Diagnosis
Brachycephalic conformation should increase suspicion for aspergillosis, although these cats are also over-represented for viral respiratory infections. Where epistaxis is present, neoplasia, mycotic rhinitis or severe chronic rhinosinusitis is more likely.
Other fungal, bacterial or neoplastic processes extending from the nasal cavity to the orbit can have a similar presentation to SOA. Haematological and serum biochemical changes are usually mild and non-specific. Mild peripheral eosinophilia is present occasionally, and mild to marked hyperglobulinaemia is relatively common in cats with SOA (Hamilton et al. 2000; Tomsa et al. 2003; Furrow and Groman 2009; McLellan et al. 2006; Smith and Hoffman 2010; Barachetti et al. 2009; Barrs et al. 2012; Giordano et al. 2010; Kano et al. 2013). Serological tests are used widely for non-invasive diagnosis of aspergillosis in humans and animals (Seyedmousavi et al. 2015). However, the diagnostic utility of serological tests to detect the fungal cell-wall antigen galactomannan (GM) or Aspergillus-specific antibodies is heavily influenced by host immunocompetence. A commercial ELISA to detect GM in serum (Platelia Aspergillus EIA, Bio-Rad) has a sensitivity of up to 90% in immunocompromised patients, including neutropenic human patients with pulmonary aspergillosis and dogs with DIA (Pfeiffer et al. 2006; Garcia et al. 2012). However, in non-neutropenic patients with pulmonary aspergillosis, assay sensitivity is less than 30% (Hachem et al. 2009; Kitasato et al. 2009; Pfeiffer et al. 2006). In dogs with SNA, a patient cohort that is systemically immunocompetent, GM also performs poorly (24% sensitivity) (Billen et al. 2009). In immunocompetent patients, GM is cleared by neutrophils, which possess mannose-binding receptors, or by antibody complexing (Mennink-Kersten et al. 2004; Herbrecht et al. 2002). Also, lack of tissue invasion in non-invasive mycoses such as SNA likely contributes to lack of detectable circulating GM. Interestingly, in cats with URTA, the sensitivity of GM detection is low in both non-invasive (SNA) and invasive (SOA) forms of disease with an overall sensitivity of only 23%. This result likely reflects the general systemic immunocompetence of affected cats (Whitney et al. 2013). Except in the setting of ruling out URTA in cats with respiratory disease (90% specificity), serum GM is not useful as a routine diagnostic test for feline URTA.Detection of Aspergillus-specific IgG by ELISA has high sensitivity in immunocompetent patients with aspergillosis, including dogs with SNA (88%) and humans with chronic pulmonary aspergillosis (90%). Specificity is also high (>90%), since optimal cut-off values can generally differentiate between exposure and infection (Billen et al. 2009; Page et al. 2015). Similar results were found using an indirect ELISA and a commercial antigen preparation derived from mycelial elements of A. fumigatus, A. flavus and A. niger to diagnose URTA in cats (sensitivity 95%, specificity 93%). Most cats in the study had infections with cryptic species (A. felis, A. thermomutatus, A. Ientulus or A. udagawae), demonstrating antibody crossreactivity with the antigen preparation (Barrs et al. 2015). A more recent study showed that a high proportion of cats with URTA also have detectable Aspergillus- specific IgA, but in the cohort studied, paired measurement of serum Aspergillus- specific IgA and IgG was of no benefit for diagnosis of URTA over IgG alone (Taylor et al. 2016). Human patients with chronic pulmonary aspergillosis that test negative for IgG may test positive of IgA, since Aspergillus-specific IgA can bind different fungal antigens than IgG (Page et al. 2015). Advanced imaging (computed tomography or magnetic resonance imaging) is recommended for all cases of suspected feline URTA and is the most useful test to differentiate SNA from SOA.
Orbital involvement may not be apparent at presentation in early disease, but its detection necessitates systemic antifungal therapy as part of the management plan. For cats with only sinonasal cavity involvement, assessment of cribriform plate integrity is required before treatment using intranasal azole preparations.Computed tomographic features of feline SNA are similar to canine SNA and include severe cavitated turbinate lysis (Fig. 15.5). Nasal cavity involvement is frequently bilateral and asymmetric, while frontal sinus involvement is usually unilateral. Other common findings in SNA include punctate areas of orbital bone lysis, which may be bilateral, and reactive bony change (sclerosis) of the nasal and frontal bones (Barrs et al. 2014). Cats with SOA have similar signs of sinonasal cavity involvement and sphenoid sinus involvement is frequent. Orbital masses cause dorsolateral displacement of the globe and extend laterally into paranasal maxillary soft tissues and ventrally into the pterygopalatine fossa of the oral cavity. Masses show heterogeneous contrast enhancement, including central coalescing hypoattenuating areas and peripheral rim enhancement (Fig. 15.5). Mass lesions within the nasal cavity, nasopharynx or paranasal sinuses are also more commonly observed in cryptic species infections than in infections caused by A. fumigatus, which typically cause cavitated turbinate lysis (Barrs and Talbot 2014). In SOA lysis and reactive change of the paranasal bones are also common. Changes seen in URTA are not pathognomonic for the disease and may be similar to other mycotic, chronic inflammatory or neoplastic diseases. MRI is the imaging modality of choice for patients with SOA presenting with neurological signs. On MRI, feline SOA orbital masses are T2-hyperintense.
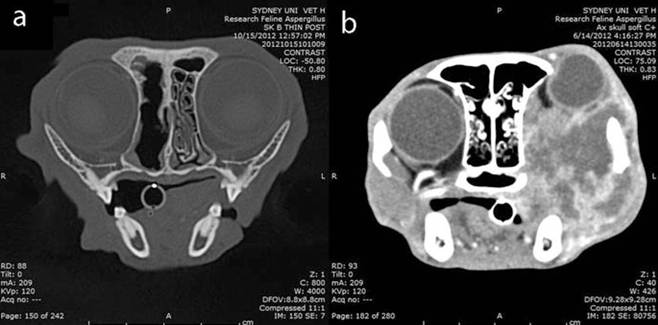
Fig. 15.5 (a) Transverse skull CT image of a cat with sinonasal aspergillosis due to A.
fumigatus infection. There is severe unilateral right-sided cavitated nasal turbinate lysis. (b) Transverse postcontrast soft-tissue images of the head in a cat with sino-orbital aspergillosis from infection with A. felis. A left orbital fungal granuloma has caused compression and dorsal displacement of the globe, with extension into the oral cavity, and adjacent maxillary soft tissues. The orbital mass shows heterogeneous contrast enhancement, with central coalescing hypoattenuating foci and peripheral rim enhancementEndoscopic assessment of the sinonasal cavity using rigid rhinoscopy and nasopharyngoscopy is indicated for both diagnosis of SNA and therapeutic debridement of sinonasal fungal plaques. Biopsy specimens can be obtained for fungal culture and cytological/histological identification of hyphae. Biopsy specimens should be stored frozen for PCR if URTA is suspected but fungal culture is negative. Sinuscopy is indicated for diagnosis when CT findings indicate sinus involvement and fungal plaques are not visualised on rhinoscopy. While anatomical landmarks have been defined for sinus trephination in cats (Winstanley 1974), CT findings can provide more precise information.
For cats with SOA, retrobulbar masses can be biopsied via the oral cavity where there is pterygopalatine invasion (Barrs et al. 2012). Nasal, nasopharyngeal and paranasal lesions can also be biopsied, as indicated by CT findings (Smith and Hoffman 2010).
The fungal pathogens that cause feline URTA can usually be isolated from tissue biopsies or sinonasal fungal plaques on commercial culture media such as Sabouraud's dextrose agar or malt extract agar. Twenty-two of 23 cases of feline URTA were culture positive in one study (Barrs et al. 2012). Cryptic species that cause URTA including A. felis, A. udagawae and A. Ientulus are usually unable to grow at 50 °C, in contrast to A. fumigatus s. str. These species also tend to have a slow-sporulating phenotype giving colonies a whitish appearance before sporulation in contrast to the grey-green rapidly sporulating colonies of A. fumigatus s. str.
Aspergillus viridinutans complex species have angled or “nodding” conidial heads. However, the prevalence of this morphological feature varies between species, and other non-related section Fumigati species including A. brevipes, A. unilateralis and A. duricaulis also share this feature (Novakova et al. 2014). Thus, molecular confirmation of species is essential for accurate identification of fungal isolates from cats with URTA, with the exception of A. fumigatus, where consistent morphological features and growth at 50 °C may be acceptable.
15.8