Clinical andDiagnostic Findings
Cholecystitis is seen most commonly in older animals (median age 9½ years) with no apparent breed or sex predilection (Church and Mathiessen 1988), although one study showed an overrepresentation of Dachshunds (Lawrence et al.
2015).Cholecystitis may be acute or chronic in nature. Signs of acute cholecystitis include abdominal pain (may only be postprandial), anorexia, vomiting, pyrexia, and icterus. Some animals may present with signs of hypodynamic shock especially when GB rupture or bile peritonitis is present. Signs of chronic cholecystitis are more vague, with a waxing and waning nature, making a diagnosis of chronic cholecystitis more challenging. Clinical signs may include intermittent anorexia, vomiting, and progressive weight loss.
Diagnosis is based on clinical signs, clinico- pathologic features, and ultrasonographic imaging findings. Laboratory abnormalities present in cases of cholecystitis are very nonspecific and indistinguishable from other hepatobiliary diseases. Abnormalities seen may include variable leukocytosis, with or without toxic neutrophils or a left shift, hyperbilirubinemia and moderate to marked increases in liver enzyme activity, especially ALP and GGT. Abdominal radiography may reveal indistinct detail in the cranial abdomen consistent with focal peritonitis or rarely; the GB wall may become radio-dense due to dystrophic mineralization secondary to chronic inflammation. Choleliths may also be seen and in cases of emphysematous cholecystitis, a spherical to ovoid gas opacity superimposed over the hepatic silhouette may be present.
Ultrasonography is the current gold standard for diagnosis of cholecystitis in small animals. Common ultrasonographic abnormalities include a thickened GB wall (Figure 21.1), intraluminal echogenic debris, presence of choleliths, signs of EHBO, or emphysema of the GB wall (Richter and Pike 2014).
Pericholecystic fluid and omental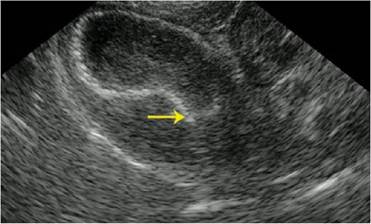
Figure 21.1 Ultrasound image of a dog with cholecystitis. There is a markedly echogenic and thickened gall bladder wall. The gall bladder is filled with echogenic fluid and sediment, and dilation of the proximal cystic duct also appears to be present (arrow).
adhesions may also be detected. Ultrasound is highly sensitive for the identification of GB rupture (86% sensitivity). Loss of GB wall continuity, hyperechoic fat in the cranial peritoneal cavity and presence of pericholecystic fluid or free abdominal fluid are all supportive of GB rupture (Richter and Pike 2014).
Percutaneous ultrasound-guided cholecys- tocentesis is also a relatively safe, minimally non-invasive diagnostic procedure that can prove useful in making both a diagnosis and in aiding in medical management of cases with cholecystitis. Bile samples should be sent for both cytological and aerobic/anaerobic culture with antimicrobial sensitivity testing. Complications of this procedure include intraperitoneal bile leakage, hemorrhage, hemobilia, bacteremia, and vasovagal reactions that may result in ventilator arrest, severe bradycardia, and death (Center 2009). To avoid bile leakage, it is recommended that the GB be drained completely during cholecystocentesis (Aguirre 2010).