Biopsy techniques
1.6.4.1 Liver biopsy
Laparoscopic liver biopsy is considered by many clinicians to be the preferred method of liver biopsy.7 Often, other diagnostic modalities do not provide sufficient tissue or information on gross appearance of the liver and adjacent organs (Figures 1.77, 1.78, and 1.79).
Generally, a right lateral approach is used for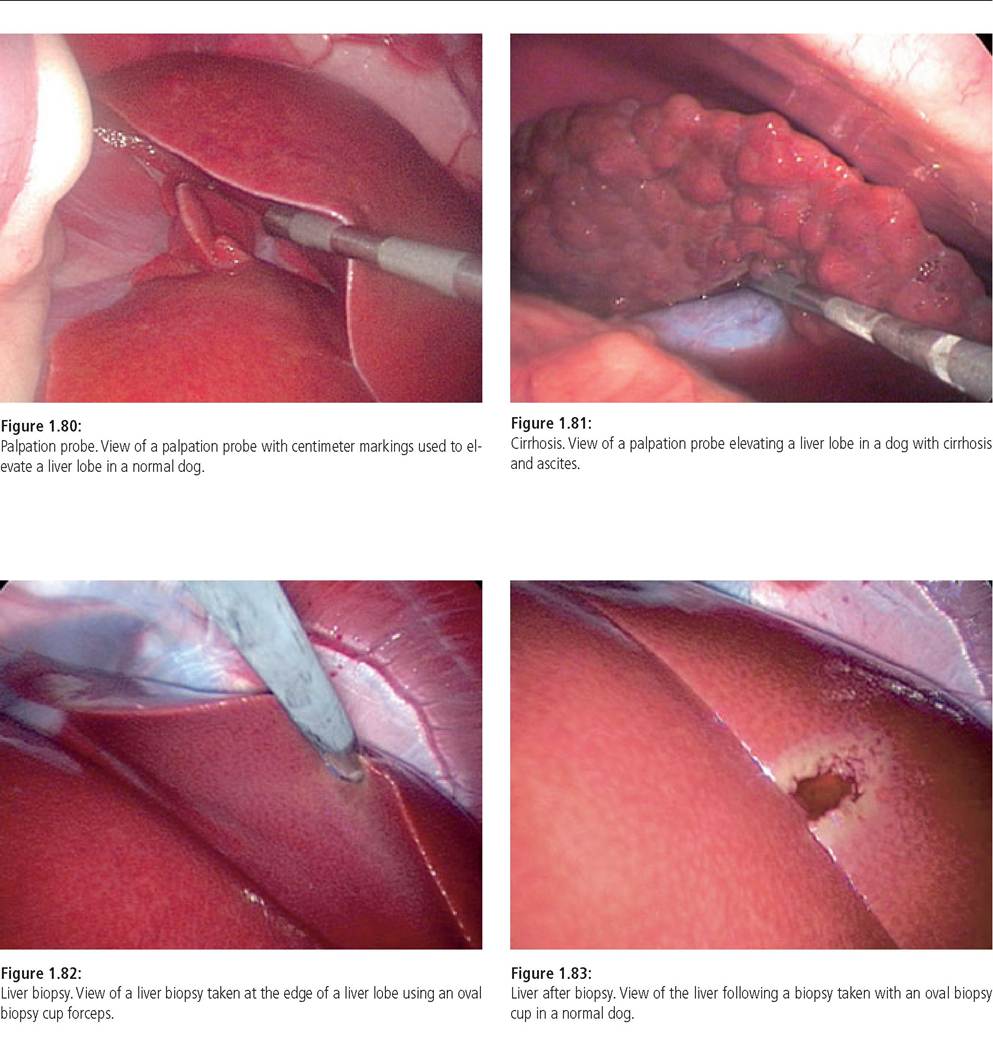
evaluation of the liver, the extrahepatic biliary system, and the right limb of the pancreas. With this approach one is able to examine over 85% of the hepatic surface. Laparoscopic liver biopsies also provide enough tissue for culture, metal analysis, or other diagnostic uses.8
Prior to liver biopsy, coagulation parameters, including a buccal mucosal bleeding time, are evaluated. Mild coagulopathies are generally considered as a relative contraindication for hepatic biopsy because the coagulation status does not necessarily predict if the patient will bleed from a liver biopsy site. The author will frequently biopsy dogs or cats with slightly abnormal coagulation parameters or low platelet counts and rarely has identified problems from excessive bleeding.
Once the liver and extrahepatic biliary system have been examined, palpated, and the decision to obtain a liver biopsy has been made, the palpation probe is removed (Figures 1.80 and 1.81). For liver biopsies, the author recommends using a 5mm oval cup biopsy forceps. A recent study emphasized the benefit of laparoscopic cup “wedge” biopsies as compared to 18-gauge needle biopsies finding that histopathology findings from evaluation of the smaller needle biopsies correlated only in approximately 50% of the cases with those from evaluation of the larger laparoscopic cup biopsies.8 The author uses oval biopsy cups to biopsy either an edge of the liver or obtain samples over the flat surface of the liver.
It is important to biopsy areas that appear normal as well as those that appear abnormal. Some authors suggest that biopsies taken at the edge of the liver often do not reflect deeper lesions and that the histopathology at the subcapsular edge of the liver is usually more reactive. However, the author believes that the samples collected by laparoscopic cup biopsy are so large that this should not be considered a major concern. In rare instances when a deep hepatic lesion is suspected but not readily evident over the surface of the liver, a core biopsy needle can be directed into the lesion. Needles of 16 gauge or larger are required to obtain samples of adequate size.Once the location of the biopsy site is selected, the biopsy cups are opened then closed around the sample area (Figure 1.82). The author generally holds the cups tightly closed for approximately 30 seconds before pulling the sample away from the liver. Generally, three to four biopsy samples from representative sites are taken from the liver. The biopsy site is then closely monitored for excessive bleeding (Figure 1.83). Usually little if any blood is lost at the biopsy site. If bleeding is considered to be excessive several steps can be taken. First, the palpation probe can be directed to the biopsy site in order to apply pressure over the site of bleeding. Alternatively, a small piece of saline soaked Gel-Foam® can be placed into the biopsy site using either laparoscopic grasping or biopsy forceps. In almost all cases this is sufficient for controlling bleeding. If continued excessive bleeding occurs, electrocoagulation, ligature clip, or loop ligature placement may be required.
1.6.4.2 Pancreatic Biopsy
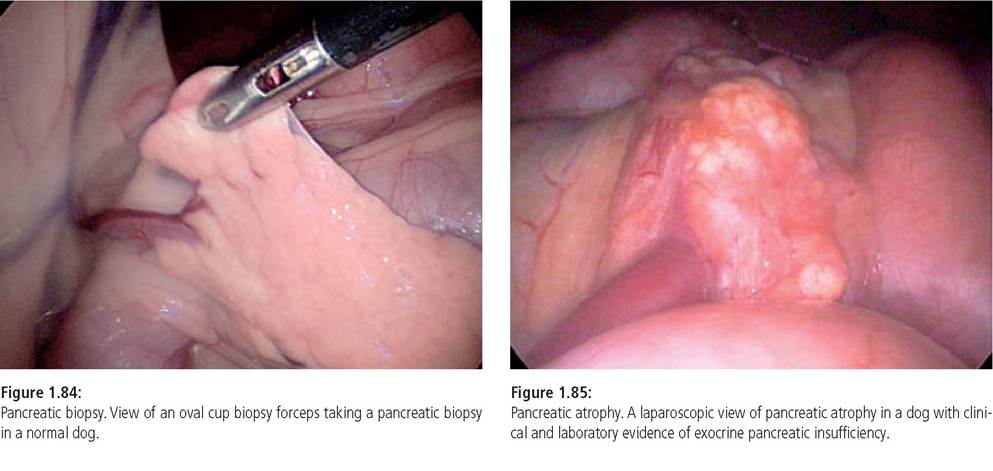
Laparoscopic forceps are also used to biopsy the pancreas (Figures 1.84 and 1.85).7 The author finds pancreatic biopsies to be generally free of complications and a study evaluating
laparoscopic pancreatic biopsies in normal dogs found no postoperative complications or evidence of secondary pancreatitis.9 Indications for pancreatic biopsies include cases suspected of having either acute or chronic pancreatitis or pancreatic neoplasia. The author sometimes uses laparoscopy to confirm the presence of acute pancreatitis and to concurrently place a jejunostomy feeding tube.
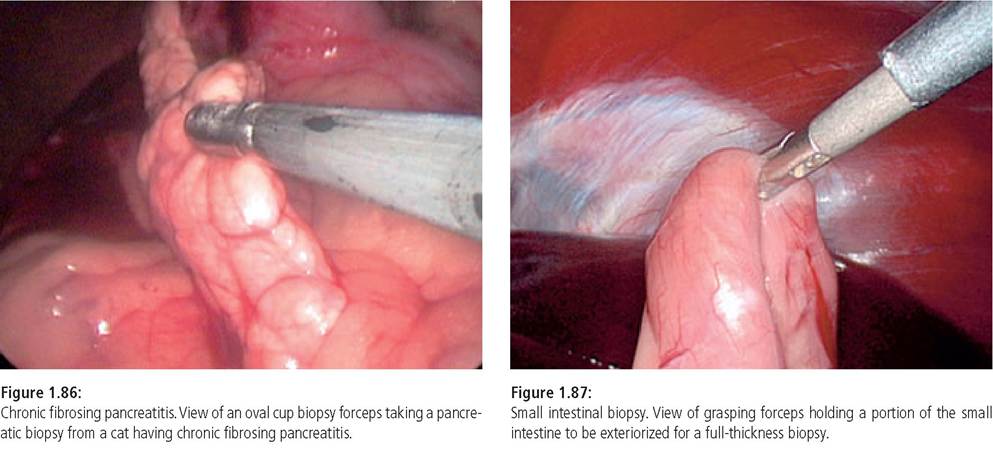
It is also possible to lavage the pancreatic area using laparoscopic guidance of a lavage and suction apparatus. Chronic pancreatitis is a common finding in the cat and is often associated with cholangiohepatitis and IBD (Figure 1.86). Laparoscopy is well suited for the diagnosis of these conditions and for the biopsy of all three organs.Generally, “punch type” biopsy forceps work well for collection of a pancreatic biopsy. For evaluation of the pancreas, a right lateral approach is preferred. This approach gives an excellent view of the duodenum, the right limb of the pancreas, as well as the extrahepatic biliary system and the liver. The left limb of the pancreas is more difficult to examine from this approach and requires a ventral approach and retraction of the omentum. The suggested biopsy location is on the edge of the pancreas away from the pancreatic ducts that traverse the center of the gland and enter the duodenum. The author generally only takes one or two representative biopsy samples of the pancreas unless multiple lesions are present.
1.6.4.3 Intestinal biopsy
Full-thickness small intestinal biopsies can be obtained using laparoscopy by exteriorizing a piece of intestine through the abdominal wall and collecting the sample externally as would be done when performing a standard surgical biopsy.1 An atraumatic forceps with multiple teeth is used to grasp the intestine at the site to be sampled. It may be necessary to “run” the bowel with two grasping forceps in order to select a section of the bowel for biopsy. The antimesenteric border is then firmly grasped with the forceps. The intestine is pulled to the cannula (Figure 1.87). Using a scalpel blade, the grasping forceps cannula incision is extended large enough to exteriorize the loop of bowel. One should see the scalpel blade enter internally parallel to the cannula shaft. The blade then cuts away from the cannula increasing the length of the abdominal incision. The cannula, forceps, and intestine together are then withdrawn through the incision.
When a 3- to 4-cm loop of intestine is exteriorized, stay sutures are placed in the intestine to prevent it from falling back into the abdominal cavity. A small full-thickness biopsy is then obtained in the same manner as one would do when performing an exploratory laparotomy. Following the biopsy and closure of the intestine, the intestinal loop is returned into the abdominal cavity.An intestinal biopsy should always be the last laparoscopic procedure to be performed as the pneumoperitoneum is lost during the procedure. If additional intestinal biopsies or other laparoscopic procedures are to be performed, the trocar cannula must be reintroduced through the abdominal inci-
sion, the incision sealed around the cannula, and a pneumoperitoneum reestablished. A technique for multiple biopsies of the intestine in conjunction with a serosal patch graft has also been described.10 This involves retaining each segment of the bowel biopsied with stay sutures and then suturing together all of the biopsy sites in order to create a serosal patch graft.
1.6.4.2 Otherbiopsytechniques
A number of other biopsy techniques can also be performed using laparoscopic direction, including biopsy of mass lesions, lymph nodes, the spleen, and other organs. Splenic biopsies are generally safe to perform using the cup-type biopsy forceps. Technique, precautions, and coagulation control are similar to those of a liver biopsy. Laparoscopy may also be used to determine the cause of an unexplained abdominal effusion. The fluid is aspirated under laparoscopic guidance in order to enable examination of the abdominal contents.
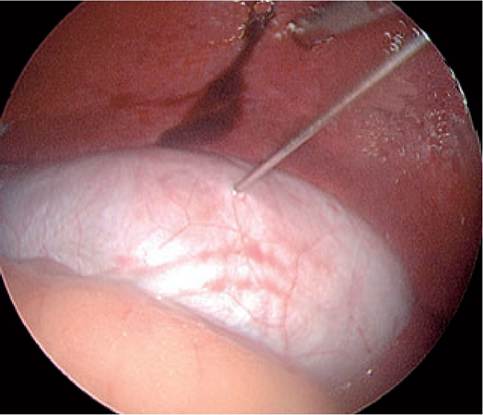
Figure 1.88:
Cholecystocentesis. View of a laparoscopy-guided Cholecystocentesis using a 20-g needle.
1.6.5