not observed. It is known that L. monocytogenes readily produces biofilms, which are microbial communities that strongly adhere to underlying surfaces. Biofilms can persist on processing equipment that is not scrupulously cleaned and disinfected. This can also occur on the farm, in that biofilms on milking machines can be a recurring source of contamination of bulk tank milk (Zundel et al. 2003). In a survey of 405 goat dairies in Spain, 2.56% of bulk tank samples were positive for L. monocytogenes. The isolates were most common in samples taken in the fall and winter and were rare in spring and summer (Gaya et al. 1996).
When goats have the septicemic or abortion form of listeriosis, the organism may be present in large numbers in feces, milk, birth fluids, placenta, fetuses, and newborn kids. Given the zoonotic potential of these materials for veterinarians and animal caretakers, appropriate precautions should be taken against infection when handling such tissues.
Pathogenesis
In the encephalitic form of listeriosis, the organism gains entrance to nerve endings in the oral cavity via breaks in the oral mucosa caused by coarse food, dental abrasions, or the loss of deciduous teeth. It then migrates up the nerves to the brain stem, where it stimulates a localized inflammatory response in the form of microabscesses comprised primarily of neutrophils. It is believed that L. monocytogenes primarily induces a cell-mediated immune response in the host and the severity of the resulting lesions may be mediated by the degree of immune recognition of the organism. Microabscesses are most common in the medulla and lead to destruction of cranial nerve nuclei, notably nerves V through IX. The cranial nerve deficits seen clinically reflect this process. Occasionally, generalized meningitis can occur in addition to focal encephalitis. The incubation period in the encephalitic form may be two to three weeks.
In the septicemic form, the incubation period may be as short as one day. The organism is believed to gain entry through the intestinal mucosa. There is an initial bacteremia with fever. This may be followed by recovery, development of a latent carrier state, or progression to more severe clinical disease. Because the morbidity rate is often low in outbreaks of septicemic listeriosis, it is presumed that many animals handle transient bacteremia effectively and are only subclinically infected. When animals do become ill, they may die within 48 hours or the illness may last for several weeks. Pregnant does abort several days after the initial fever and aborted fetuses also show evidence of septicemia. Septicemic goats may excrete the organism in feces and milk during and after clinical illness. Newborn kids exposed to the colostrum or milk of infected does can show signs of septicemia in the first few days of life. Seroconversion is marked in goats after septicemic listeriosis, but mild in goats after encephalitic listeriosis (L0ken and Gr0nst0l 1982).
Ocular forms of listeriosis are also reported in cattle and sheep (Morin 2004). Keratoconjunctivitis and iritis appear to result from direct contact of the eye with Listeria present in silage during the act of feeding (“silage eye”). The condition is not well documented in goats. Harwood (2004) reports unilateral or bilateral keratoconjunctivitis occurring in a goat herd concurrently with the encephalitic form of listeriosis, but not specifically in association with silage feeding.
Clinical Findings
The encephalitic form is the most common in goats. Though unusual, septicemic and encephalitic listeriosis have been reported in the same goat herd (L0ken and Gr0nst0l 1982).
The initial signs of the encephalitic form are non-specific and include depression, decreased appetite, a decrease in milk production, and a transient fever of up to 42 °C (107.6 °F). These prodromal signs may be followed by incoordination and hemiparesis, with a tendency for the goat to lean, stumble, or move in one direction only. This tendency progresses to obvious torticollis and circling in the same direction. In advanced cases, the goat may be recumbent with the head pulled tightly into the flank, unable to straighten the neck voluntarily (Figure 5.5a).
Deficits of the facial nerve are also common and may occur with or without concurrent hemiparesis and circling. The signs are usually unilateral and include ear droop, ptosis, flaccid buccal muscles with accumulation of feed in the buccal pouch, salivation, and a collapsed nostril (Figure 5.5b). Slack jaw, weak tongue, impaired swallowing, and nystagmus may also be seen. When lesions are bilateral, some of these deficits may be paradoxically less obvious since the abnormalities are symmetrical. Keratitis may be observed as a sequela to abnormal eyelid function.

Figure 5.5 Clinical presentations of encephalitic listeriosis in goats. (a) An adult buck with listeriosis in recumbency with torso, neck, and head drawn tightly to one side and exhibiting profound depression. Source: Courtesy of Dr. Daan Dercksen. (b) Unilateral facial nerve paralysis in an adult female goat with a history of being fed silage. Note the drooped, flaccid right ear, eyelid and cheek, the collapsed right nostril, the flaccid tongue, the feed accumulated in the mouth, and the beard soaked with saliva from excessive drooling. (c) The same goat as in (b). Note the head and neck pulled to the left and the pool of saliva on the floor under the goat's head. Both pictures reproduced by permission of Dr. Jaroslaw Kaba, Faculty of Veterinary Medicine, Warsaw University of Life Sciences, Warsaw, Poland.
Loss of excessive saliva through drooling (Figure 5.5c) and the inability to swallow can lead to acid-base imbalance, electrolyte and fluid losses, dehydration, and weakness. The course of encephalitic listeriosis in goats is usually one to four days, which is shorter than that observed in cattle. The morbidity rate is variable, but the mortality rate can be high.
The septicemic form also begins with depression, loss of appetite, decreased milk production, and fever up to 42 °C (107.6 °F). In these cases, fever may persist and the animal grows progressively weaker over the next several days. Neurologic signs rarely develop, but diarrhea, often bloody, is a common finding in goats. Goats may die within a few days or remain ill for several weeks. Pregnant does abort several days after the onset of septicemia. They may not necessarily show severe signs of septicemia.
Clinical Pathology and Necropsy
The hemogram may remain normal, particularly in the encephalitic form of the disease, or show a neutrophilic leukocytosis. The monocytosis seen in laboratory animals does not occur in ruminants. Analysis of the CSF may be helpful. Protein levels and cell counts are typically moderately elevated. The cells are predominantly monocytes and lymphocytes, with some neutrophils also present. Bacteria are rarely seen in the CSF, and efforts to culture Listeria organisms or detect them by PCR from the CSF are rarely successful.
Historically, serology, while useful for epidemiologic studies, has not been widely applied for diagnosis of individual cases (Morin 2004). Different serodiagnostic techniques have been employed using crude antigens, but a general limitation for all these techniques was a lack of specificity, with cross-reactions to other Gram-positive organisms being common (Low and Donachie 1997). Another practical limitation is that in cases of encephalitic listeriosis, affected animals do not appear to mount a consistent, detectable humoral immune response, in contrast to cases of septicemic listeriosis. An increase in indirect hemagglutination titer is reported after septicemic listeriosis, but not after the encephalitic form (Loken et al. 1982a). Sero-agglutination was found to be unsatisfactory as a screening test for accurately identifying herds with enzootic listeriosis (Nicolas et al. 1974).
ELISA tests have been developed in recent years to detect antibodies against a specific antigen, listeriolysin O, which is an extracellular 58 kDa hemolysin, produced by all the pathogenic strains of L. monocytogenes (Elezebeth et al. 2007). As with other tests, it does not appear to be a reliable indicator of acute-phase disease in cases of encephalitic listeriosis. The kinetics of the antibody response to listeriolysin O in experimentally infected goats has been reported (Rekha et al. 2006).
Culture or molecular identification of L. monocytogenes should be attempted for definitive diagnosis, recognizing that the organism may be difficult to isolate without special enrichment methods. In the septicemic and abortion forms of the disease, feces, milk, and aborted fetuses are suitable specimens. Experimentally infected, septicemic goats shed L. monocytogenes in the feces for 28 days after infection, but only 2 days in milk. Stomach contents, spleen, and liver of the fetus are tissues most likely to be positive on direct culture without enrichment (Gupta et al. 1980). In the encephalitic form, definitive diagnosis in the live animal by identification of the organism is extremely difficult and the disease is usually confirmed at post mortem. Occasionally goats with the encephalitic form are fecal culture positive. Culture of silage is also indicated when silage is implicated. However, the distribution of organisms in silage may be uneven and the offending portions may be long gone by the time clinical disease is observed.
For definitive diagnosis of the encephalitic form post mortem, both fresh and formalin-fixed brain tissues, particularly from the brain stem, should be submitted for histopathology, IHC, bacterial culture, and PCR. Fresh samples should be refrigerated and shipped on cold packs. Gross postmortem findings are uncommon in the encephalitic form of the disease, though visible, focal gray discoloration and malacia of the brain stem have been observed in affected goats (Wood 1972). The CSF may be cloudy and the meninges congested. In most cases, lesions are identified histologically, and consist of focal microabscesses principally in the medulla, but also in the pons and cerebellum. These abscesses are composed primarily of neutrophils. Perivascular cuffing with mononuclear cells and neutrophils, diffuse microgliosis, and a mononuclear infiltrate of the meninges may also be seen. IHC performed on CNS tissues is more reliable than bacterial culture for confirming the presence of L. monocytogenes in tissues (Ehrensperger et al. 2001; Loeb 2004).
In the septicemic form, multiple foci of necrosis may be seen in liver, spleen, kidney, and heart. Multiple, small yellowish spots on the liver of aborted fetuses are highly suggestive of listeriosis. Placentitis and endometritis may also be observed in does that abort. Successful culture is most likely from the liver, spleen, lung, and uterus of septicemic adults.
Diagnosis
Neurologic diseases that can produce localizing signs consistent with a diagnosis of listeriosis include the neurologic form of CAE, focal brain abscesses, cerebrospinal nemato- diasis, coenurosis, middle ear infections, bacterial meningitis, early rabies, and trauma to the facial nerve. Recumbent animals in an advanced stage of encephalitic listeriosis may be misdiagnosed. In a survey of 67 encephalitic listeriosis cases in goats and sheep, 12 of the animals were not diagnosed with the disease until necropsy. Six had a working diagnosis of PEM (cerebrocortical necrosis), one was diagnosed with ketosis, one with pulmonary emphysema, and in four no specific diagnosis was made (Braun et al. 2002).
The differential diagnosis for septicemic listeriosis, particularly when diarrhea is present, includes salmonellosis, yersiniosis, and enterotoxemia. When weakness predominates and diarrhea is absent, milk fever and pregnancy toxemia should be ruled out. Causes of abortion in which the doe shows clinical signs of illness are discussed in Chapter 13.
Treatment
Early intervention improves the prognosis for recovery. Goats already recumbent rarely respond favorably to treatment and a poor prognosis should be given for recumbent animals. Penicillins, tetracyclines, and, where permitted, chloramphenicol, are effective antibiotic choices. Adult goats with the septicemic form of disease responded favorably to IM penicillin administered for three consecutive days at a dose of 2.5 g per day, but shorter courses of therapy were less effective (Loken and Gronstol 1982). In the encephalitic form, IV sodium penicillin at a dose of 40 000 IU∕kg every six hours until improvement is noted, followed by a seven-day course of IM procaine penicillin at a dose of 20 000 IU/kg BID (twice a day), has been recommended (Brewer 1983). Oxytetracycline should be given IV at a dose of 10 mg/kg BID for at least three days. These high dosage levels are necessary to promote passage of antibiotic across the blood-brain barrier and the development of high tissue concentrations in the CNS.
It has been reported that ampicillin or amoxicillin given in conjunction with gentamicin is the treatment regimen of choice in human listeriosis cases. The use of a combination of gentamicin given at a dose of 3 mg/kg bw IV BID and amoxicillin given at a dose of 7 mg/kg bw IM BID was reported in one retrospective case study in small ruminants (Braun et al. 2002). The outcomes for sheep and goats treated with gentamicin/ampicillin were better than for those treated with either penicillin or oxytetracycline. However, more of the animals treated with gentamicin/ amoxicillin had a favorable prognosis at the onset of therapy because they were not yet recumbent. The use of gentamicin in goats is problematic due to prolonged antibiotic residues in meat and milk.
Dexamethasone given at a dose of 0.1 mg/kg IV SID (once a day) has also been used in conjunction with antibiotics in the treatment of encephalitic listeriosis, with the rationale that steroids may suppress the infiltration of mononuclear cells that lead to microabscesses in the brain stem. The non-steroidal anti-inflammatory drug flunixin meglumine has been used at a dose of 2.2 mg/kg bw IV SID in the treatment of goats with encephalitic listeriosis, but its contribution to a favorable outcome is not documented.
Supportive therapy in the form of fluid and electrolyte administration, supplemental feeding, and management of exposure keratitis associated with lid paralysis may be necessary in severely affected animals. Large amounts of bicarbonate and fluid may be lost when salivation is prolonged and intense, so fluid therapy should be managed to address these deficiencies.
Control
In outbreaks of disease, aborting does should be isolated from the herd, and kids should be raised separately from adults. Aborted fetuses, placentas, and discharges should be handled wearing gloves and face masks and disposed of carefully. Kids should not receive unpasteurized colostrum or milk from does involved in the outbreak to avoid neonatal septicemia. Feed samples, particularly silage, should be examined and cultured and infected feeds discarded. Even when culture tests are negative, poor-quality silage with a pH more than 5 should be suspect, and not fed. Recently introduced animals also should be considered suspect as carriers. Floors and pens should be thoroughly cleaned and disinfected. After an outbreak, herd-wide fecal cultures with culling of fecal shedders has been used to effectively eliminate infection from goat herds (Dijkstra 1984c). Because of the zoonotic potential, no unpasteurized milk should be consumed from goats in a herd with a history of listeriosis, since shedding of the organism in the milk of latent carrier animals does occur.
The presence of listeriosis in a herd of dairy goats can be insidious, as illustrated by a situation reported from Belgium (Delhalle et al. 2012). An outbreak of listeriosis occurred in people consuming a soft goat cheese produced with milk from a single farm of 350 Alpine goats. During the follow-up investigation, the milk from all lactating goats on the farm was cultured in pools of 20 samples. One pool was positive. When the 20 samples were individually tested, only one goat was positive. On further testing, the goat was positive only in the right half of the udder, and clinical examination revealed no gross evidence of clinical mastitis. Thus, a single goat with subclinical mastitis due to L. monocytogenes in a herd of 350 goats was responsible for this food-borne zoonotic disease outbreak. When monitoring dairy herds for Listeria infection, it has been shown that submitting the milk filter located in the milk pipe at the point where it enters the bulk milk tank produced better culture results than submitting samples of bulk tank milk, especially if the milk filters were submitted in Cary Blair transport medium (Artursson et al. 2018).
A live, attenuated vaccine has been in use in central Europe and Norway to protect sheep from listeriosis. While case rates in vaccinated and unvaccinated sheep were similar, the severity of disease was less and the response to treatment was better in vaccinated animals (Gudding et al. 1985). A vaccination trial in goats in France produced a sharp reduction in new cases that lasted for at least three months when used in known infected herds. No difference was observed in disease rate or host response to vaccination between live and killed vaccine, except for a rare abortion in does vaccinated with the live vaccine in late gestation (Guerrault et al. 1988).
Goat farmers who produce or market milk, cheese, or other dairy products need to be aware of the zoonotic potential of these products if contaminated with L. monocytogenes. There should be no sale of raw milk products from herds where the Listeria infection status is not known to be negative. Some of the challenges of keeping cheeses free of listeria contamination in small-scale cheese-making operations and approaches to reducing the risk of contamination of soft goat cheeses have been reported (Theodoridis et al. 2006).
Tetanus
Tetanus is a well-known clostridial disease of humans and animals that produces a characteristic syndrome of muscular rigidity, hyperesthesia, and convulsions. Routine prophylaxis against tetanus in goats is recommended.
Etiology and Pathogenesis
The causative agent is Clostridium tetani, an anaerobic, Gram-positive, spore-forming rod found widely in soil and animal feces. Spores are very resistant to destruction and can persist in soil for many years. Proliferation of the organism with release of a potent neurotoxin, tetanospasmin, can occur when spores are subject to a suitable anaerobic environment, as can occur in deep puncture wounds or injuries producing necrotic tissue in susceptible hosts. The organism does not disseminate from the site of proliferation, but the neurotoxin ascends the motor neuron axons in peripheral nerve trunks to the spinal cord, where it blocks the effect of inhibitory interneurons on alpha motor neurons by preventing the release of the inhibitory neurotransmitter gamma-aminobutyric acid (GABA). This results in the sustained discharge of motor neurons and the associated signs of tetany. When the toxin reaches the postsynaptic sites where it exerts its effect, it cannot be neutralized by antitoxin and is only removed by gradual degradation. Death is usually caused by respiratory arrest from dysfunction of the

Figure 5.6 Young goat with advanced tetanus. Note extensor rigidity and opisthotonos. This goat developed tetanus secondary to abrasions of the neck associated with prolonged tethering with a tight rope. Source: Courtesy of Educational Media, Cummings School of Veterinary Medicine at Tufts University, Mr. David Wilman photographer.
tetanic diaphragm. Further explanation of the pathogenesis of tetanus at the cellular and molecular level is available elsewhere (Rings 2004; Zaragoza et al. 2019).
Epidemiology
Goats are susceptible to tetanus, and factors that predispose other livestock to the disease also predispose goats. The tetanus organism may be introduced into the goat via puncture wounds; obstetric interventions, including Cesarean section; performance of routine procedures such as thermal disbudding, dehorning, tattooing, ear tagging, castration, and hoof trimming; dog bites; fighting by bucks; and penetration of the oral mucosa by fibrous plant awns (King 1980). The use of elastrator bands for castration may be particularly dangerous in establishing conditions for the proliferation of spores. In South Africa, tetanus is frequently encountered in young Angora goats after shearing (Van Tonder 1975). Persistent skin irritation caused by constant rubbing from a metal neck chain (Sinha and Thakur 1978) or a rope tether has been identified as causing tetanus in goats (Figure 5.6).
Spores of C. tetani are resident in the intestines of livestock and may be passed in the feces in large numbers, particularly by horses. These spores accumulate in soil, particularly where livestock are kept under intensive management. Goats maintained in barns currently or previously used for horses may be at increased risk of disease.
Clinical Findings
The incubation period varies in tetanus. It can depend in part on the location of the inciting wound or injury and its distance from the CNS, as the toxin has to reach the spinal cord before clinical signs are seen. Tetanospasmin moves intra-axonally at a rate of 75-250 mm/day (Sanford 1995). Clinical disease has been observed in a 1-week-old kid within four days of disbudding and in an adult doe several months after dystocia. In most cases, however, the incubation period is 10-20 days.
Early signs of tetanus include an anxious expression, a stiff gait, and mild bloat. Affected animals adopt a characteristic base-wide or “sawhorse” stance, and the ears and tail become stiff. There is reluctance to move and difficulty opening the mouth. The animal may become constipated. Food may accumulate in the buccal space and salivation may be observed. Prolapse of the third eyelid may occur. Over time, animals become hyperesthetic and respond dramatically to touch or loud noise by stiffening and collapsing to the ground. This may be followed by seizures. Eventually animals are permanently recumbent, with rigid extension of all limbs and opisthotonos. Rumen tympany may be pronounced. Affected animals convulse periodically at the slightest disturbance. Once they are recumbent, death usually occurs within 24-36 hours.
Clinical Pathology and Necropsy
There are no characteristic laboratory abnormalities in tetanus and no definitive necropsy findings, as the neurologic lesion is functional rather than physical. A thorough history and careful inspection of the carcass may lead to identification of the wound or infection site of bacterial proliferation where the organism might be cultured. Because the organism may be present in tissues without causing disease, this supports but does not confirm the diagnosis.
Diagnosis
The diagnosis of tetanus is based on the rather cha.ra.ct.er- istic clinical syndrome it produces. However, at different points in the development of full-blown tetanus, other differential diagnoses must be considered. Laminitis and nutritional muscular dystrophy can produce a stilted or stiff gait, as seen in early tetanus, but not bloat or the other signs. Hyperesthesia and trismus are seen in bacte - rial meningitis, but this condition can be differentiated by CSF analysis. In the terminal stages when recumbency, opisthotonos, and convulsions are present, PEM, which is common in goats, must be differentiated. Strychnine poisoning and hypomagnesemic tetany must also be ruled out, but these are less common in goats. Myotonia congenita, as seen in “fainting” goats, can produce tetanic spasms and collapse in response to touch or loud noise, but these effects are intermittent and resolve spontaneously. The condition is discussed in more detail in Chapter 4.
Treatment
The prognosis is always guarded, but early recognition and intervention improve the recovery rate. Therapeutic goals are to inhibit additional toxin production, neutralize existing unbound toxin, ameliorate the effects of bound toxin, and provide whatever supportive care is necessary. Treatment with systemic penicillin inhibits additional bacterial proliferation and toxin release. Procaine penicillin G at a minimum dose of 25 000 IU∕kg bw IM BID for two to three days is recommended with a reduction to once-a-day treatment after that. Other antibiotics with a Gram-positive spectrum such as ampicillin and amoxicillin may also be used at high, frequent doses.
The drug of choice in human medicine is metronidazole, and this is now being used for tetanus cases in small animal practice as well (Linnenbrink and McMichael 2006), but no reports of its use or effectiveness in ruminants were found. The use of metronidazole in food animals (including all goats) is forbidden in the United States (Payne et al. 1999).
The site of bacterial proliferation should always be searched for and, whenever possible, the wound or infection site should be opened to the air, debrided, flushed with hydrogen peroxide, and infiltrated with penicillin. It is suggested that the area be infiltrated with tetanus antitoxin before the wound-cleaning process begins, to reduce the chance that more preexisting toxin will be absorbed during tissue manipulations.
Neutralization of existing unbound toxin is accomplished by parenteral administration of tetanus antitoxin at a dose of 10 000-15 000 units IV every 12 hours for at least the first 24 hours, and longer if the proliferation site has not been identified and treated. An alternative approach is the onetime administration of antitoxin directly into the CSF via the atlanto-occipital space. In a goat, 5 mL of antitoxin has been introduced into the subarachnoid space after removal of an equivalent amount of CSF (Brewer 1983).
Anticonvulsants, tranquilizers, and muscle relaxants can be administered to reduce the clinical effects of bound toxin. Diazepam can be used at a dose range of 0.5-1.5mg∕kg IV to effect. Acepromazine works well as a tranquilizer in tetanic animals at a dose of 0.2mg∕kg IM. Methocarbamol is an effective muscle relaxant at a dose of 22mg/kg IV. Guaifenesin, given IV to effect as a 5% solution, may also be used to reduce muscle spasms, but care must be taken not to overdose the animal, because it acts by blocking nerve transmission at the level of the interneurons (Rings 2004). Other drugs recommended for use as muscle relaxants but not specifically reported for use in goats are dantrolene sodium, mephenesin, and magnesium sulfate (Rings 2004).
Supportive care includes removing the animal to darkened, quiet surroundings. IV fluids containing dextrose and electrolytes are indicated to counter dehydration and lack of feed intake. An enema may relieve constipation and make the animal more comfortable. The position of the animal should be shifted regularly to avoid decubital ulcers. A nasogastric tube can be passed to relieve bloat and provide fluids and feed per rumen. An egg, honey, milk, glycerin, and oatmeal gruel has been recommended (King 1980). Care must be taken not to traumatize the pharynx and esophagus when the tube is passed repeatedly. When valuable animals are severely affected and the convalescence is expected to be long, surgical creation of a rumen fistula may be indicated to facilitate feeding and bloat control. Any sign of improvement is favorable, but it may take several weeks for complete recovery to occur.
Control
Tetanus can be readily prevented by a combination of improved hygiene and immunoprophylaxis. In general, all wounds should be cleaned promptly and thoroughly. The use of elastrator bands for castration should be avoided. When the immune status of young kids is unknown, routine procedures such as disbudding and castration should be accompanied by injection of 150-250 units of antitoxin. When the status of adults is unknown, 500-750 units of antitoxin can be administered when treating wounds, dystocias, and other potential sources of tetanus.
It is recommended that routine vaccination for tetanus be incorporated into the herd health program. For small ruminants, tetanus is often included with Clostridium per- fringens types C and D as a trivalent vaccine, which can serve as the foundation for a goat preventive vaccination program. Initially, all goats vaccinated should receive a booster vaccine three to four weeks after their initial vaccination. Then, if pregnant does are vaccinated one month prior to parturition, their kids will be protected by passive colostral antibody for at least several weeks, and can be vaccinated for the first time at 3-4 weeks of age. The kids then should be boostered three to four weeks later, and then revaccinated annually, preferably three to four weeks before kidding. Bucks should also be included in the vaccination protocol.
Botulism
Botulism, a fatal paralysis resulting from the ingestion of the preformed neurotoxin produced by Clostridium botulinum, has been reported in goats, but is uncommon.
Etiology and Pathogenesis
Cl. botulinum is an anaerobic, Gram-positive, sporeforming rod found in soil and vegetation and as a normal inhabitant of the intestine of various livestock species, including poultry. Seven neurotoxin types (A-G) of Cl. botulinum are known along with different subtypes. As in cattle, botulism in goats is caused principally by types Cβ and D. Spores revert to the vegetative state under suitable anaerobic conditions and produce an extremely stable neurotoxin. Bacterial proliferation and toxin production commonly occur in infected, decomposing carcasses and decaying vegetation contaminated with Cl. botulinum. Livestock become ill after consuming preformed toxin. Ingested toxin is absorbed from the intestine and reaches the nervous system via the blood. The toxin acts primarily on lower motor neurons, interfering with the release and function of acetylcholine, the principal neurotransmitter. The result is a general flaccid paralysis that includes the diaphragm and leads to death by asphyxia.
In experimental type Cβ botulism in goats, clinical signs usually appeared on day two or three after oral administration of toxin. Doses as small as 0.5 minimum mouse lethal dose (MMLD)∕g of bw were fatal, and a cumulative toxic effect was observed when small doses were fed over eight days. Goats that grazed pasture or ate silage tolerated higher challenges than goats receiving hay and concentrate, suggesting a protective effect of green forage (Fjoelstad 1973). In another experimental study, goats were given type C botulism toxin SC in doses ranging from 15.6 to 500 LD/kg bw. Goats given doses of 250 or 500 LD/kg bw died at 42-46 hours post inoculation. Goats given 31.3, 62.5, or 125 LD/kg bw developed subacute disease, while the goat receiving 15.6 LD/kg developed a chronic form of the disease, indicating that clinical response in goats is dose dependent. Toxin was only detectable by the mouse toxicity test in goat serum at the highest dose administered (Santos et al. 1993).
Epidemiology
There is little information on the incidence of botulism in goats throughout the world and few clinical reports. In South Africa, where cattle botulism is considered common and is frequently associated with gnawing on the bones of carrion as a result of phosphorus deficiency, botulism in Angora goats is reported, but is comparatively rare. In contrast to cattle, all reported cases in Angora goats were associated with contaminated feed, either milled lucerne containing rodent carcasses or poultry litter containing dead chickens (Van Tonder 1975). However, botulism in goats resulting from osteophagia associated with likely phosphorus deficiency has been reported from Brazil, where 37 adult does in a herd of 460 goats died at pasture over a period of two months (Riet-Correa et al. 2012). Botulism in goats associated with ingestion of poultry litter as feed has also been reported from Brazil, where 233 of 450 Moxoto goats died within 48 hours of the feed being introduced (Lobato et al. 2008). The feeding of poultry litter, especially if it contains bird carcasses, is widely recognized as a risk factor for botulism in domestic ruminants, as is the feeding of hay, silage, and small-grain forage preserved in plastic tubes or bags, when these feedstuffs have been contaminated with spores from soil, dead birds, dead rodents, or other sources.
In Senegal, a water-borne outbreak of type D botulism killed 50 goats, 100 sheep, 10 cattle, and 5 horses. The source of toxin was identified as a dead mammal contaminating the water well (Thiongane et al. 1984). In a more recent report from South Africa, type D botulism was confirmed in a mixed flock of sheep and Boer goats via the mouse toxicity test using intestinal contents from one of the affected sheep (van der Lugt et al. 1995). Most affected goats and sheep in that outbreak were found dead without first exhibiting clinical signs or had a short course of disease lasting 2-12hours.
Clinical Findings
Flaccid paralysis is the cardinal manifestation of botulism, but the occurrence and progression of particular signs can vary considerably in individual cases. The duration and severity of disease depend on the dose of toxin ingested and can range from peracute to chronic. In experimental caprine botulism (Fjoelstad 1973), early signs include a hoarse character of the voice, depression, anorexia, difficulty in chewing, salivation, and a reluctance to stand. When forced to stand, goats show trembling of the limb muscles and stiffness in the hindquarters, and will lie down immediately when permitted. Some show an abdominal respiratory effort. Hypersensitivity to light may be seen. As the disease progresses, animals are unable to stand due to flaccid paralysis, but remain sternal. This progresses to lateral recumbency and death, sometimes as early as two days after toxin ingestion. Recoveries are possible after a prolonged illness when low doses of toxin are initially ingested.
In the clinical outbreak reported from South Africa, death without clinical signs was the most common presentation. Goats that did show clinical signs initially showed restlessness, reluctance to move, a stiff gait, muscle tremors, grinding of the teeth, salivation, foaming at the mouth, and pupillary dilatation. They then became recumbent, exhibited paddling of the limbs, and died within minutes to a few hours of lying down (van der Lugt et al. 1995).
In the outbreak in Brazil associated with osteophagia, tetraparesis leading to tetraplegia and recumbency were predominant signs, but other notable signs included obvious tongue paralysis and wry or twisted neck (cervical torticollis) (Riet-Correa et al. 2012).
Clinical Pathology and Necropsy
There are no characteristic clinicopathologic laboratory abnormalities in botulism and no specific necropsy findings, because the neurologic lesion is functional rather than physical. Grossly affected animals may show a variety of lesions: congestion of the carcass; some ascites, hydrothorax, and hydropericardium; pulmonary congestion and emphysema; and petechiation of the ruminal, abomasal, and duodenal mucosa (van der Lugt et al. 1995). Stomach contents and suspect feedstuffs may be tested for the presence of toxin by toxin neutralization assays in laboratory animals, usually mice. However, distribution of toxin in feeds may be patchy, and ingested toxin may already have been absorbed from the gut, so these tests are often unrewarding in addition to being costly and time-consuming. The blood of goats is unlikely to contain sufficient toxin to be a useful sample for animal challenge studies (Santos et al. 1993). Culture of the organism from feeds or the tissues of affected animals may be misleading, because the organism may be present without participating in disease.
Diagnosis
In most cases, the diagnosis of botulism is presumptive based on identification of a feed source contaminated by likely sources of Cl. botulinum, such as rodent and bird carcasses, in conjunction with a characteristic syndrome of rapidly progressing generalized weakness or flaccid paralysis. Several other conditions should be considered in the differential diagnosis. Enzootic muscular dystrophy should be responsive to vitamin E and selenium therapy in the early stages. Milk fever in lactating does should respond to calcium therapy. Tick paralysis may appear similar, but ticks should be identifiable on the affected goat. The paralytic form of rabies should be considered and can be confirmed at necropsy. Skeletal trauma and spinal cord damage can be ruled out by careful physical examination and supported by radiographs or other imaging techniques.
In the reported South African outbreak, sudden death was the predominant presentation, and the necropsy findings suggested that heart failure was contributory to that outcome. Therefore, the differential diagnosis also included plant poisonings caused by cardiac glycoside- and monofluoroacetate-containing plants, gousiekte-inducing shrubs, and ionophore toxicity (van der Lugt et al. 1995). These cardiotoxic agents are discussed further in Chapter 8.
Treatment
The prognosis is grave in botulism. If type-specific or polyvalent antitoxin were available, it could be useful given early on when toxin is still circulating and has not yet fixed to neuromuscular junctions, but there is little documentation for this in the veterinary literature. Animals with slowly progressive disease may recover gradually over many weeks. Supportive care is necessary and includes maintenance of hydration, tube feeding, slinging or frequent shifting to avoid decubital ulcers, and, in extraordinary cases, ventilatory support when the diaphragm is paralyzed. Except when aspiration pneumonia or wound infections are present, the use of antibiotics is discouraged. Clostridiocidal drugs may lyse vegetative Cl. botulinum cells, thus increasing the amount of free toxin in the intestinal tract. Aminoglycosides may potentiate neuromuscular weakness and a non-depolarizing type of neuromuscular block (Anniballi et al. 2013).
Control
Because the disease appears to be sporadic in goats, control measures are limited. In cattle, it is recommended that grazing animals be provided adequate protein and phosphorus in the diet to reduce osteophagia. At the least, feed and water supplies should be routinely examined to identify the presence of dead rodents, and waterfowl and poultry litter should be fed cautiously and only if free of whole or fragmented carcasses.
Vaccines are available in some countries, mainly for use in cattle, but may also in some cases, e.g., South Africa., be approved for use in goats. Vaccines can be protective, but vaccination is not widely practiced. If goats are vaccinated, a bivalent C and D toxoid should be used. Animals that have not previously been immunized should be given two injections of vaccine at an interval of four to six weeks, starting at 3 months of age. Thereafter they should be revaccinated with a single dose annually.
Because botulism occurs in human beings and can be food borne, regulatory agencies concerned with food safety have studied the risks of botulism from foods of animal origin. Specifically, the UK Food Standards Agency has undertaken a risk assessment related to meat and dairy products from sheep and goats, and determined that the risks are low, even when meat or milk is derived from clinically healthy sheep or goats at farms where there have been clinically suspected cases of botulism in sheep and goats. In addition, it was concluded that there should be no requirement to restrict the slaughter of healthy sheep and goats from herds where cases of confirmed or suspected botulism have occurred. This risk assessment was predicated on the assumption that meat would be properly cooked and milk pasteurized before consumption. It was also recognized that feeding of poultry litter to small ruminants was a major risk factor in the occurrence of botulism on farms and that good risk communication to farmers on the production, storage, and spreading of poultry litter was an important mitigation measure (UK Food Standards Agency 2008).
Clostridium perfringens Type D Enterotoxemia
Disease due to Cl. perfringens type D is associated mainly with hemorrhagic enteritis and/or sudden death in goats, and is discussed in detail in Chapter 10 in the section on enterotoxemia.
However, clinical signs of neurologic disease, such as opisthotonos and convulsions, are sometimes observed in cases of enterotoxemia, particularly in calves and lambs (Rings 2004). At necropsy, sheep show a characteristic brain lesion, cerebellar microangiopathy, which is considered pathognomonic for the disease in sheep (Buxton et al. 1978). Neurologic manifestations of enterotoxemia in goats were poorly documented, until Uzal et al. (1997) reported on the histologic findings of cerebellar microangiopathy with perivascular edema in two goats in Australia that died suddenly and were confirmed with type D enterotoxemia. One goat also demonstrated bilateral symmetrical foci of encephalomalacia in the cerebellar peduncles. Similar histologic findings of focal symmetrical encephalo- malacia have subsequently reported from goats with confirmed (Colodel et al. 2003) and putative (Oliviera et al. 2010) enterotoxemia in Brazil. More recently, a retrospective study of confirmed caprine cases of type D enterotoxemia in California identified eight affected goats with histologic evidence of microangiopathy, most frequently in the cerebral cortex, corpus striatum (basal ganglia), and cerebellar peduncles (Ortega et al. 2019).
Epsilon toxin of Cl. perfringens type D is not a direct neurotoxin and the pathogenesis of neurologic signs and brain lesions in ruminants with type D enterotoxemia is not fully understood. Experimentally, young goats given high doses of epsilon toxin showed clinical neurologic signs of paddling, opisthotonos, and convulsions, but no brain lesions, while lambs given similar doses showed similar clinical signs and histologic lesions of perivascular edema (Uzal and Kelly 1997). In a related experiment, goat kids were given whole cell cultures of Cl. perfringens type D intraduo- denally and these kids did develop characteristic brain lesions, suggesting the possibility that, at least in goats, CNS manifestations of enterotoxemia may be associated with bacterial components other than or in addition to epsilon toxin (Uzal and Kelly 1998).
Meningoencephalitis and Brain Abscesses
Meningoencephalitis in goats can be bacterial or thermal. The latter occurs due to injudicious use of a hot disbudding iron during horn bud removal in the kid. Brain abscesses occur only sporadically in goats.
Etiology and Epidemiology
Bacterial meningoencephalitis is seen most commonly in young kids, occurring as a sequela to neonatal septicemia arising from navel infection. Meningoencephalitis may be the only manifestation of septicemia, or it may be one of a constellation of signs, including omphalophlebitis, polyarthritis, pneumonia, diarrhea, and endotoxic shock. Neonatal septicemia is a major cause of kid mortality worldwide, but the frequency of CNS involvement is not well established (Sherman 1987). Sporadic cases of meningoencephalitis can also be seen in mature goats.
Multiple factors contribute to the high frequency of bacterial infections in young kids. They include failure of passive transfer of maternal antibodies caused by inadequate colostrum intake by neonates, failure to treat the navel with antiseptics after birth, poor environmental sanitation caused by overcrowding, inadequate drainage or insufficient bedding, and stresses of weather and poor nutrition, among others.
The most commonly involved bacterium in septicemia and subsequent meningoencephalitis is Escherichia coli, but other Enterobacteriaceae may be isolated as well. In addition, Streptococcus Zooepidemicus has been identified as the cause of meningoencephalitis in a yearling goat (Gibbs et al. 1981). Cryptococcosis of the CNS has been reported in goats in Brazil (Santa Rosa et al. 1987). L. monocytogenes may occasionally produce a general meningoencephalitis, but is more commonly associated with focal brain stem lesions. Corynebacteriumpseudotuberculosis and Trueperella (Arcanobacterium) pyogenes may occasionally cause meningoencephalitis secondary to extension of infection from superficial lymph node and soft tissue abscesses of the head and neck. There is a single case report of pyogranulomatous meningoencephalitis in a goat due to Corynebacterium ulcerans (Morris et al. 2005). Meningitis also may occur during mycoplasma septicemia in goats (East et al. 1983).
A major non-infectious cause of meningoencephalitis in kid goats is the removal of horn buds with a hot, usually electric, disbudding iron. In contrast to calves, the frontal bone of kids is thin and the frontal sinuses are undeveloped. Excessive heat or prolonged application of the disbudding iron to the skin and horn bud can lead to thermal damage of underlying bone, meninges, and brain. Proper techniques for disbudding are discussed in Chapter 18.
It has been stated that cerebral abscesses caused by Staphylococcus aureus, Fusobacterium necrophorum, and Trueperella (Arcanobacterium) pyogenes are common in both sheep and goats (Brewer 1983). However, specific studies on the etiology and pathogenesis of brain abscesses in goats are lacking. As in other ruminant species, goats may be predisposed to pituitary abscesses of hematogenous origin by the presence in ruminants of the rete mirabile, a complex mass of capillaries surrounding the pituitary gland. Five such cases are documented in goats (Lomas and Hazell 1983; Pedrizet and Dinsmore 1986).
Pathogenesis
Bacterial infections are most likely to involve the leptome- ninges, choroid plexus, and ventricular walls, and not penetrate into the parenchyma, so that any encephalitis that occurs tends to be superficial. It is speculated that in septicemic animals, bacteria become established on these membranous surfaces via transport within blood monocytes destined to develop into CNS macrophages that normally reside on these membrane surfaces (Cordy 1984). Meningoencephalitis can be focal or diffuse. When the spinal meninges are involved, extension of inflammation to the nerve roots can also occur. In thermal meningoencephalitis caused by disbudding, the lesions are usually focal in the frontal region of the cerebrum. Thermal lesions alone can account for the neurologic dysfunction that occurs, but bacterial invasion also can occur secondary to thermal necrosis of skin and bone overlying the brain (Wright et al. 1983), and infection should be considered as a likely sequela when managing thermal necrosis cases associated with hot iron disbudding (Thompson et al. 2005).
Factors leading to the development of cerebral abscesses in goats are not well defined. The behavioral pattern of frequent head butting with the potential for traumatic injury and the common practice of hot iron disbudding of kids are likely contributors to the potential development of abscesses in young goats. Hematogenous spread from focal or generalized infections is also possible, as in the pituitary abscess syndrome. The clinical signs that develop in cases of brain abscess depend on the size and location of the abscess, and are highly variable. In one instance, a cerebellar abscess in a Nubian doe led to rostral transstentorial herniation of the brain (Kornegay et al. 1983). In another case, a pyogranuloma involving the cerebellum, cerebellar peduncles, and pons in a 6-year-old goat appeared to have been an extension of a middle ear infection. In that case, the clinical signs were suggestive of vestibular dysfunction and included circling, vertical nystagmus, and head tilt (Morris et al. 2005).
Clinical Findings
Fever is common in bacterial meningoencephalitis and may also occur in the thermal form. Not all possible signs of meningoencephalitis are seen in all cases. Variability depends on whether the lesions are focal or diffuse, and mild or severe. Possible signs include mania or an anxious expression, trismus, cutaneous hyperesthesia, and hypersensitivity to sound. Muscular spasms or rigidity may also be observed or palpated, especially over the neck and back. Recumbent animals may show extensor rigidity of the limbs, opisthotonos, and convulsions.
In goats, depression occurs more often than mania. Incoordination, paraplegia, and coma are common signs. Blindness is also frequently reported in affected kids, and may be accompanied by hypopyon. When hypopyon is not obvious, fundic examination may reveal papilledema and vascular congestion. While mortality is generally high, spontaneous recoveries from thermal meningoencephalitis have been reported (Sanford 1989).
Kids with signs of meningoencephalitis should be examined for other evidence of septicemia, particularly omphalophlebitis, pneumonia, and hot swollen joints. Frequently animals with thermal meningoencephalitis may show no prodromal signs and die suddenly hours to weeks after disbudding injury is incurred.
Though variable, signs most often associated with brain abscesses include mental depression, clumsiness, head pressing, blindness, and intermittent attacks of motor irritation, including convulsions (Constable et al. 2017). In pituitary abscess syndrome, dysphagia, blindness, abnormal pupillary responses, and reduced jaw tone are the most common signs (Pedrizet and Dinsmore 1986).
Clinical Pathology and Necropsy
Characteristic changes in the CSF caused by meningoencephalitis include an increase in white blood cells, particularly neutrophils, and an elevation of the total protein. Bacteria may also be present in the CSF. In severe cases, the CSF may be visibly cloudy on collection. Gram staining of the CSF sediment can be helpful in guiding therapy while cultures are pending.
Brain abscesses that may occur deep in the parenchyma of the brain may not induce inflammatory changes in the CSF. The inflammatory response may be reflected in the hemogram in both meningoencephalitis and brain abscesses. Kids with meningoencephalitis are often hypogammaglobulinemic.
Meningoencephalitis is usually detectable grossly at post mortem as thickening, cloudiness, and hemorrhage of the meninges, along with hyperemia and congestion of the adjacent brain tissue. In early cases, histologic examination may be necessary to identify active inflammation. Signs of septicemia may be observed in other tissues, such as hemorrhage of serosal surfaces and cloudy joint fluid. Bacterial culture of liver, heart blood, and CSF should be carried out when there is a potential herd problem. In thermal meningoencephalitis, obvious focal, circular, necrotic, fibrinous lesions of the frontal bones (Figure 5.7) and underlying meninges and cerebrum will be observed, representing the points of application of the disbudding iron. Focal abscesses are revealed by systematic serial section of the brain or inspection of the sella turcica in the case of pituitary abscesses.
Diagnosis
The presumptive diagnosis of meningoencephalitis in young kids is based on typical clinical signs in conjunction with a history of recent hot iron disbudding or
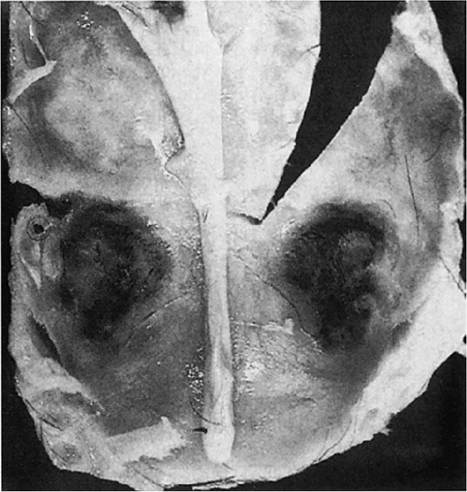
Figure 5.7 Circular lesions of the skull associated with excessive heat applied to the head during a thermal disbudding procedure with a hot iron. Source: Wright etal. 1983 / Veterinary Medicine Small Animal Clinician.
identification of management factors that predispose to septicemia. Meningoencephalitis and brain abscesses can virtually always be confirmed by postmortem examination, and this is the most common method of diagnosis for the latter.
Treatment
The prognosis is guarded in meningoencephalitis, but early, aggressive intervention can result in some successful outcomes. Antibiotic therapy is indicated in all cases of meningoencephalitis because there is evidence of secondary bacterial invasion, even in cases initiated by thermal injury. Resolution of brain abscesses with antibiotic therapy is rarely achieved.
Treatment should be initiated using broad-spectrum bactericidal antibiotics until culture and sensitivity results are available to guide therapy. Several antibiotics have been recommended for use in ruminants with Gram-negative bacterial meningitis (Jamison and Prescott 1988).
Trimethoprim-sulfonamide combinations are recommended for IV use at doses of 16-24 mg combined/kg at least every 12 hours. Third-generation cephalosporins such as cefotaxime or moxalactam can be used IV at 50 mg/kg two to four times a day. Gentamicin can be used at a dose of 3 mg/kg IV or IM three times a day, either alone or in conjunction with trimethoprim-sulfonamide combinations, cephalosporins, ampicillin, or penicillin.
The recommended dose for sodium ampicillin is 10-50 mg/kg IV or IM given four times a day. The dose for sodium penicillin G is 20 000-40 000 IU/kg given IV four times a day. Penicillin or ampicillin should not be used alone when there is any likelihood of Gram-negative bacterial involvement, but is usually effective alone in streptococcal infections. The duration of antibiotic therapy depends to a large extent on the clinical response, but should continue for at least 48 hours after the goat appears normal.
Antibiotics should be administered in cases of thermal meningoencephalitis associated with hot iron disbudding. In one report from New Zealand, 18 of 150 kids showed altered mentation two days after hot iron disbudding and were treated with a single dose of long-acting oxytetracycline. On the next day, an additional 12 of the 150 disbudded kids were found dead and 5 that were necropsied had lesions of cerebral infarction beneath the disbudding sites. It was concluded that the 18 goats treated the day before also had thermal injury, but survived because of the antibiotic therapy that had been given (Thompson et al. 2005).
Non-steroidal anti-inflammatory drugs are also indicated, including phenylbutazone at a dose of 10 mg/kg SID or flunixin meglumine given IV or IM at 1-2 mg/kg every 12 hours. Aspirin can be given to goats with a developed rumen at a dose of 100 mg/kg orally every 12 hours.
Affected animals should be kept in quiet, dimly lit, well- bedded surroundings. They should be turned frequently if recumbent to minimize decubital ulcers and hypostatic congestion of the lung. If excitatory signs are present, anticonvulsant therapy or sedation may make the animal more comfortable and manageable, as described earlier for tetanus.
Control
When bacterial meningitis is confirmed in kids, a careful review of kid-rearing techniques with the owner or herd- sperson is necessary to identify deficiencies in management. Special attention must be paid to identifying problems of overcrowding and poor sanitation, inadequate disinfection of navels, and failure of transfer of passive immunity, as discussed in Chapter 7. Serious kid losses caused by septicemia and meningitis have been reported in herds in which kids were deprived of colostrum and instead fed commercial products advertised as colostrum supplements (Scroggs 1989; Custer 1990).
Veterinarians should provide information to clients on the risks of hot iron disbudding and the proper techniques for performing it. If thermal meningoencephalitis does occur in a herd, the veterinarian should ask to be present at subsequent disbudding sessions to identify any problems associated with the disbudding iron or its application.
Despite the potential problems of thermal meningoencephalitis, hot iron disbudding remains the most efficient, reliable way to prevent horn growth when done properly. It has been recommended that a dose of broad-spectrum antibiotic be given to kids prophylactically at the time of hot iron disbudding, because some of the losses that occur may be due as much to secondary infection of the meninges and brain entering through devitalized tissue as to the thermal lesion itself (Thompson et al. 2005).