Indications
Common indications for diagnostic laparoscopy in gastroenterology include the examination and biopsy of abdominal organs or masses (Table 1.12). Laparoscopy is frequently used as a method for obtaining liver, pancreas, kidney, splenic, and intestinal biopsies.1,2 Laparoscopy is also used to diagnose and
Table 1.12: Laparoscopic procedures in small animal gastroenterology
Diagnostic Procedures
■ Liver biopsy
■ Cholecystocentesis
■ Pancreatic biopsy
■ Intestinal biopsy
Surgical Procedures
■ Feeding tube placement
■ Gastropexy
■ Gastric foreign body removal
to stage the extent of neoplastic conditions of the abdominal cavity.3 Laparoscopy may reveal small (0.5 cm or less) metastatic lesions, peritoneal metastases, or other organ involvement not easily observed by other techniques.
An unexplained abdominal effusion is another indication for laparoscopy when other diagnostic modalities used to determine the cause are unsuccessful. Full-thickness intestinal biopsies can also be performed using laparoscopic assistance. Other ancillary diagnostic techniques using laparoscopic guidance include gallbladder aspiration (cholecystocentesis), and splenoportography.1The advantages of laparoscopy over a conventional surgical laparotomy include improved patient recovery because of smaller surgical sites, lower postoperative morbidity, and decreased infection rate, postoperative pain, and hospitalization time. Other less obvious benefits of laparoscopy are related to fewer stress mediated factors than do occur with surgery.4
Due to the limited degree of invasiveness of this procedure there are few contraindications for laparoscopy. Often, the high-risk surgical patients are good candidates for a laparoscopic procedure.
Abdominal effusion, abnormal clotting times, and poor patient condition are only relative contraindications. Fluid can be removed prior to or during a laparoscopic procedure and has little influence over the success rate of the procedure. Abnormal clotting times may also not definitively preclude the use of laparoscopy. Abnormal coagulation due to hepatic failure does not always correlate with excessive bleeding at the biopsy site.2 Laparoscopy further makes it possible to visually select areas that appear to be less vascular and to monitor the extent of bleeding following the collection of a biopsy. If bleeding is considered to be excessive, various laparoscopic techniques can be used to control hemorrhage.Absolute contraindications for laparoscopy include septic peritonitis or conditions for which surgical intervention is clearly indicated. Relative contraindications include the patient’s condition, small body size, and obesity. The procedure becomes difficult in extremely small (is connected to a light source using a light guide cable. It is generally recommended that a high-intensity light source such as a xenon light source be used for laparoscopy.1 Light sources used for gastrointestinal endoscopy are generally sufficient for laparoscopy. A video camera attached to the telescope allows the image to be viewed on a video screen.Video- assisted laparoscopy is imperative when performing surgical procedures.
A Veress needle is used for the initial insufflation of the abdominal cavity. The needle consists of an outer cutting tip and, contained within the needle, a spring-loaded obturator that retracts into the needle shaft as it traverses the abdominal wall. Once in the abdominal cavity, the obturator is once again advanced beyond the sharp tip and prevents needle injury to internal abdominal organs. The needle is then connected to the automatic gas insufflator. Most automatic insufflators are similar and function to dispense gas at a prescribed rate while maintaining a predetermined intra-abdominal pressure.
Carbon dioxide is the gas most often used in order to prevent air emboli and spark ignition during cauterization.1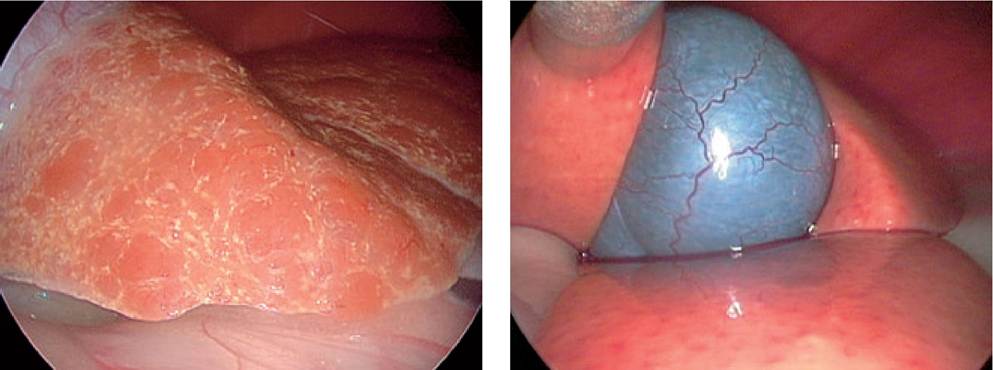
Figure 1.78:
Nodular liver. View of a nodular liver in a dog with hepatocutaneous syndrome.
Figure 1.79:
Idiopathic hepatic lipidosis. View of the liver and gallbladder of a cat with idio pathic hepatic lipidosis.
The trocar cannula units are required to enter the abdominal cavity and are of a corresponding size to receive either the telescope or the biopsy instruments. There are a number of different types of cannula units available but the most common ones consist of a sharp trocar housed in an outer cannula. Together they are used to penetrate the abdominal wall. Once in the abdomen, the trocar is removed while the cannula remains in place traversing the abdominal wall and it becomes a portal for the introduction of the telescope or instruments into the abdominal cavity while maintaining the pneumoperitoneum.
Common accessory instruments include a palpation probe used to move and palpate abdominal organs and biopsy forceps. The author prefers a 5-mm diameter biopsy forceps with oval biopsy cups to obtain liver, spleen, abdominal mass, and lymph node biopsies. A variety of other biopsy forceps, tissue graspers, and aspiration needles are also available for diagnostic laparoscopy. A “true-cut” type or similar biopsy needle is required for both kidney and deep tissue biopsies. Biopsy needles are passed directly through the abdominal wall and guided to the area to be sampled without the need for a cannula.
1.6.3.2 Procedural considerations
The patient should be fasted for at least 12 hours before the procedure and the urinary bladder should be evacuated. Laparoscopy is commonly performed using general gas anesthesia and most patients tolerate the anesthesia and laparoscopy well.5,6 In some situations, the author will perform diagnostic laparoscopy using only heavy sedation in conjunction with local anesthesia at the entry sites.
In order to select the appropriate cannula portal placement sites, one must first determine the objectives of the laparoscopic procedure. The two most common approaches are a right lateral and a midline approach. The right lateral approach is recommended for diagnostic evaluation of the liver, gallbladder, right limb of the pancreas, duodenum, right kidney, and the right adrenal gland. A ventral approach is useful for many operative procedures, and offers good visualization of the liver, gallbladder, pancreas, stomach, intestines, reproductive system, urinary bladder, and spleen. With the ventral approach, visualization is sometimes hindered by the location of the falciform ligament. A complete description of a step-by- step technique of the laparoscopy procedure is beyond the scope of this chapter and has been previously described.1
1.6.4