diagnosis of GASTRIC DISEASE
History and Physical Examination
Vomiting is the predominant and most consistent sign of the patient with gastric disease; however, the vomiting patient is a diagnostic and therapeutic challenge.
Many nongastric disorders cause vomiting (Boxes 5-1 and 5-2), and not all patients with gastric disease are observed to vomit. Vomiting does not always indicate presence of a serious problem, but it is often the first sign of many life-threatening diseases such as parvovirus, hemorrhagic gastroenteritis (HGE), pancreatitis, intussusception, hypoadrenocorticism, and acute renal failure. For these reasons, a detailed history and thorough physical examination are essential to determine if a serious problem exists and to formulate a logical and economical diagnostic plan.Clinical abnormalities in patients with primary gastric disease are usually nonspecific. Vomiting, hematemesis, melena, anorexia, abdominal pain, and distention are the predominant signs of gastric disease, whereas diarrhea and weight loss occur less frequently. Vomiting is considered to be the hallmark of gastric disease. Unfortunately, most owners do not distinguish between vomiting and regurgitation when describing the problem and will also confuse vomiting with dysphagia, gagging, or coughing. Most patients that are diagnosed with esophageal disease at the University of Tennessee Veterinary Teaching Hospital initially have vomiting instead of regurgitation as the pri-
mary owner complaint. To avoid misinterpretation of clinical signs, the owner must be questioned carefully to distinguish between what has been observed versus the owner’s interpretation of those observations. Characteristics helpful in differentiating among vomiting, regurgitation, and dysphagia are listed in Table 5-1.
Hematemesis and melena are commonly caused by gastric bleeding from erosive or ulcerative gastric disease (Box 5-3) but can also be caused by esophageal or small intestinal bleeding. Digested blood in the vomitus is typical of gastric bleeding, whereas fresh blood is more likely to be of oral or esophageal origin. Black stool can result from bleeding from any portion of the upper GI tract; however, gastric bleeding is the most common cause of melena. Coagulopathy should always be ruled out in any patient with hematemesis or melena.
Abdominal distention is a less common but important sign of gastric disease. Acute abdominal
distention accompanied by unproductive retching, particularly in larger-breed dogs, are cardinal signs of gastric dilatation-volvulus (GDV). In this instance distention is primarily caused by air in the stomach. Delayed gastric emptying, caused either by pyloric outflow obstruction or by abnormal gastric motility, is often characterized by postprandial distention from retention of fluid and ingesta in the stomach. Nongastric causes of abdominal distention occur more gradually and include ascites, peritonitis, organomegaly, tumor, Cushing's syndrome, and obesity.
Laboratory Evaluation
Laboratory tests help to distinguish primary GI causes of vomiting from metabolic causes and to assess patient status for complications. Complete
| Predisposing Causes of Gastric Erosive-Ulcerative Disease | |||
| Nonsteroidal Antiinflammatory Drugs | Altered Gastric Blood Flow—Stress-Related | ||
| Aspirin | Piroxicam | Factors | |
| Phenylbutazone | Naproxen | Hypotension | Surgery |
| Indomethacin | Ibuprofen | Shock | Spinal cord disease |
| Ketoprofen | Indoprofen | Sepsis | Gastric dilatation-volvulus |
| Meclofenamic acid | Flunixin meglumine | ||
| Increased Secretion of Gastric Acid | |||
| Corticosteroids | Gastrin-secreting tumor | ||
| High dose, long duration | Mast cell tumor | ||
| Associated with other risk factors | Pyloric outflow obstruction—chronic gastric distention | ||
| Metabolic Diseases | colspan=2 bgcolor=white>Toxic-Traumatic Agents | ||
| Liver failure | Renal failure | Bile salts | Foreign bodies |
| Hypoadrenocorticism | Acute pancreatitis | Pancreatic enzymes | Alcohol |
| Neurologic disease | Inflammatory bowel disease | Lead | Corrosive compounds |
| Gastric Neoplasia | |||
blood counts (CBCs) are often normal in patients with primary gastric disease; however, a CBC can provide clues to the cause of vomiting.
Chronic gastric bleeding can result in nonregenerative anemia, often with characteristics of iron deficiency (microcytosis, hypochromasia, thrombocytosis). Acute gastric hemorrhage can cause either a regenerative or nonregenerative anemia, depending on severity and duration of bleeding. Parvovirus usually causes profound neutropenia, whereas other enteric viruses cause no characteristic changes in the CBC. Acute pancreatitis, bacterial enterocolitis, and inflammatory bowel disease (IBD) can cause a neutrophilic leukocytosis. Eosinophilia in the vomiting patient can occur from parasitism, eosinophilic gastroenteritis, and adrenocortical insufficiency.Biochemical tests provide important diagnostic and therapeutic information in the vomiting patient. Normal biochemical test results eliminate most metabolic causes of vomiting. One exception is cortisol-dependent hypoadrenocorticism, in which electrolyte concentrations are normal despite the patient having clinical signs typical of Addison's disease. In this instance an adrenocorticotropic hormone (ACTH) stimulation test is needed to rule out hypoadrenocorticism as a cause of vomiting. Hypoproteinemia occurs infrequently as a result of chronic infiltrative or granulomatous disease such as gastric lymphoma, carcinoma, or infection with Pythium spp. Urinalysis is useful to rule out nongastrointestinal causes of vomiting such as renal failure and diabetic ketoacidosis.
Vomiting of short duration does not change fluid, electrolyte, or acid-base balance, whereas profuse or protracted vomiting can cause significant abnormalities. These changes, however, do not reliably indicate the cause of the problem. Dehydration is the most common problem caused by vomiting. Hypokalemia frequently occurs as a result of loss of potassium both in the vomitus and urine, coupled with lack of dietary intake. Hypochloremia occurs from loss of chloride-rich gastric secretions and from reduction of chloride reabsorption in the distal nephron that occurs when the patient is hypokalemic.
The acid-base status of the vomiting patient can be acidotic, alkalotic, or normal depending on the composition of the vomitus and the presence of dehydration, lactic acidosis, or metabolic disease such as renal insufficiency. Many vomiting patients have normal acid-base status because of simultaneous loss of gastric hydrochloric acid and bicarbonate-rich duodenal juice. Others will have metabolic acidosis caused by dehydration, prerenal azotemia, and lactic acidosis from decreased tissue perfusion. Hypochloremic metabolic alkalosis indicates that loss of a substantial amount of gastric contents has occurred and is most indicative of gastric outflow obstruction. Duodenal or biliary obstruction, acute pancreatitis, or renal failure can cause similar imbalances from loss of large quantities of gastric juice. If the vomiting patient is hyperkalemic, hypoadrenocorticism and oliguric or anuric renal failure are the most likely causes of the vomiting. Occasionally, severe intestinal disease caused by trichuriasis or by bacterial enterocolitis will mimic hypoadrenocorticism, causing a syndrome of vomiting and diarrhea and hyponatremia-hyperkalemia that is typical of hypoadrenocorticism.Imaging
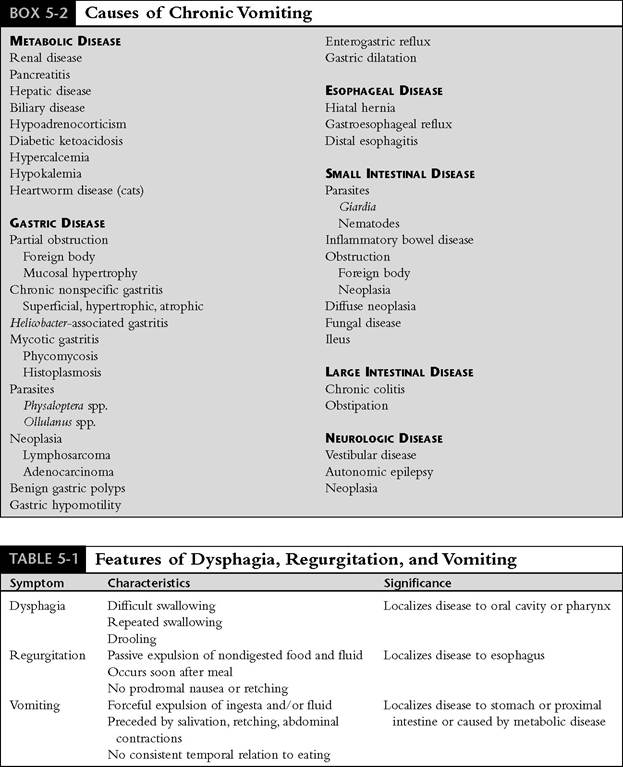
Survey and contrast radiographs are valuable when evaluating the patient with suspected gastric disease. Survey radiographs identify foreign bodies and gastric distention, displacement, or malposition. Gastric distention with gas is common in an excited or struggling patient due to aerophagia or in patients with dyspnea, but it can also occur with GDV. Simple aerophagia causes a large but normally positioned and nontympanic stomach. GDV causes a tense and malpositioned stomach in a patient with signs of retching and vomiting. The major radiographic feature of GDV is gas and fluid distention of the stomach, with displacement of the pylorus dorsally and to the left. Radiographic determination of the location of the pylorus is the essential differentiating feature between simple gastric dilation and GDV.
This is best accomplished by comparing left and right lateral recumbent views (Figure 5-2, A and B). A stomach distended with fluid or ingesta in a patient that has been fasted overnight is indicative of delayed gastric emptying. Gastric wall thickness, gastric ulcers, and gastric masses are very difficult to accurately identify using survey radiographs unless outlined by intraluminal air. Pneumoperitoneum indicates rupture of a vis- cus such as a penetrating gastric or intestinal ulcer, abdominal infection with gas-forming bacteria, or less commonly from perforation of the vagina or uterus.Contrast radiographs of the stomach and duodenum can be helpful when laboratory data and survey radiographs have not revealed the cause of vomiting. Gastric or intestinal foreign bodies,
Figure 5-2 Gastric dilatationvolvulus. A, Left lateral recumbent view of an 8-year-old German shepherd with gastric dilatation-volvulus. The stomach is very distended with gas in the fundus and the body. The pyloric portion is fluid filled and not well visualized. B, Right lateral recumbent view of the same dog. The stomach is distended with gas. A fold of soft tissue (arrows) separates the dorsally displaced, gas-filled tubular pylorus (P) from the dilated fundus of the stomach, key findings that confirm the presence of volvulus. The bowel is displaced caudally and ventrally, and the spleen is not identified because of gastric malposition. (Courtesy Dr. William Adams.)
masses, ulceration, or evidence of delayed gastric emptying can usually be identified. Filling the stomach with air to provide negative contrast can help to identify foreign bodies, gastric wall masses, or deep ulcers. Positive contrast gastrography using premixed barium sulfate is more reliable. Barium should be given by stomach tube to the fasted patient; recommended doses are 4 to 6 ml/lb for small dogs and cats and 2 to 4 ml/lb for large dogs.
Ventrodorsal, right lateral, and left lateral radiographs should be taken within 5 minutes of giving the barium and repeated in 20 to 30 minutes. Liquid barium should be observed in the duodenum within 5 to 20 minutes, and the stomach should be nearly empty within 3 hours. If barium does not enter the duodenum within 30 minutes, or if the stomach remains barium filled with no evidence of peristalsis, a gastric motility disorder or gastric outflow obstruction should be suspected (Figure 5-3, A). The presence of a persistently narrowed stream of barium at the pylorus is suggestive of pyloric obstruction from hypertrophy, neoplasia, or inflammatory disease (Figure 5-3, B and C). Atropine, aminopentamide, ketamine, and xylazine will significantly slow gastric emptying, giving the false impression of gastric outlet obstruction. If a tranquilizer is needed, acepromazine is recommended. (See Chapter 2 for details on GI contrast radiography.)Liquid barium contrast radiographs are most useful to detect gross abnormalities of the gastric mucosa. This technique, however, is an insensitive indicator of gastric emptying of a meal when a functional gastric motility disorder or partial obstruction in the stomach or bowel is suspected. This limitation, in addition to the difficulty encountered in administering barium by orogas- tric tube, the need for multiple radiographs to be taken at specific times, the risk of barium aspiration, and the inaccuracies in interpretation of results have led to the development of a new method to evaluate GI motility.
Barium-impregnated polyethylene spheres (BIPS)[§§] are commercially available radiopaque markers that are given orally to quantitatively measure the gastric emptying rate and intestinal transit time of food. Diagnostic sets of BIPS consist of multiple (30 1.5-mm spheres and 10 5.0-mm spheres) contained within gelatin capsules that dissolve in the stomach and release the spheres. The primary function of the large spheres is to detect GI tract obstruction, whereas the smaller spheres provide a quantitative measure of gastric emptying rate and intestinal transit time of food. The rate of gastric emptying is calculated by determining the percentage of markers that remain in the stomach after a standard period of time and comparing that percentage with reference ranges provided by the manufacturer. Various radiographic patterns showing selective movement or retention of small versus large spheres or patterns that show a bunching of spheres are also used to identify and localize specific problems such as partial obstruction. Use of these spheres is a practical diagnostic tool to evaluate gastric emptying of solids in dogs and cats. Patients with chronic vomiting, particularly those with chronic postprandial vomiting, recurrent bloating, or suspected radiolucent foreign body, or patients with anorexia of unknown cause are good candidates for a gastric motility study using BIPS.
Gastric emptying of solids can also be evaluated using fluoroscopy to observe movement of barium mixed with food into the doudenum. Nuclear scintigraphy is used to evaluate gastric emptying of liquids versus solids. These techniques are obviously limited in availability to referral institutions, whereas use of BIPS is practical for most veterinary practices. Ultrasonography has limited use in evaluating the stomach wall for abnormalities because of interference from air in the gastric lumen. Filling the stomach with water via gastric tube helps to eliminate this problem and improves sonographic visualization of the gastric wall. (See Chapter 2 for a discussion on GI ultrasonography.)
Endoscopy
Gastroduodenoscopy (Figure 5-4, A and B; see color plate) is the most useful method available for the diagnosis of gastric disease because it allows direct visualization and biopsy of the surface of the stomach and duodenum. Small lesions not detected by radiographs can usually be seen with an endoscope, foreign bodies can be removed, and biopsy specimens can be obtained. Because histologic lesions can be present in a normal-appearing stomach or duodenum, multiple biopsy specimens should always be obtained, even if the gross appearance is normal. If endoscopy is not available, exploratory surgery must be done to remove foreign bodies and to obtain biopsy specimens.
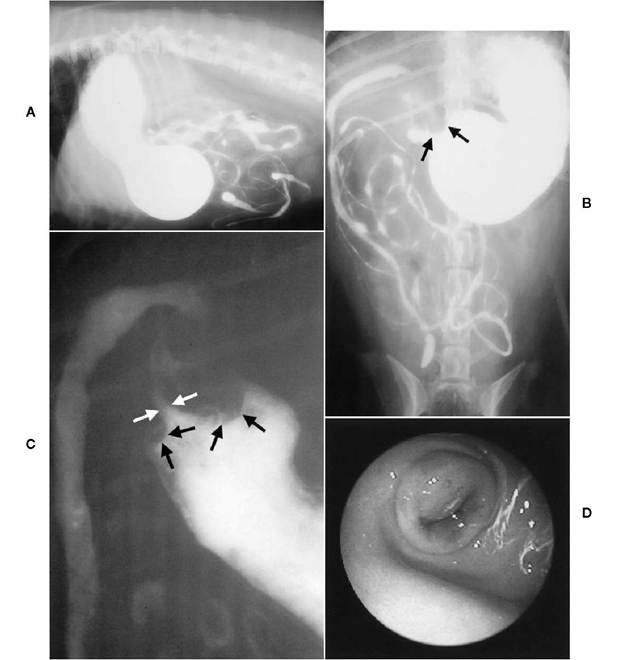
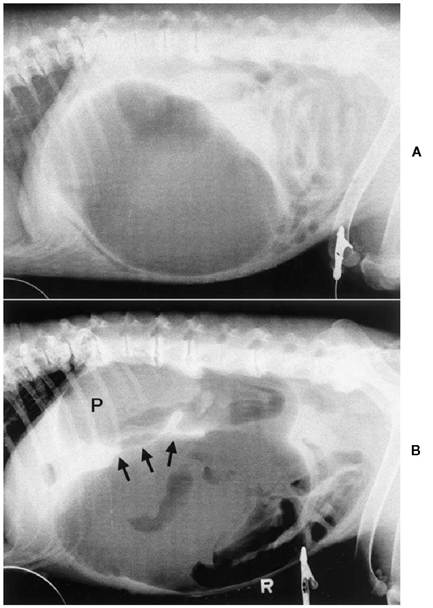
Figure 5-3 Delayed gastric emptying. A, Right lateral recumbent radiograph of a 5-year-old, 16-lb female/spayed (F/S) Chihuahua-mix with chronic intermittent vomiting caused by antral pyloric hypertrophy. The stomach is distended with liquid barium, most of which is retained in the stomach 5 hours after administration.
B, Ventrodorsal radiograph showing a narrowed pyloric antrum. Filling defects (arrows) caused by antral hypertrophy were consistent throughout the series of radiographs. C, Close-up ventrodorsal view of the pyloric region. Hemispheric filling defects (black arrows) protruding into the lumen cause an annular stricture of the pyloric sphincter. A faint narrow stream of barium (beak sign) (white arrows) can be seen passing through the partially obstructed pylorus into the duodenum. D, Endoscopic appearance of the pylorus showing circumferential thickening and bulging of a masslike lesion of the pylorus. The pylorus was rigid, and the endoscope could not be passed into the duodenum. Endoscopic biopsy revealed mild lymphocytic-plasmacytic gastritis and mucosal hyperplasia. A Y-U antral advancement flap pyloroplasty was done, and excisional biopsy confirmed the presence of hypertrophic gastropathy.
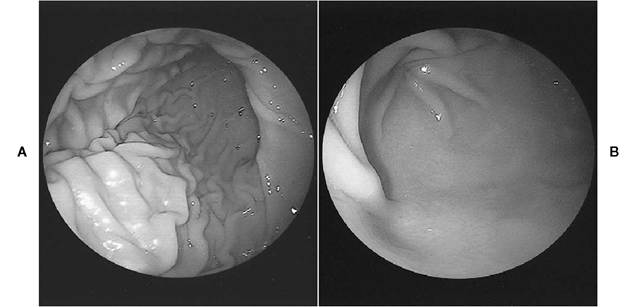
Figure 5-4 Normal stomach. A, Endoscopic appearance of a normal stomach. The smooth, pale-pink rugal folds of the greater curvature of the gastric body gradually become more linear distally at the junction with the pyloric antrum. The incisura angularis appears as a curved fold located at the 12 to 3 o’clock position. B, Appearance of a normal pyloric antrum (foreground) and pylorus (upper left). The antral mucosa is smooth, pale pink, and without rugal folds. The closed pyloric orifice is located at the center of the converging mucosal folds. (See color plate.)
BOX 5-4
Causes of Acute Gastritis
Dietary
Spoiled foods
Food sensitivity
Foreign body
Infectious
Viral
Parvovirus
Distemper
Infectious hepatitis
Coronavirus
Bacterial
Helicobacter spp.[***]
Parasitic
Physaloptera spp.*
Ollulanus spp.*
Drugs
Nonsteroidal antiinflammatory drugs (NSAIDs)*
Corticoste ro ids*
Chemicals/Toxins
Cleaning products
Ethylene glycol
Herbicides
Fertilizers
Petroleum distillates
Organophosphates
Heavy metals
Plant toxins