Cardiac Murmurs
Throughout the cardiovascular system, blood has a laminar or streamlined flow, except in the heart and sometimes in the aorta. Occasionally conditions occur that cause turbulent flow that is sufficient to cause resonance in adjacent structures.
This resonance may be heard as a murmur when a critical level of turbulence is reached (Boxes 6.5 and 6.6). The factors that determine whether blood flow is laminar or turbulent are related by the Reynolds number, which is the ratio of the inertial to viscous forces. When the Reynolds number exceeds■ BOX 6.5
Causes of Cardiac Murmurs in Horses Common Causes
Valvular regurgitation
Congenital defects
Anemia
Excitement
Fever
Functional murmur
Exercise
Uncommon Causes
Aortic cardiac fistula
Aortopulmonary fistula
Cardiomyopathy
Pericarditis
Cranial mediastinal abscess
■ BOX 6.6
Causes of Cardiac Murmurs in Ruminants
Common Causes
Anemia
Excitement
Fever
Functional murmur
Valvular regurgitation
Congenital defects
Lymphosarcoma
Pericarditis (usually traumatic reticulopericarditis)
Uncommon Causes
Cardiomyopathy
Myocarditis a critical value (about 2000 in large vessels), turbulence occurs. Increased flow velocity or reduced blood viscosity (e.g., anemia) predisposes to murmur development. The characteristics of the murmur depend on the velocity of the blood flow and the nature of the structures that vibrate.
It is useful to characterize murmurs with regard to timing in the cardiac cycle (systolic, diastolic, or continuous); duration in the cardiac cycle (early, mid, late, holo-, pan-); intensity (loudness); shape and quality or frequency; PMI; and radiation of the murmur. Systolic murmurs occur any time between the first and second heart sound. Diastolic murmurs occur between the second and first heart sounds.
Continuous murmurs occur throughout the cardiac cycle (Fig. 6.4). The intensity of murmurs is frequently graded on a scale of 1 to 68:• Grade 1 is a soft murmur heard only after minutes of careful listening.
• Grade 2 is a soft murmur heard immediately on auscultation.
• Grade 3 is a murmur of moderate intensity.
• Grade 4 is a loud murmur associated with a faint palpable thrill.
• Grade 5 is a loud murmur with a palpable thrill but is not heard when the stethoscope is removed from the chest wall.
• Grade 6 is a loud murmur with a palpable thrill and is audible with the entire stethoscope chest piece held away from the chest wall.
The PMI of a murmur usually corresponds to the location of one of the heart valves. Murmurs associated with the mitral valve will frequently be heard best in the left fifth intercostal space just dorsal to the level of the elbow. These murmurs usually radiate dorsally or toward the aortic valve area. Pulmonic valve and aortic valve murmurs are best heard at the base of the heart. For this area to be accessed, the hand is moved under the left triceps muscle to the third (pulmonic) and fourth (aortic) intercostal spaces just below the level of the shoulder. Murmurs associated with the tricuspid valve are frequently located in the right third or fourth intercostal space between the shoulder and elbow.
Most systolic murmurs fall into one of two categories: ejection or regurgitant (see Fig. 6.4). Systolic ejection murmurs are caused by obstructed, increased, or turbulent blood flow across normal or damaged semilunar valves. Valvular obstruction is rare in large animals, but functional ejection murmurs are commonly found in healthy horses. The diagnostic considerations for systolic ejection murmurs are given in Box 6.7. The PMI of the innocent or functional murmur is typically at the pulmonic or aortic valve or just dorsal to them over the great vessels. It is a crescendo-decrescendo murmur that is audible in early to mid systole.
The functional murmur may be distinguished from a pathologic murmur by being of lower and variable intensity,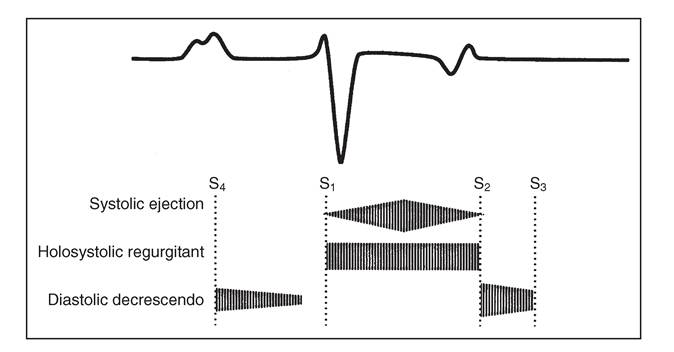
FIG. 6.4 Phonocardiographic characteristics of systolic ejection, holosystolic (pansystolic) regurgitant, and diastolic decrescendo cardiac murmurs.
■ BOX 6.7
Possible Causes of Ejection and Regurgitant Systolic Cardiac Murmurs
Ejection
Innocent murmur
Anemia
Fever
Aortic stenosis
Pulmonic stenosis Atrial septal defect Ventricular septal defect Tetralogy of Fallot
Regurgitant
Mitral regurgitation Tricuspid regurgitation Ventricular septal defect Tetralogy of Fallot
peaking in early to mid systole, ending well before the second heart sound, and having no radiation. The physiologic systolic ejection murmur may disappear or become louder after exercise. Diagnostic considerations for systolic regurgitant murmurs are listed in Box 6.7.
Regurgitant murmurs can be variable in duration and may occur in early, mid, or late systole or can be pansystolic or holosystolic. Location of the PMI and the direction of radiation of the systolic murmur distinguish mitral or tricuspid regurgitation from a ventricular septal defect (VSD). Systolic clicks are rare in horses and cattle but may indicate abnormalities of the chordae tendineae, AV valve prolapse, or dilation of the aorta. The presence of a musical murmur indicates vibration of a cardiac structure such as rupture of one of the chordae tendineae or a torn valve leaflet.
Diastolic murmurs can occur between S4 and S1 (atrial systolic murmurs), between S2 and S3 (ventricular filling murmurs), or from S2 to S1 (aortic regurgitation or, rarely, pulmonic regurgitation). Both the atrial systolic and ventricular filling murmurs are usually functional, can be heard over the left or right hemithorax, and can vary in intensity. They may have a musical or “squeaky” quality.
The aortic regurgitation murmur is typically a decrescendo murmur with its PMI over the aortic valve that begins immediately after S2 (see Fig. 6.4). Some aortic regurgitation murmurs can be harsh or musical, associated with high-frequency vibrations of an aortic valve leaflet, and they are often audible over the right thorax, although with lesser intensity.Continuous murmurs are uncommon in horses and ruminants. Patent ductus arteriosus, a finding in normal foals for a short time after delivery, can be heard in the left third intercostal space. This murmur can be continuous, but more frequently only a residual systolic murmur is audible.9 Continuous machinery murmurs are most frequently reported in adult horses with an aortic cardiac fistula secondary to rupture of the aortic root or of a sinus of Valsalva aneurysm. If both a systolic and diastolic murmur or a continuous murmur are heard in the aortic to pulmonic valve area in a Friesian horse, an aorticopulmonary fistula should be considered.10 Most acquired systolic and diastolic murmurs in adult horses or cattle are usually the result of separate murmurs but can sometimes be confused. A continuous “washing machine” murmur/rub, which is most easily heard over the left cardiac area, is associated with traumatic pericarditis in cattle and is caused by the accumulation of fluid, gas, and fibrin within the pericardium.
Approach to Diagnosis of Cardiac Murmurs
1. Take a history. Note the age, onset, duration, and progression of the condition. Determine exercise capability, growth, and attitude; inquire about previous fever, illness, or medications.
2. Perform a physical examination. Record the animal's vital signs. Determine timing, duration, intensity, location of PMI, shape, and radiation of murmur. Palpate peripheral arterial pulse and observe the jugular vein for distention and pulsations. Carefully auscultate the lungs at rest and during deep inspiration.
3. Obtain blood for CBC (includes fibrinogen, SAA, and total plasma protein concentration).
4. Test serum or plasma for the following:
a. Electrolyte concentrations
b. Bovine leukosis virus (BLV), AGID status (cows)
c. Cardiac troponin I or cTnT if myocardial inflammation, injury, or necrosis is suspected7
5. Record an ECG.
6. Perform an echocardiogram to look for valve abnormalities, abnormalities of the aortic root, congenital defects, chamber enlargement, and wall motion abnormalities; use pulsed wave and color flow Doppler echocardiography to localize the shunt, regurgitant blood flow, or stenosis (rare); use color flow and continuous wave Doppler echocardiography to estimate the severity of the jet associated with a shunt, valvular regurgitation, or stenosis (rare); estimate pulmonary artery pressure by applying the Bernoulli equation to tricuspid or pulmonic regurgitant jet velocities, if present. Contrast echocardiography can also be used for examination of congenital defects and detection of an aortic cardiac fistula and some valvular insufficiency. Tissue Doppler imaging and speckle tracking can be used to further assess myocardial function.11
7. Take radiographs or perform thoracic ultrasonography to find evidence of pulmonary edema or pleural effusion.
8. Catheterize the right heart to determine pulmonary artery and wedge pressures, which may complement data obtained noninvasively with Doppler echocardiography.
Muffled Heart Sounds
Auscultation of heart sounds requires that the vibrations generated by the heart be transmitted through the tissues of the thorax to the outer chest wall with sufficient amplitude to be heard. Blood transmits sound well, whereas lung tissue strongly attenuates sound waves. The chest wall itself causes attenuation of the sound that is most significant at the interface between bone and muscle. Therefore physical factors in a normal patient, such as a large, thick chest or obesity, can cause heart sounds to be muffled. If the environment for auscultation is conducive to hearing heart sounds, other factors such as stethoscope quality may cause muffling of heart sounds in a normal patient.
One should strive to have a stethoscope with comfortably fitting earpieces; thicker and shorter tubing; a rigid diaphragm to hear S1, S2, and higher-frequency sounds; and a bell piece for auscultation of S3, S4, low-frequency sounds, and murmurs. If the overlying hair coat is thick, clipping the hair may be necessary for optimal contact of the stethoscope to the skin.Heart sounds are muffled primarily because of displacement of the heart from the thoracic wall by fluid (pericardial effusion), a soft tissue mass (abscess or tumor), or air (pneumothorax, pneumomediastinum, or emphysema) (Boxes 6.8 and 6.9). Rarely is muffling of heart sounds attributed to weak cardiac contractions alone, although this may be a finding in recumbent, hypocalcemic cows.
Approach to Diagnosis of Muffled Heart Sounds
1. Take a history. Inquire about any change in attitude, appetite, diet, or posture; determine whether a magnet has been administered to cattle; note any history of fever, weight loss, respiratory disease, colic, or diseases of other body systems and the deworming history; determine whether cattle are known to be BLV positive. Determine whether the horse had possible exposure to Eastern Tent caterpillars.12
■ BOX 6.8
■ BOX 6.10
Causes of Muffled Heart Sounds in Horses
Common Causes
Obesity
Large or thick chest wall
Pericarditis or pericardial effusion
Neoplasia: lymphosarcoma
Pleural abscess
Chronic heart failure
Uncommon Causes
Pulmonary emphysema
Pneumothorax
Neoplasia: mesothelioma, squamous cell carcinoma, fibrosarcoma
Causes of Exercise Intolerance, Weakness, and Syncope in Horses*
Common Causes
Myocardial disease
Cardiac arrhythmias
Aortic or pulmonary artery rupture
Aortoiliac-femoral thrombosis
Congenital heart defects
Chronic heart failure
Pericardial disease
Hyperkalemic periodic paralysis
*See Chapters 8, 13, 31, 41 and 42 for additional noncardiac causes.
■ BOX 6.11
■ BOX 6.9
Causes of Muffled Heart Sounds in Ruminants
Common Causes
Obesity
Large or thick chest wall
Pericarditis (traumatic reticulopericarditis)
Neoplasia: lymphosarcoma
Pleural abscess
Chronic heart failure
Emphysema
Uncommon Causes
Pneumothorax
Idiopathic hemorrhagic pericardial effusion
2. Perform a physical examination and determine vital signs. Carefully auscultate the lungs to establish whether there is ventral dullness or evidence of increased or added sounds from pulmonary parenchymal compression; carefully auscultate the heart for pericardial friction rubs; determine whether there are signs of CHF (jugular venous distention, peripheral edema); percuss the thorax to determine whether there is emphysema, pleural fluid, or pneumothorax; note that pleural fluid in the absence of pericardial effusion causes radiating heart sounds but absence of airway sounds; determine whether there is thoracic and/or abdominal pain; and in cattle, check for the presence of a reticular magnet using a compass or stud finder.
3. Obtain blood for the following:
a. CBC
b. Fibrinogen concentration
c. SAA concentration
d. Plasma or serum protein concentration
e. Liver enzymes and tests for liver function (AST, SDH, alkaline phosphatase, GGT, bilirubin, and bile acid concentration)
f. Tests for kidney function (urinalysis, creatinine, blood urea nitrogen [BUN], Na, K, Cl, P concentrations, and fractional excretion of Na, Cl, P)
4. Test serum for BLV serology and for equine influenza, viral arteritis, and herpes virus.
5. Take radiographs of the thorax to determine whether there is pulmonary parenchymal and/or pleural or pericardial disease.
6. Perform an ECG.
7. Perform a thoracic ultrasound examination/echocardiogram to determine if there is pericardial or pleural fluid, a cardiac mass, or a mass in the cranial mediastinum compressing the heart. Determine the location and type of fluid present.
Causes of Exercise Intolerance, Weakness, and Syncope in Ruminants*
Common Causes
Myocardial disease Cardiac arrhythmias
Congenital heart defects Chronic heart failure
*See Chapters 8, 13, 31, 41 and 42 for additional noncardiac causes.
8. Analyze pericardial or pleural fluid, and perform culture and sensitivity testing if indicated.
Cardiovascular Exercise Intolerance, Weakness, and Syncope
Exercise intolerance, weakness, or syncope can be a clinical sign associated with disease in many body systems. Exercise intolerance can be manifested as sudden deceleration or stopping, failure to perform at an expected level, a sudden change in the level of performance or production, lowered enthusiasm for work, cough on exertion, evidence of respiratory distress, or excessive sweating. Weakness can be manifested as recumbency, difficulty in rising from recumbency, muscle tremors or fasciculations, reluctance to move, or toe dragging. Syncope is a sudden collapse and loss of consciousness (fainting).
Mechanisms of Cardiovascular Exercise Intolerance, Weakness, and Collapse
The clinical signs of exercise intolerance, weakness, or collapse can be caused by cardiovascular disease (Boxes 6.10 and 6.11). They are the result of failure to maintain cardiac output, caused by inability to regulate either heart rate or stroke volume. A normal horse increases cardiac output at submaximal heart rates (beats can reduce cardiac output even at submaximal heart rates.16 Horses with cardiac arrhythmias can have abnormal elevations in lactate concentration in response to exercise, indicating a lower anaerobic threshold and leading to exercise intolerance.17,18 Bradyarrhythmias cause exercise intolerance and/or collapse via failure to maintain an adequate heart rate at rest or by failing to adequately increase heart rate to meet the increased cardiac output demands during exercise. Complete heart block and advanced second-degree heart block are the most common bradyarrhythmias to cause clinical signs.
Cardiac output maintenance may also be compromised in animals by diseases affecting myocardial contractility or diseases that result in increased end-systolic volume despite a submaximal heart rate.19 Diseases that result in decreased venous return (peripheral vascular disease) can also reduce cardiac output and cause signs of exercise intolerance, weakness, or collapse.
Exercise intolerance or weakness can also be caused by painful peripheral vascular conditions or conditions causing peripheral hypoxia or lactic acid accumulation. In horses, such conditions may exist with aortoiliac thrombosis. Sudden episodes of weakness and collapse without change in consciousness are associated with hyperkalemic period paralysis in horses (see Chapter 42).
Collapse may be associated with epilepsy, narcolepsy, or other central nervous system (CNS) disturbance. If cardiovascular and pulmonary function appear normal, the nervous system should be examined in detail (see Chapter 8). Collapse at rest may also be caused by sleep disorders or poorly defined mechanisms such as girth tightening. Collapse during exercise is most commonly caused by cardiovascular disease, whereas collapse at rest is usually associated with neurologic disease.
Approach to Diagnosis of Exercise Intolerance, Weakness, and Collapse
1. Note signalment and take history. Establish onset of problem, previous performance history, activity level, and whether there is loss of consciousness when clinical signs are observed. Determine whether there is coughing, dyspnea, or excessive sweating associated with stress or exercise. Determining whether the weakness or collapse primarily occurs with exercise or at rest will direct further workup.
2. Perform a physical examination and record vital signs. Of particular importance are heart rate at rest, peripheral arterial pulse characteristics, presence of pulse deficits, mucous membrane color, and appearance of jugular venous pulses. Lungs should be auscultated for evidence of pulmonary edema or pleural effusion. The chest should be percussed. Rectal examination should be performed to evaluate aortic and iliac arterial pulses; metatarsal artery pulses and saphenous vein refill should be evaluated.
3. Perform neurologic and lameness evaluations. Perform a rectal ultrasound examination if aortoiliac thrombosis is suspected, to document the disease and assess its severity.
4. Perform an echocardiogram (2D, M-mode, and Doppler) to evaluate the size of heart chambers; to look for congenital defects, acquired valvular heart disease, and pericardial disease; and to evaluate myocardial contractility and ventricular wall motion. Tissue Doppler imaging and speckle tracking can also be used to further evaluate atrial and ventricular wall motion.11
5. Record an ECG at rest. Record a continuous 24-hour ECG to determine the frequency of arrhythmias detected on the resting ECG or to look for infrequent or paroxysmal arrhythmias not detected at rest.
6. Simultaneous video monitoring and continuous ECG recording can help determine if episodes of collapse are associated with cardiac rhythm disturbances. Video surveillance can also help characterize the nature of the collapse episodes and aid in differentiation of seizure activity from sleep disorders.20
7. If collapse is associated with exercise and a definitive diagnosis cannot be made with resting diagnostics, an exercising stress test should be performed. Diagnostics may include resting and exercising upper airway endoscopy, an exercising ECG (preferably with real-time monitoring), stress echocardiogram before and immediately after exercise, resting and exercising lactic acid and arterial blood gas concentrations, resting and postexercise creatine kinase, and cTnI or cTnT concentrations and a postexercise bronchoalveolar lavage. Clinicians should be prepared to discontinue the test, treat life-threatening arrhythmias, and/or establish a patent airway (tracheostomy) in horses with a history suggestive of ventricular arrhythmias or upper airway obstruction, particularly pharyngeal collapse or laryngeal dysfunction.
Venous Distention and Pulsations
The jugular venous pulsations observed in the neck are primarily a reflection of right atrial and right ventricular activity. There may be some small contribution from carotid arterial impact.21 The jugular venous pulse reflects the right atrial or central venous pressure, which is influenced by blood volume, right ventricular cardiac output, and right atrial contractility (Boxes 6.12 and 6.13). Jugular venous pulsations are observed in normal animals, but the pulse seldom radiates more than one third of the distance from the thoracic inlet to the ramus of the mandible when the head is held in a normal, upright position.
Mechanisms of Venous Distention and Pulsations
The normal jugular venous pulse consists of three positive and two negative deflections (Fig. 6.5). The first and dominant positive wave is the A wave, produced by atrial contraction. During atrial relaxation the pressure declines until ventricular systole. The second positive deflection is the C wave, which is produced by the bulging of the tricuspid valve leaflets into the right atrium during early (isovolumetric) right ventricular systole. Carotid arterial impact on the jugular vein may also contribute to the C wave.21 As the ventricle contracts, the plane of the tricuspid valve is pulled toward the apex of the
■ BOX 6.12
Causes of Jugular Venous Distention and Pulsation in Horses
Common Causes
Right-sided heart failure
Left-sided heart failure with pulmonary hypertension Cardiomyopathy
Atrial fibrillation
Tricuspid regurgitation
Cranial mediastinal mass
Lymphosarcoma
Abscess
Jugular venous phlebitis and thrombosis
Uncommon Causes
Ionophore toxicity
Pericarditis
Myocarditis
Ventricular tachycardia
Squamous cell carcinoma
Fibrosarcoma
Cor pulmonale
Chronic obstructive pulmonary disease Overhydration
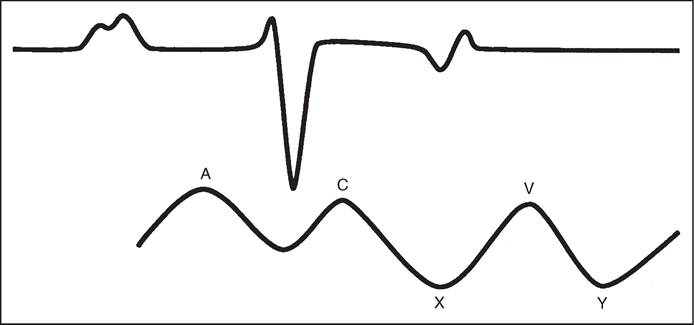
FIG. 6.5 Schematic illustration of a venous (jugular or atrial) pressure curve and its relationship to events of the electrocardiogram. A, Positive wave produced by atrial contraction; C, second positive deflection caused by bulging of the tricuspid valve during isovolumetric systole; X, first negative wave produced by the plane of the atrioventricular valve being pulled toward the apex of the heart during systole; V positive pressure wave caused by venous return; Y, negative wave produced by AV valve opening.
■ BOX 6.13
Causes of Jugular Venous Distention and Pulsation in Ruminants
Common Causes
Right-sided heart failure
Left-sided heart failure with pulmonary hypertension Vitamin E or selenium deficiency (white muscle disease) Cardiomyopathy
Tricuspid regurgitation Pericarditis
Jugular venous phlebitis and thrombosis
Heart base tumor: lymphosarcoma
Heart base abscess
Cor pulmonale caused by chronic pneumonia Brisket disease
Uncommon Causes
Ionophore toxicity
Idiopathic hemorrhagic pericardial effusion Overhydration
Cranial mediastinal mass
heart and the atrial pressure declines, producing the X descent. The X descent is terminated by the V wave, which is associated with venous return, subsequent atrial filling, and a closed tricuspid valve. At the end of ventricular systole, the atrial pressure falls again as a result of tricuspid valve opening and rapid right ventricular filling. This is the Y descent. The Y descent is terminated as the pressure gradually rises with right-sided heart filling.
Abnormal pulsations occur with increased resistance to right ventricular filling, regardless of the cause. Distention and pulsations in the jugular vein are usually associated with an elevated right ventricular pressure such as occurs in right-sided heart failure, constrictive pericarditis, or, more rarely, cardiomyopathy. Prominent jugular pulsations are noted with tricuspid regurgitation and certain cardiac arrhythmias, especially those arrhythmias associated with atrial contraction against a closed AV valve. The carotid arterial pulse can mimic jugular venous pulsations. To distinguish among the causes of jugular venous pulsations, lightly compress but do not occlude the jugular vein at the thoracic inlet. The jugular vein will distend enough to eliminate carotid arterial pulsations. If pulsations are still present, tricuspid regurgitation, atrial arrhythmias, or rightsided heart failure should be considered. If the jugular vein is compressed near the ramus of the mandible and massaged toward the thoracic inlet, refilling is indicative of tricuspid regurgitation. Jugular venous distention without pulsations can occur with compression of the cranial vena cava from a cranial thoracic or mediastinal mass or from occlusion of the jugular vein with a thrombus.
Approach to Diagnosis of Venous Distention and Pulsations
1. Take history. Note especially history of respiratory disease, exposure to high altitude and locoweed, or ingestion of potential cardiotoxins. Determine whether other animals have been similarly affected, whether the BLV status of affected cattle is known, and whether a magnet has been administered.
2. Perform a physical examination. Determine whether there is tachypnea or tachycardia. Carefully auscultate for abnormal heart sounds, rhythm, or intensity of sounds; note whether jugular veins are patent. Look for jugular venous pulsations as described previously.
3. Obtain blood for the following:
a. CBC
b. Fibrinogen concentration
c. SAA concentration
d. Total protein concentration
e. BLV status (bovine) and serology for equine influenza, viral arteritis, and herpes virus
f. Vitamin E (serum) and selenium concentrations if cardiomyopathy suspected
4. Take radiographs of the thorax and abdomen to establish whether there is respiratory disease, a magnet, or a penetrating foreign body.
5. Record an ECG when there is an arrhythmia to look for atrial premature depolarizations.
6. Perform an echocardiogram to examine the following:
a. Right ventricular size and function
b. Right atrium, for abnormal size or structures
c. Tricuspid valve
d. Pulmonary artery diameter looking for evidence of
ι y ι y b
pulmonary hypertension
e. Left atrial size
f. Left ventricular size and function
g. Pericardium
h. Interventricular septal thickness and motion
7. Perform Doppler echocardiogram to look for:
a. Tricuspid regurgitation
b. Pulmonic regurgitation
c. If tricuspid or pulmonic regurgitation is detected, check for concurrent mitral and aortic regurgitation. Use velocity of tricuspid and/or pulmonic regurgitation to calculate/estimate pulmonary artery pressure.
■ BOX 6.14
■ BOX 6.15
Causes of Painful Peripheral Swellings in Horses
Common Causes
Thrombophlebitis
Abscess (Corynebacterium pseudotuberculosis in western United States)
Cellulitis
Hypersensitivity vasculitis (complicated by skin necrosis and secondary infection)
Equine viral arteritis
Equine granulocytic ehrlichiosis (Anaplasma phagocytophilum, formerly Anaplasma equi or Ehrlichia equi)
Equine infectious anemia
Purpura hemorrhagica
Clostridium species myositis
Septic tenosynovitis Bursitis
Muscle disruption/hematoma
Fracture
Insect bite
Application of topical counterirritants, firing, or soring
Uncommon Causes
Frostbite
Piroplasmosis
Ulcerative lymphangitis
Epizootic lymphangitis Glanders
Melioidosis
Sporotrichosis Immune vasculitis
Aortoiliac thrombosis
Sporadic lymphangitis
Congenital lymph node and lymphatic dysgenesis Hemangiosarcoma
Snakebite
8. Perform ultrasound examination of the cranial thorax and cranial mediastinum.
9. Performing jugular venous catheterization may be useful to determine right atrial (central venous), right ventricular, and pulmonary arterial pressures.