Conditions of Increased Body Temperature (Hyperthermia)
Body temperature disorders in which the core body temperature set point is unaltered can occur from increased heat production, absorption of heat, or impairment of heat loss. Central nervous system (CNS) disorders that disturb the hypothalamic regulatory center, certain drugs, and metabolic disorders may also cause temperature changes.
Regardless of the triggering cause, hyperthermia should be considered a medical emergency, and severely hyperthermic patients require immediate total body cooling, as temperatures above 107° F (41.6° C) may lead to permanent organ damage or death. Cooling options for the hyperthermic patient are discussed later in the “Heat Stroke” section.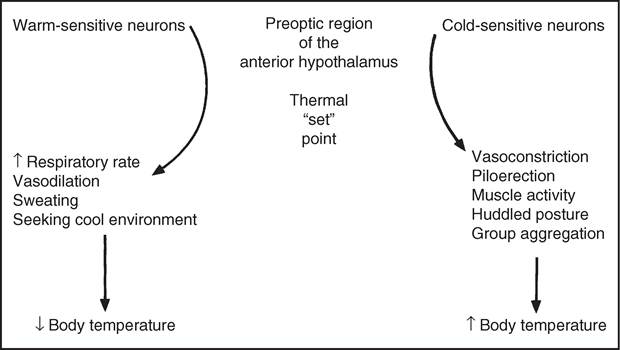
FIG. 4.1 Regulation of body temperature.
Malignant Hyperthermia
Malignant hyperthermia (MH) is a pharmacogenetic disorder of skeletal muscles that presents as a hypermetabolic response to potent volatile anesthetic gases such as halothane, sevoflurane, desflurane, and the depolarizing muscle relaxant succinylcholine and, rarely, in humans, to stresses such as vigorous exercise and heat.5 The classical signs of MH include marked hyperthermia, tachycardia, tachypnea, increased end-expired carbon dioxide production, increased oxygen consumption, acidosis, hyperkalemia, and muscle rigidity.5 The pathophysiology of MH involves an uncontrolled release of intracellular calcium from skeletal muscles' sarcoplasmic reticulum, resulting in sustained muscle contractions, increased oxygen consumption and carbon dioxide production, adenosine triphosphate (ATP) breakdown, and increased glycogen metabolism, which in turn generates heat.5 Although MH is most common in humans and pigs, it has been reported in horses.6-9 Of note, MH has also been reported in pot-bellied pigs.10 A dominant mutation of the ryanodine receptor 1 gene (RYR1), which is essential in skeletal muscle excitation-contraction coupling, is the basis of MH in humans, pigs, and dogs.11 The mutation has also been documented in Quarter Horses with MH and has an estimated prevalence of 1.3% in a random sample of 225 Quarter Horses.12-13 In all species, MH typically leads to death if it is not recognized and treated early (see also Malignant Hyperthermia, Chapter 42).
Exercise
During sustained exercise, heat production may exceed the ability of heat loss mechanisms, leading to a stable increase in core body temperature proportional to the intensity and duration of exercise.
The elevation in temperature often persists for several hours after exercise, but temperature returns to normal with rest as heat loss mechanisms remain activated. Body temperature increases of greater than 2° C (4° F) above normal during exercise, especially if reached early in exercise, are usually the result of severe environmental conditions and/ or failure in heat loss mechanisms. In one study looking at the effect of age on thermoregulation during exercise, old horses reached higher body temperatures faster and had greater sweat losses when compared with young horses.14 It is proposed that in horses, ageing affects the ability to handle the combined demand of exercise and thermoregulation in part due to a decrease in absolute preexercise plasma volume.14 Peripheral cooling to augment heat loss should be used to lower body temperature because increases in temperature caused by exercise are unaffected by antipyretic drugs.15-16The intense muscular activity associated with generalized tonic-clonic seizures may, like vigorous exercise, cause a rise in body temperature. If central heat regulatory systems are unaffected by the disease process, body temperatures return to normal no longer than 48 hours after the last seizure.17 Elevated temperatures that persist for longer periods should prompt investigation into other causes for the increased temperature. Similarly, hyperkalemic periodic paralysis of horses has also been associated with episodes of hyperthermia.18