Colitis
Acute and chronic colonic inflammation (colitis) commonly results in large bowel diarrhea in dogs and cats. Signs of colitis include excess fecal mucus, hematochezia, tenesmus, increased frequency of defecation, and reduced volume of feces per defecation.
Vomiting, anorexia, dehydration, and abdominal pain may also be observed. With concurrent small bowel involvement, melena and weight loss (chronic cases only) may also occur.Acute colitis is most commonly caused by dietary indiscretion or intolerance (see 9.1), toxin or foreign body ingestion, drug administration (antibiotics or NSAIDs), whipworm infestation (dogs only), Clostridiumperfringens enterotoxicosis, or may be idiopathic. Infections with Salmonella spp. or Campylobacter spp. are uncommon causes of acute colitis, and may cause both small and large bowel diarrhea. Diagnosis is based on history, fecal examination, and response to dietary management with a highly digestible, low fat, and low fiber diet, or exclusion of a source of dietary indiscretion. Colonoscopy and mucosal biopsy are rarely performed, so histological documentation of colonic inflammation is not often acquired, and the speculative diagnosis of acute colitis is based on the rapid resolution of diarrhea.
Chronic colitis is usually associated with IBD (see 9.2), or Clostridium perfringens enterotoxicosis (see below). Uncommon causes of colitis include histiocytic ulcerative colitis (see below), pythiosis (phycomycosis), and colitis associated with histoplasmosis, the colorless unicellular alga Prototheca spp., or Heterobilharzia americana (schistosomiasis).
6.4.2.1 Histiocytic ulcerative colitis of Boxers
Histiocytic ulcerative colitis (HUC) is an uncommon, chronic, idiopathic disease characterized by progressive colitis and ulceration (Figure 6.5), which is histologically associated with an inflammatory mucosal infiltrate of plasma cells, lymphocytes, and distended PAS-positive macrophages.20,21 The immunohistochemical characteristics of the inflammatory response have recently been characterized.4 The disease occurs most commonly in young Boxer dogs, less than 2 years of age, but has also been reported in a French Bulldog, a Mastiff, an Alaskan Malamute, and a Doberman Pinscher.22
Weight loss and debilitation occur as a result of chronic intestinal blood and protein loss.
A corrugated, thickened mucosa, hemorrhage, or pain may be evident on digital rectal examination.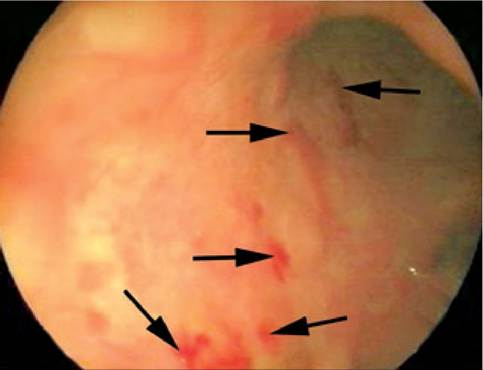
Figure 6.5:
Histiocytic ulcerative colitis. Endoscopic appearance of the descending colon in a 2-year-old Boxer with histiocytic ulcerative colitis. Erosions (arrows) and ulcers were present throughout the entire colon.
treatment with enrofloxacin at 2.5-5.0 mg/kg PO q 12 h for 4-8 weeks, may be more effective.23 However, more cases with a longer follow-up period need to be studied. Traditionally, if signs of HUC are severe at the time of diagnosis, a poor prognosis is warranted. Dogs with mild signs may respond well to traditional therapy.24
6.4.2.2 Clostridium perfringens enterotoxicosis
A preliminary review has associated large bowel diarrhea with Clostridium perfringens type A enterotoxin.34 The disorder occurs most commonly in dogs, but can occasionally be seen in cats. Both naturally occurring and hospital acquired cases have been described.35 Recently, several epidemiological studies have characterized the prevalence of Clostridium perfringens fecal enterotoxin in dogs with diarrhea, hospitalized dogs without diarrhea, and healthy outpatients.36-39 A concise description of this syndrome that is universally accepted has not yet emerged, and some of the syndrome’s characteristics remain controversial. The author believes that Clostridium perfringens enterotoxicosis is a common cause of chronic large bowel diarrhea in dogs and may also be an important cause of acute diarrhea. Many questions will hopefully be answered after the completion of case-based studies in which a definitive diagnosis is reached, the animals treated with appropriate antibiotics, and the clinical outcome is assessed.
Traditionally, treatment similar to that for IBD described in
9.2.2.4 has been suggested, with sulfasalazine being the drug of choice.
Recently, preliminary evidence is accumulating that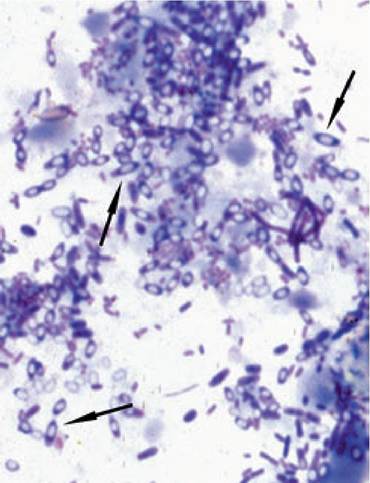
Figure 6.6:
Clostridium perfringensendospores. Huge numbers of clostridial endospores (arrows) in a rectal cytology specimen stained with a rapid Wright stain.
Pathophysiology
Clostridium perfringens is an anaerobic, spore-forming, grampositive bacillus.39 Five toxigenic types have been differentiated based on the production of one to four major toxins. In addition, each type can also produce other toxins. The majority of enterotoxin is produced by type A strains. A vegetative form of C.perfringens is a normal inhabitant of the colon.39 The enterotoxin is produced during sporulation and causes intestinal fluid accumulation, mucosal inflammation, alterations in mucosal tight junctions, increased mucosal paracellular permeability, and diarrhea.40 In some experimental models, the enterotoxin has its greatest effects within the small intestine. The stimuli for sporulation and enterotoxin production are unknown.
Clinical signs
Acute and chronic large bowel diarrhea commonly occur with Clostridium perfringens enterotoxicosis. Vomiting, weight loss, flatulence, and abdominal pain are seen less frequently. Small bowel diarrhea may also occur, but a causal relationship with C. perfringens is somewhat controversial. A syndrome of acute hemorrhagic diarrhea in dogs has been strongly associated with the presence of both C. perfringens and C. difficile enterotoxins in their feces.36 The syndrome described in that study was characterized by acute hemorrhagic diarrhea, hematemesis, severe dehydration, and necrotizing hemorrhagic enteritis and mesenteric lymphadenopathy on necropsy.
Diagnosis
The diagnosis is confirmed by identifying the enterotoxin in the feces from a dog or cat with typical clinical signs, which lack evidence of another large bowel disease. The clinical signs should rapidly improve following antibiotic administration.
The only test currently available is a qualitative ELISA (TechLab, Blacksburg, VA). The test is available through some commercial diagnostic laboratories. In animals with intermittent signs, fecal samples should be collected when diarrhea is present, as the enterotoxin may not be found during asymptomatic periods. There is some suspicion that refrigeration may lead to unreliable results.41In the past, it has been suggested that diagnosis of this enterotoxicosis should be suspected when more than 3-5 spores per oil immersion field are seen in a rectal cytology specimen. The spores are larger than most bacteria and assume a “safety pin” appearance (Figure 6.6). However, recent epidemiological studies have not demonstrated a consistent relationship between the number of fecal spores and the presence of enterotoxin.37,38 However, dogs with signs of large bowel diarrhea have been associated with large numbers of spores on rectal cytology.36 In the author’s experience, large numbers of spores on rectal cytology samples from dogs with typical clinical signs and diagnostic findings are usually associated with a positive test for fecal enterotoxin and rapid clinical response to antibiotic treatment. However, the presence of fecal enterotoxin, typical clinical signs, and response to antibiotic treatment may also occur in dogs without an increase in spores on a rectal cytology sample. Although endoscopic examination of affected animals has been infrequently performed, the colon may be grossly and histologically normal or may show a hy- peremic, hemorrhagic, or ulcerated mucosa with histopathological findings of catarrhal or suppurative colitis.34
Treatment
Clinical signs in acute cases may resolve spontaneously. Affected animals usually respond to antibiotic therapy rapidly, within 3-5 days. Metronidazole at 6 mg/kg PO q 8-12 h, ampicillin at 22 mg/kg PO q 8 h, or amoxicillin at 11-22 mg/ kg PO q 8-12 h, for 7-10 days are all effective.34 Animals that develop recurrent clinical signs after treatment may require repeat therapy (1 or 2 additional times) or long-term therapy with tylosin (Tylan® powder) for 3-6 months, at 10-20 mg/kg PO q 12 h.
Tylosin powder has a bitter taste and may need to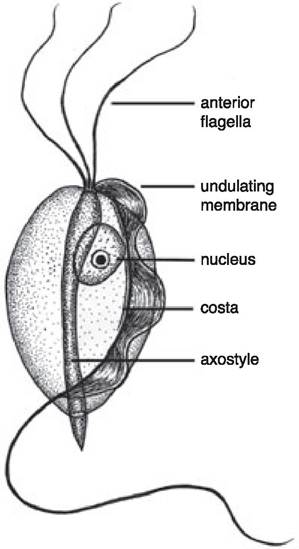
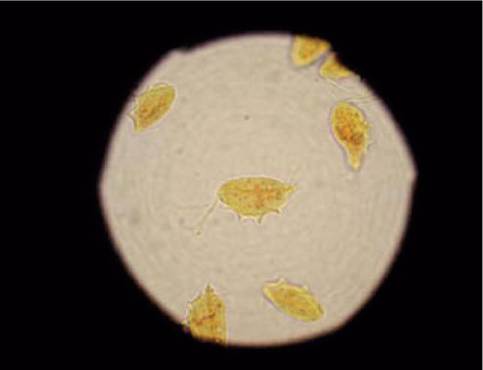
Figure 6.8:
Tritrichomonas foetus. Appearance of an individual T. foetus organism stained with Lugol's iodine solution. Three anterior flagellae and an undulating membrane that runs the length of the body can be seen. (Image reproduced with permission from www.fabcats.org; photograph by Andy Sparkes.)
Figure 6.7:
Tritrichomonas foetus. This line drawing shows a detailed outline of a Tritrichomonas foetus organism. As seen in Figure 6.8, the three flagellae and the undulating membrane are defining characteristics that can be used to differentiate T. foetus from other protozoal organisms on fecal examination. (Image reproduced with permission from supplemental visual material posted on the www for Biology 625 at Kansas State University; original line drawing by Jarrod Wood.)
be mixed with a small quantity of canned food or placed into a gelatin capsule. Some chronic recurrent cases benefit from feeding a high fiber diet. The proposed mechanisms of action for dietary fiber include bacterial fermentation of fiber, leading to acidification of the colon, which may inhibit sporulation, or an alteration of bacterial flora that inhibits C. perfrin- gens proliferation.
Prognosis
The prognosis for patients with Clostridium pefringens enterotoxicosis is excellent. Most affected animals respond to therapy within several days. At the present time, clinical findings have not been identified that can predict which patients will require long-term therapy.
6.4.2.3 Tritrichomonas foetus infection
Jan S. Suchodolski
Recently, Tritrichomonas foetus (Figures 6.7 and 6.8), a flagellated protozoal parasite that is usually associated with venereal trichomoniasis in cattle has been identified as an intestinal pathogen in cats.42,43 Diarrhea has been reported in cats after both experimental and natural infection.
Although the true prevalence of T. foetus infection in cats is unknown, it is suspected to be relatively high. In one study, 31% of 117 cats examined at an international cat show were found to be infected with Tfoetus.44While cats of any age, breed, or sex can be infected, young cats that are densely housed (e.g., cats in catteries, animal shelters, or multi-cat households) seem to be at an increased risk.43 Infection is most commonly seen in young cats (i.e., those that are less than 12 months of age) but older cats may also be infected. Tritrichomonas foetus primarily colonizes the surface of the colonic mucosa, leading to chronic large bowel diarrhea. Without appropriate treatment cats usually remain persistently infected. While the diarrhea may spontaneously resolve, infected cats will often experience recurrent bouts of diarrhea after being exposed to stress. Indeed, cats infected with T foetus generally appear healthy but show an increased frequency of defecation with loose to liquid stools, which may contain blood and/or mucus. Fecal incontinence is frequently observed. The anal region often appears edematous and may become painful with severe diarrhea. A rectal prolapse may occur in some cases.
Diagnosis
Diagnosis of a Tfoetus infection can be made by the identification of trophozoites on a direct fecal smear examination (Figure 6.8), fecal culture, PCR analysis of fecal material, or by colonic mucosal biopsy. The disadvantages of direct fecal smear examination include a low sensitivity (14%), low specificity (T foetus can be misdiagnosed as Giardia spp. or the non- pathogenic Pentatrichomonas hominis), and the fact that only fresh fecal samples can be used.
Tritrichomonas foetus can also be cultured in-house using the commercially available culture system In Pouch™ TF (Biomed Diagnostics, San Jose, CA). The pouches should be inoculated with less than 0.1 g of freshly voided feces and then incubated at 25°C. The pouches need to be evaluated under a microscope every couple of days. Results are usually obtained between 1 and 11 days after setting up a pouch. Although fecal culture is more sensitive than direct fecal smear examination, difficulties in the interpretation of results, the necessity of using freshly voided feces, and the fact that the results might not be available for up to 11 days, are important disadvantages of this method.
Tritrichomonasfoetus DNA can be amplified from fecal samples by PCR.45 PCR has been shown to be the most sensitive method for detecting Tfoetus in fecal samples, and is ideally suited for the direct diagnosis of Tfoetus infection.45 The advantages of PCR testing compared to culture include a higher sensitivity, faster turnaround time, and easier handling and storing of samples since DNA is relatively stable at various temperatures.
Therapy
Until recently, a successful treatment strategy for Tfoetus infections in cats was not available. However, a recent study has shown that administration of ronidazole (30-50 mg/kg PO q 12 h for two weeks) is effective in both resolving diarrhea and eradicating Tfoetus.46 There has been some anecdotal evidence that ronidazole may cause neurological side effects. However, these side effects appear to be reversible once therapy is discontinued. It should also be noted that ronidazole is not approved for use in domestic animals and it is recommended to obtain signed consent from the owner before initiating therapy. Recently, several compounding pharmacies have started offering ronidazole.
6.3.5