Conjunctivitis and Keratoconjunctivitis
Infectious keratoconjunctivitis is known to the layperson as “pinkeye.” A number of etiologic agents have been incriminated. When only one or two animals are affected, it becomes more difficult to distinguish between an infectious and an irritant cause.
In fact, many sources of irritation, such as bright sunlight, dusty hay, and dust blown into the eyes by wind or transport in an open vehicle, can predispose the goat to development of an infection. Flies and hay or grass contaminated by ocular secretions can spread the agents to other goats. A herd outbreak may follow introduction of a carrier animal or attendance at a show.Another common source of irritation to conjunctiva and cornea is entropion. Entropion should be suspected in young kids with tearing; its management is discussed above. In an older animal with sudden occurrence of entropion, the possibility that a foreign body remains in the conjunctival sac or beneath the third eyelid must be considered and investigated by thorough examination.
Infectious Keratoconjunctivitis
Etiology
Mycoplasma and Chlamydia are currently believed to be the most common causes of outbreaks of keratoconjunctivitis in goats in the United States. Numerous other organisms are rarely the primary etiologic agent or are exotic to North America.
Mycoplasma
Mycoplasma conjunctivae has been isolated from naturally occurring cases or outbreaks of pinkeye in goats and in sheep, and has induced the disease in experimental studies (Barile et al. 1972; Baas et al. 1977; Trotter et al. 1977; Hadani et al. 2013). It also can exist in a carrier state in the conjunctival sac of clinically healthy eyes. Mild forms of the disease are self-limiting and last approximately 10 days, although clinical signs have been reported as persisting as long as 12 weeks. Other mycoplasma species isolated from goats with keratoconjunctivitis include Mycoplasma agalactiae, Mycoplasma mycoides subsp.
mycoides, large- colony type (McCauley et al. 1971; Bar-Moshe and Rapapport 1981), Mycoplasma capricolum (Taoudi et al. 1988), and Acholeplasma oculi (Al-Aubaidi et al. 1973). Because these agents can be associated with mastitis, pleuropneumonia, or arthritis, it may be easier to demonstrate the organism in other disease processes in the same goat. A report of M. mycoides var. capri from theUnited States (Jones and Barber 1969) possibly represented a misidentification of M. mycoides subsp. mycoides (DaMassa et al. 1984), but currently the large-colony strains are all included in M. mycoides subsp. capri (Brown 2010). Chlamydophila remains an important differential, especially if arthritis or pneumonia is concurrent.
Chlamydia
The name applied to the chlamydial species causing conjunctivitis in small ruminants was temporarily changed to Chlamydophila pecorum (Nietfeld 2001), but has since reverted to Chlamydia pecorum (Borel et al. 2018).
Chlamydial conjunctivitis has been recorded as a contagious disease of young goats and adults (Baas 1976; Eugster et al. 1977). In sheep, recurrence of chlamydial keratoconjunctivitis within a few weeks after clinical remission and an outbreak duration of several months have been recorded (Andrews et al. 1987). Lymphoid follicles are reported to develop in the conjunctiva early in the course of the disease.
Other Possible Agents
The isolation of a bacterium from the conjunctival sac of a goat with keratoconjunctivitis is not adequate proof of causality. It is possible that Moraxella (Branhamella)(Neisseria) ovis is sometimes involved in the pathogenesis (Bulgin and Dubose 1982; Bourdzi-Hatzopoulou et al. 1997). Conjunctivitis but not severe keratitis has been reproduced experimentally in goats using a strain of Moraxella (Branhamella) ovis isolated from an outbreak of keratoconjunctivitis (Bankemper et al. 1990), but this same organism appears to be common in normal eyes of goats, at least in some herds (Pitman and Reuter 1988).
Staphylococcus aureus has also been isolated from ocular swabs of healthy goats (Adegoke and Ojo 1982), as have Moraxella bovoculi and Staphylococcus equorum (Meekins et al. 2017). In cattle and sheep, Listeria monocytogenes has been associated with a keratitis resulting from direct inoculation of contaminated silage into the eye (Evans et al. 2004).Moraxella bovis, an important cause of pinkeye in cattle, is rarely involved in caprine keratoconjunctivitis. The organism is rod shaped, whereas Moraxella (Branhamella) ovis is a coccus. Commercial Moraxella vaccines have no place in caprine medicine. A very closely related species, Moraxella caprae, is also a rod and has been isolated from normal goats (Kodjo et al. 1995). The significance of this organism as a potential cause of keratoconjunctivitis is unknown.
Infectious bovine rhinotracheitis (IBR) virus has been isolated from a goat that developed severe keratoconjunctivitis after five days of treatment with an antibiotic preparation containing corticosteroid for respiratory disease (Mohanty et al. 1972). Most experimental inoculations of goats with the IBR virus have produced seroconversion but only mild clinical signs in addition to fever.
Borna disease is an infectious meningoencephalomyeli- tis of viral origin that affects horses and sheep in middle and eastern Europe and may be transmitted by ticks. Conjunctivitis and epiphora have been reported as ocular signs. Central nervous system involvement can lead to blindness as well as other neurologic signs. Antibodies have been found in goats, but spontaneous cases of the disease have rarely been reported in this species (see Chapter 5).
Before its global eradication, the rinderpest virus was noted to cause high fever and gastrointestinal disease, as does the virus that causes peste des petits ruminants (discussed in Chapter 10). Ocular signs of these infections include increased lacrimation and a serous conjunctivitis that turns mucopurulent. Gray, elevated fibrinonecrotic lesions in the conjunctiva may eventually slough, leaving an ulcer (Williams and Gelatt 1981).
Goats with capripox infections sometimes develop oculonasal discharge, conjunctivitis, and keratitis, in addition to fever and anorexia (Patnaik 1986). The typical skin lesions caused by the virus are discussed in Chapter 2.
Thelazia spp., the eyeworms, can cause conjunctivitis or keratitis in sheep and in goats. Thelazia rhodesii occurs in goats as well as cattle, sheep, and other species, and is cosmopolitan in Europe, Asia, and Africa. Thelazia californ- iensis is widely distributed in the United States, but goats are not mentioned as harboring the parasite (Soulsby 1982). The nematodes are small (7-18 mm) and slender. They may be found in the conjunctival cul-de-sacs, behind the third eyelid, or swimming across the surface of the cornea. The cornea may be cloudy. Sometimes they invade the nasolacrimal duct. Topical application of an avermectin, such as a drop or two of 1% moxidectin for injection, kills the parasite (Lia et al. 2004). Systemic levamisole or avermectins should also kill the worms (Pearce and Moore 2013; Kumar and Bachan 2016). Control of non-biting flies, which serve as vectors (Otranto and Traversa 2005), is desirable.
A single Setaria cervi worm longer than 2.5 cm (1 in.) was found in the aqueous humor of a goat in India. The goat exhibited continuous unilateral lacrimation. The worm was successfully removed under local anesthesia (Emaduddin 1954).
Migrating larvae of Gedoelstia hassleri (nasal botfly) cause keratoconjunctivitis and panophthalmitis in goats and other species in endemic areas of South Africa (Basson 1962, 1969). Trypanosoma brucei and Trypanosoma rhodesiense cause blepharo-conjunctivitis and keratitis in goats (Losos and Ikede 1972). In many tropical and subtropical countries, screwworm larvae may invade fresh wounds on the head or ocular tissues infected with keratoconjunctivitis. A foul odor and brownish exudate are produced. Other opportunistic fly larvae may then infest the lesions.
Besnoitiosis is a parasitic disease of goats as well as cattle and horses in southeastern Europe, the Middle East, Africa, and New Zealand, and of donkeys in the United States.
The causative agent in goats is a Besnoitia species, possibly different from B. besnoiti of cattle (Njenga et al. 1993). Cats that eat cysts in infected tissues develop an intestinal infection and excrete infective forms in their feces. Clinical signs in goats include dermatitis, alopecia, and infertility. Ocular cysts (white, elevated, sand-like foci) on the scleral conjunctiva are useful for field diagnosis of the infection (Bwangamoi et al. 1989; Oryan and Azizi 2008).Mycotic keratitis, although relatively common in horses, seems to be rare in ruminants (Wyman 1983) and specific reports in goats are lacking. Isolation and identification of the fungus are required before the diagnosis can be made. A chronic keratitis, plaque-like growths on the cornea, or severe keratomalacia might prompt attempts to perform scrapings or culture a fungus, especially if there is a history of treatment with antibiotics and corticosteroids together. Therapy is difficult and expensive. The practitioner should consult with an ophthalmologist.
Clinical Signs
Early or mild keratoconjunctivitis results in lacrimation; the side of the face is wet below the eye. The conjunctiva is also red and swollen (chemosis; Figure 6.6). Over several days, hyperemia of the conjunctiva increases, follicle formation occurs, and neovascularization of the cornea may develop. The cornea may be slightly hazy at the limbus or entirely opaque (Baxendell 1984). A few animals develop a

Figure 6.6 Early keratoconjunctivitis with chemosis and slight ocular discharge. Source: Courtesy of Dr. M.C. Smith.

Figure 6.7 A corneal ulcer is green from uptake of fluorescein stain. Marked neovascularization of the cornea indicates chronicity. Source: Courtesy of Dr. M.C. Smith.
corneal ulcer that can be demonstrated with fluorescein stain (Figure 6.7), and that ulcer may perforate.
The eye is painful and held partially closed; blinking is frequent. If both eyes are opaque or ulceration occurs, the goat will lose body condition because it does not forage well. Totally blind animals on range may starve (Eugster et al. 1977).Diagnostic Techniques
The various etiologic diagnoses for infectious keratoconjunctivitis cannot be distinguished on the basis of clinical signs; laboratory assistance is required. Mydriatics, topical anesthetics, or vital stains should not be used until after diagnostic samples have been taken.
Cultures
A premoistened sterile polyester or calcium alginate swab is rubbed briskly across the conjunctiva and placed in transport media (such as Amies). If possible, personnel at the diagnostic laboratory should be consulted regarding media, because chlamydia and mycoplasma can be difficult to isolate. Dry cotton swabs are less desirable for fastidious organisms. It is also important to take samples from early lesions; secondary bacteria, leukocytes, and various products of immune mechanisms interfere with isolation efforts.
Polymerase Chain Reaction
Polymerase chain reaction (PCR) methodology is increasingly being used for rapid identification of fastidious organisms. It is possible to identify the various species of chlamydia harvested from caprine conjunctiva, using a cytobrush or swab, by PCR (DeGraves et al. 2003). Likewise, M. conjunctivae (as well as other mycoplasmas) can be identified by PCR (Giacometti et al. 1999). If the laboratory does a PCR test, use of transport media may dilute the sample too much for good results.
Scrapings for Immunofluorescence Testing
Scrapings from the palpebral conjunctiva (especially lymphoid follicles) can be made with a wooden spatula designed for obtaining Pap smears, the butt end of a disposable scalpel blade, or with the bevel of a sterile, disposable 20-gauge needle. The tissue thus obtained is spread on several microscope slides. Fluorescent antibody testing for chlamydia may be more rapid and less expensive than culturing this agent or detecting its genome by PCR.
Exfoliative Cytology
Interpretation of cytological preparations from conjunctival scrapings can be very difficult, even for trained people. Practitioners should consider preparing duplicate slides to simplify later consultation with an ophthalmologist or diagnostic laboratory. Superficial cells can be harvested with minimal distortion by rolling a dry swab across the conjunctiva and then across the slide, as is done for canine vaginal smears. Deeper scrapings are obtained with a blade or small spatula. New methylene blue, Wright, Giemsa, Diff-Quik® (Siemens Healthineers, Erlangen, Germany), or Gram stain is typically used. Large basophilic, Gramnegative cytoplasmic inclusion bodies in epithelial cells occur with chlamydial conjunctivitis, but are difficult to find after the first week (Wyman 1983). Smaller basophilic coccobacillary (McCauley et al. 1971) and signet-shaped bodies are found attached to or within epithelial cells in mycoplasmal infections. Moraxella (Branhamella) ovis organisms are larger than mycoplasma and more uniform in shape, and stain more intensely (Dagnall 1994). Pigment granules or stain precipitates can be confusing, and visible evidence of an etiologic agent may be lacking, even when cultures are positive.
Treatment
The intensity of treatment varies according to the number of infected goats and the concern of the owner. Most goats will fully recover from infectious keratoconjunctivitis without treatment and sooner than if antibiotics are used extensively. What follows is most appropriate for goats with very painful eyes, impaired vision, or corneal ulcers. Milder signs might be treated in single pets or valuable animals. Isolation of the animal may be considered, although isolating affected animals with a herd mate may be less stressful. The eye should be irrigated with physiologic saline, sterile saline for contact lens wearers, hypochlorous acid spray, or clean (preferably previously boiled) water, to remove exudates and dust or other foreign matter. Although antibiotic drops are theoretically better than ointments, it is inconvenient for the owner to apply drops every two hours. Ointments are generally effective if given at least twice (or better, three to four times) a day. Several antibiotics have been clinically effective, but it must be remembered that many animals heal uneventfully without treatment. Given the spectrum of agents associated with keratoconjunctivitis, a tetracycline eye ointment is a reasonable choice. In countries where its use is permitted, chloramphenicol ointment might be effective, although systemic chloramphenicol was not effective in treating sheep with keratoconjunctivitis (Konig 1983). It is illegal to administer chloramphenicol to goats in the United States, because all goats are assumed to be food-producing animals regardless of the owner's plans for the individual.
Powders and aerosols are irritating to the eyes and ideally should not be used. When economics become an important consideration, as when many goats are affected or the whole herd is being treated simultaneously to try to end a prolonged epizootic, it may not be possible to use ophthalmic ointments; off-label topical application of mastitis ointment has been used. Intramuscular injections of long-lasting tetracycline have prevented relapses in sheep affected with M. conjunctivae and other agents (Konig 1983; Hosie 1988). Intramuscular tylosin (200 mg/goat/day) has afforded good results in goats treated early in the course of chlamydial keratoconjunctivitis (Eugster et al. 1977). Subcutaneous administration of these antibiotics might also be effective and less painful. Florfenicol concentrations in the tears of sheep have been investigated (Regnier et al. 2013). Intramuscular rather than subcutaneous injections at 40 mg/kg twice a day were necessary to achieve effective tear concentrations for at least 50% of the dosing interval; a single subcutaneous injection is unlikely to be effective. A newer macrolide antibiotic, tulathromycin, has not yet been evaluated for treating pinkeye in small ruminants, but is effective in treating keratoconjunctivitis due to Moraxella bovis in beef cattle (Lane et al. 2006). As pharmacokinetics of tulathromycin in goats are very similar to those in cattle (Young et al. 2011), it may be a useful treatment for pets and non-lactating goats. Milk contamination makes systemic antibiotic treatment unjustifiable in most dairy herds. In fact, the possibility of milk contamination from eye ointments has apparently not been investigated. Preliminary work suggests that a twice-daily hypochlorous acid spray is effective in treating pinkeye due to M. bovis in cattle, and this product might be considered when the use of antibiotics is not allowed (Gard et al. 2016).
Corticosteroids are available in many different topical and injectable preparations of varying anti-inflammatory effect and penetrating ability (Bistner 1986). Corticosteroids are not necessary and are contraindicated if an ulcer is present. A subconjunctival injection of a depot form of corticosteroid may be helpful to control neovascularization after extensive keratitis. The eye must be “quiet” and the cornea free of ulcers, as demonstrated by fluorescein staining, before such a treatment is performed. In general, it is best to dispense an ointment without steroids, because the owner is likely to use whatever product is on hand to treat undiagnosed eye problems of goats or other animals at a later date.
Ulcerated eyes should be observed several times a day for descemetocele formation. If perforation of the cornea appears imminent, a conjunctival flap, third eyelid flap, or tarsorrhaphy is indicated to protect and support the cornea.
The third eyelid flap is often easiest. Light tranquiliza- tion with xylazine may be necessary. Topical anesthesia with an ophthalmic anesthetic is performed. Paralysis of the eyelids is obtained by injection of 1-2% lidocaine (diluted if the goat is small) over the auriculopalpebral nerve. The injection site for the auriculopalpebral nerve is located caudal to the palpable arch of the zygomatic bone, immediately rostral to the base of the ear. Lidocaine should be “fanned” as it is injected at this location, in order to anesthetize any superficial or deep branches of the nerve. Small depots of lidocaine can also be injected over the suture sites. A 2-0 absorbable suture is passed through a rubber or plastic stent, and then through the full thickness of the upper lid and conjunctiva at the dorsal aspect of the lateral canthus. The suture is next passed through the free edge of the third eyelid, taking care not to penetrate the bulbar aspect of the third eyelid. The suture may be passed through the cartilage of the third eyelid for greater purchase. The suture is then passed outward through the conjunctiva and skin at the ventral aspect of the lateral canthus. The suture can be passed through a second rubber or plastic stent here. The surgeon should check to ensure that no exposed suture lies on the bulbar (ocular) side of the third eyelid. The suture is then tightened to pull the third eyelid across the cornea, and the suture is knotted on the surface of the eyelid skin, creating a horizontal mattress pattern (Moore and Whitley 1984; Irby 2017). Follow-up care includes continued therapy with antibiotic ointment and close observation for loosening of the sutures. Absorbable sutures dissolve in two to three weeks.
As a simpler alternative to surgery for severe corneal ulcers, the author (MCS) has seen excellent response to topical 5% silver nitrate, a few drops applied once a day for five days in conjunction with systemic oxytetracycline. This solution is not available commercially, but can be approximated by dissolving the material coated onto one Grafco® (Graham Field, Atlanta, GA, USA) silver nitrate applicator stick in 1 mL of sterile water. The totally opaque soft cornea is firm and shiny again in a few days, although total clearing of the cornea can be expected to require more than a week (Figure 6.8). Because the silver nitrate appears to sting, pretreatment with a topical anesthetic is advised. In human medicine, both 1% silver nitrate solution and
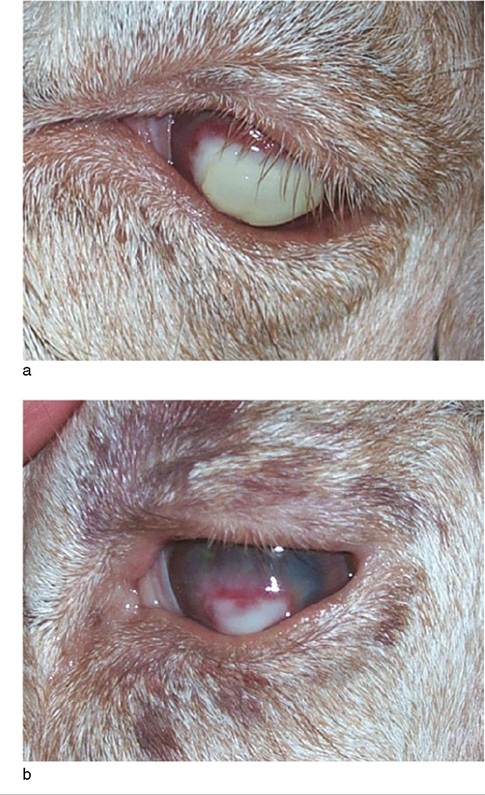
Figure 6.8 (a) A totally opaque and softened cornea from severe bilateral keratoconjunctivitis. (b) The same cornea, five days after initiation of treatment with systemic oxytetracycline and topical 5% silver nitrate. The cornea is firm, shiny, and clearing. Source: Courtesy of Dr. M.C. Smith.
2.5% povidone iodine solution have been effective in killing microorganisms in the eye for prophylaxis of ophthalmia neonatorum (Isenberg et al. 1994).
Non-infectious Keratitis
Not all cases of keratitis begin as infectious conjunctivitis.
Abrasions
Foreign bodies (in addition to eyelashes) may abrade or penetrate the cornea. The eye is painful, and fluorescein staining reveals a defect in the corneal epithelium. Treatment for shallow abrasions is with an antibiotic ointment after careful search for a foreign body in the fornix or behind the third eyelid, or, in the case of burdock (Arctium) pappus bristles, lodged in the conjunctiva of the eyelid. If the injury has reached the level of Descemet's membrane and the inner layer of the cornea bulges outward, a conjunctival or third eyelid flap is indicated. A corneal stromal ulcer with lysis (melting) as a result of collagenase production may appear soft and gelatinous or may resemble a deep abrasion. When any doubt exists as to the origin of the lesion, anticollagenase drugs such as acetylcysteine topically and a non-steroidal anti-inflammatory drug should accompany placement of a conjunctival flap. If the full thickness of the cornea has been perforated but iris has plugged the hole, consultation with or referral to an ophthalmologist is desirable. Typically, a collapsed eyeball (phthisis bulbi) is enucleated.
Exposure Secondary to Facial Nerve Deficit
Listeria organisms often enter the brain stem along a cranial nerve. If the facial nerve is thus involved, unilateral paresis or paralysis of the eyelids may occur before any signs of central nervous system disturbance are recognized. The goat that can no longer blink may incur a shallow abrasion to the cornea, which the owner recognizes because of lacrimation, conjunctival injection, corneal clouding, and photophobia. It is very important for the veterinarian to evaluate ipsilateral tone of eyelid, ear, and lip. Although it may be impossible to distinguish a facial nerve paralysis of traumatic origin or secondary to otitis media from early listeriosis, treatment with penicillin or tetracycline for one week is justified, because the prognosis for an animal with listeriosis is so much worse when the signs are unequivocal.
The cornea dries out and becomes opaque in more advanced listeriosis or other long-standing facial nerve paralysis. A temporary tarsorrhaphy, wherein partialthickness sutures are placed to hold the lids in apposition over the cornea, may be helpful in such cases. This procedure prevents additional corneal damage and decreases the frequency with which application of ointments is required during the prolonged recovery period, until nerve function returns. In general, local therapy for exposure keratitis should include antibiotics to prevent secondary infection and atropine for cycloplegia (Rebhun and de Lahunta 1982). Uveitis and even hypopyon can be expected in severely affected goats. For further discussion of listeriosis, see Chapter 5.
Vitamin A Deficiency
Bilateral corneal opacity, lacrimation, and diarrhea were observed in kids born in a goat herd experiencing severe vitamin A deficiency due to six months on dry pasture. All signs disappeared after improvement of the diet (Caldas 1961). Night blindness, lacrimation, and corneal ulceration were reported in adult goats kept on an experimental vitamin A-deficient diet for periods as long as two years (Schmidt 1941; Majumdar and Gupta 1960; Dutt and Majumdar 1969).
Toxins
Phenothiazine was once commonly used as an anthelmintic. If metabolism is not complete, phenothiazine sulfoxide reaches the aqueous humor and is a primary photosensitizing agent; it induces uveitis, corneal endothelial damage with subsequent edema, and keratitis (Enzie and Whitmore 1953). Young goats should be kept out of direct sunshine for three days after receiving this drug.
Keratoconjunctivitis sicca, or dry eye, is one of the signs associated with locoweed poisoning (Astragalus spp.). Drying out of the eyes may be caused by inadequate blinking and failure of neurologic stimulation to the lacrimal glands, or by reduced tear production capabilities of the glands.
The imported fire ant (Solenopsis invicta) is present in the south-central United States. Ants occasionally attack weak or debilitated animals, injecting a necrotoxic venom into the victim. Necrotic ulceration of conjunctiva and cornea has been observed in a goat stung by these ants (Joyce 1983).
Caprine Mucopolysaccharidosis-IIID
A recessive genetic defect (G6S) of Nubian goats that causes a deficiency of N-acetylglucosamine-6-sulfatase results in the accumulation of glycosaminoglycans in lysosomes. Growth retardation has been reported clinically. One severely affected kid was ataxic and developed mild, non-progressive corneal clouding; histologically there was vacuolation of cells in the cornea as well as in the brain (Jones et al. 1998). A survey of 552 purebred Nubian goats in Michigan revealed that 25% of the animals were heterozygous for the mutation and 1.3% were homozygous (Hoard et al. 1998).