ACUTE GASTRITIS AND GASTRIC EROSIVE-ULCERATIVE DISEASE
Causes
Acute gastritis occurs commonly in dogs and cats and is caused by numerous factors that result in gastric mucosal injury and inflammation. Dietary indiscretion, food intolerance, or allergy; ingestion of foreign material, chemicals, and plant irritants; viral and parasitic infections; and drugs are causes of acute gastritis (Box 5-4).
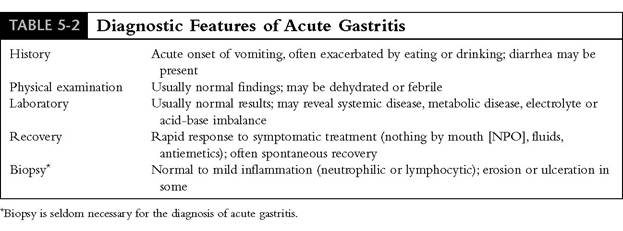
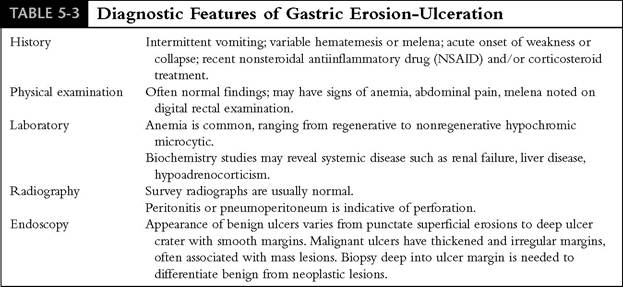
Many patients, however, respond to symptomatic treatment, and a definitive cause of the acute gastritis is not identified. Repeated exposure to dietary antigens, drugs, chemicals, toxins, or infectious agents is thought to initiate an allergic or immune-mediated response, ultimately causing chronic gastritis. Diagnostic features of acute nonspecific gastritis and gastric ulceration are listed in Tables 5-2 and 5-3, respectively.There are many causes of gastric erosion-ulcer (GEU) (see Box 5-3), and the signs can be acute or chronic. Nonsteroidal antiinflammatory drugs (NSAIDs) continue to be one of the most common causes of GEU, particularly in dogs. Mucosal damage caused by NSAIDs is primarily the consequence of two effects: NSAIDs cause direct damage to the gastric mucosa, and more importantly
NSAIDs inhibit synthesis of gastroprotective prostaglandins. All commonly used NSAIDs,espe- cially ibuprofen, piroxicam, and flunixin, have the potential to cause GEU. Ibuprofen, which owners frequently give to their pets thinking it is safe, is particularly dangerous because it undergoes enterohepatic circulation, which significantly prolongs the half-life of the drug compared with humans; the same is true for piroxicam. Flunixin has strong antiprostaglandin potency and is often used in combination with corticosteroids and/or in conditions where there is hypoperfusion of the GI tract such as occurs with parvoviral enteritis and HGE and in the postoperative patient.
Such patients are predisposed to GEU because of the effects of mucosal hypoperfusion, and the use of flunixin or corticosteroids compounds the risk of severe gastric ulceration and possible perforation. Most dogs treated with combinations of NSAIDs and corticosteroids develop endoscopically visible gastroduodenal hemorrhages, erosions, or ulcers (Figures 5-5 and 5-6; see color plate). Because these lesions are often clinically silent, the potential for severe and sometimes fatal GI hemorrhage or perforation is frequently overlooked. Even the selective cyclooxygenase-2 (COX-2) inhibitors have been associated with GEU in dogs, although much less frequently than with the nonselective NSAIDs.Corticosteroids are another important category of drugs that increase the r isk of GEU. Corticosteroids decrease mucosal cell growth and mucus production and increase gastric acid secretion. Use of corticosteroids alone is not usually ulcerogenic; however, corticosteroids do enhance the damaging effects of NSAIDs, hypotension, refluxed bile acids, and other factors of mucosal damage. Prednisolone is usu-

Figure 5-5 NSAID-induced ulcerative gastritis. Diffuse ulcerative gastritis in a 9-year-old German shepherd-mix with degenerative joint disease. The dog was being treated with aspirin (325 mg 2 times a day). Treatment began 2 months before presentation, but clinical signs of weakness, vomiting, melena caused by acute gastrointestinal blood loss, and anemia did not occur until the day of presentation. (See color plate.)
ally not a problem unless used in very high dosages (e.g., greater than 2 mg/lb/day) for more than a few days. There is no doubt, however, that high dosages of dexamethasone can cause significant GEU, especially if other factors of mucosal damage are present.
Many metabolic diseases predispose to GEU, especially chronic liver disease, renal disease, and hypoadrenocorticism.
Liver insufficiency results in decreased gastric mucus production, decreased gastric epithelial cell renewal, and decreased gastric blood flow. These factors, coupled with an increase in serum bile acid concentration that stimulates gastrin and gastric acid secretion, can cause significant GEU. Injury to gastric epithelial cells and submucosal vessels by uremic toxins and by decreased renal metabolism of gastrin account for GEU that occurs in acute and chronic renal failure. Adrenocortical insufficiency, in which mucosal damage is likely caused by hypotension and loss of vascular tone, is an infrequent cause of GEU. Although most dogs with hypoadrenocorticism do not have signs of GEU, this disorder should be considered in dogs that have hematemesis or melena if drug therapy and liver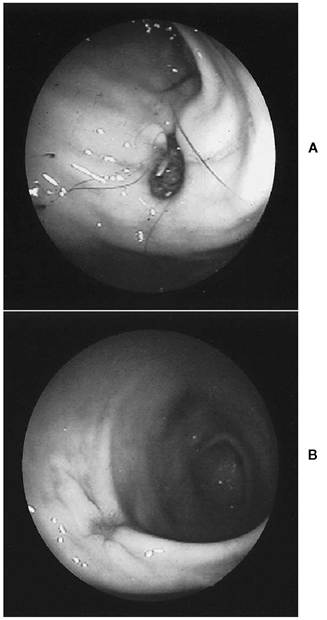
Figure 5-6 NSAID-induced gastric ulcer.
A, Gastric ulcer in pyloric antrum of a 5-year-old Welsh corgi that had been treated for back pain with ibuprofen (325 mg every day for 5 days). The dog had an acute onset of vomiting and an episode of melena on the day of presentation. B, Healing gastric ulcer in the same patient after 7 days of treatment with omeprazole (0.3 mg/lb every day). (See color plate.)
or renal disease have been eliminated as causes of the clinical signs.
Hypotension from shock, sepsis, hypovolemia, spinal trauma, and surgery are common but frequently unrecognized causes of GEU. The fundus and body of the stomach are very dependent on a rich submucosal blood supply to maintain mucosal barrier function. Reduced blood flow to the gastric mucosa impairs epithelial cell renewal. Endogenous vasoconstrictive catecholamines and corticosteroids that are secreted in response to hypotension further potentiate ulcer formation, as will the administration of exogenous corticosteroids. All critically ill patients, especially those with severe trauma, major surgery, organ failure, or sepsis, should be considered likely candidates for development of ulcers.
Mast cell tumors (MCT), pancreatic gastrinsecreting tumors (gastrinomas), and pancreatic polypeptide-secreting tumors can cause severe gastritis and significant GEU. MCTs, even those benign-looking subcutaneous lumps that at first glance appear to be nothing more than a lipoma, can release excessive amounts of histamine that stimulate hypersecretion of gastric acid, which subsequently damages the gastric and duodenal mucosa. Most dogs with MCT do not have clinical signs of GEU at the time of diagnosis. However, surgical manipulation or aggressive palpation can cause massive mast cell degranulation and release of histamine. Corticosteroids, which are sometimes used to treat MCT, can further predispose to GEU and occasionally cause gastric perforation.
Gastrinomas are small pancreatic tumors that secrete large amounts of gastrin, a trophic hormone that stimulates growth of gastric mucosa and secretion of excessive gastric acid. Severe gastroesophageal reflux, esophagitis, esophageal ulceration, chronic gastritis, duodenitis, and proximal duodenal ulceration will typically occur. Gastrinoma should be considered in any adult dog that has chronic vomiting, weight loss, diarrhea, melena, and/or signs of esophagitis. Increased fasting concentration of serum gastrin is diagnostic. Other causes of increased gastrin concentration that must be considered when interpreting serum gastrin results include renal failure and conditions that cause chronic gastric distention. In addition, treatment with proton pump inhibitors (e.g., omeprazole, lansoprazole) that have potent acidsuppressing effects will cause increased gastrin production because of the lack of negative feedback of acid on gastrin-secreting cells in the pyloric antrum. Treatment for gastrinoma requires tumor removal (partial pancreatectomy), which can be curative if no metastasis has occurred. Medical management requires use of the proton pump inhibitors such as omeprazole to maximally suppress acid secretion and control symptoms.
Therapy is indefinite. Patients with metastatic disease and those not controlled with acid-suppressing drugs alone can be treated with octreotide (Sandostatin), an antisecretory drug that inhibits gastrin secretion.Medical Management
Treatment of acute gastritis, erosions, and ulceration requires elimination of predisposing causes and symptomatic-supportive therapy to enhance mucosal defenses (Box 5-5). In general, fluids are given to prevent dehydration and to maintain mucosal perfusion. Oral intake should be stopped until vomiting resolves. Parenteral or enteral nutrition should be given to patients in poor nutritional condition (see Chapter 12), and blood transfusion is given to patients with severe anemia and evidence of ongoing GI bleeding. Surgical treatment is indicated when uncontrolled hemorrhage or perforation is suspected.
Drugs used for nonspecific medical management of gastritis and GEU include H2-receptor antagonists, proton pump inhibitors, cytopro- tective agents, and prostaglandin analogues (Table 5-4) and antiemetics (Table 5-5). The drugs listed in Table 5-4 were developed primarily for the treatment of gastric ulcer disease. However, they are very useful to treat a broad variety of disorders, including esophagitis, gastritis, and GI bleeding, as well as GEU. Suppression of gastric acid promotes healing of damaged mucosa and diminishes the proteolytic effects of gastric pepsin, which is most active in an acid environment. Cytoprotectants and prostaglandin analogues strengthen mucosal defenses. Promotility drugs reduce gastroesophageal and enterogastric reflux and help to control vomiting. Antiemetic therapies are designed to diminish either the humoral or neural pathways of the vomiting and are recommended for short-term use to provide patient comfort and to reduce fluid and electrolyte losses.
Antisecretory Drugs. Histamine, gastrin, and acetylcholine stimulate the gastric parietal cell to secrete acid; simultaneous stimulation by all three causes maximal acid secretion.
H2-receptor antagonists competitively and reversibly bind to H2- receptors on acid-producing gastric parietal cells to block the acid-stimulating effects of histamine and to render the cell less responsive to stimulation by acetylcholine and gastrin. Because these drugs are competitive inhibitors, they suppress but do not eliminate gastric secretion. The H2-receptor antagonists cimetidine, ranitidine, nizatidine, and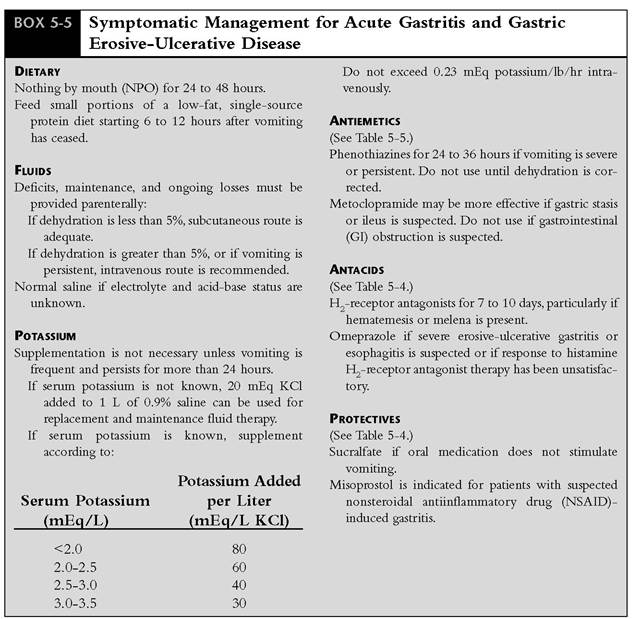
famotidine are useful to treat gastritis and GEU in dogs and cats. All are effective and differ primarily in acid-suppressing potency, frequency of dosing, and in prokinetic effects. Cimetidine is the least potent and must be given three to four times daily to achieve adequate acid suppression. Ranitidine and nizatidine both have about 5 times the potency of cimetidine. Ranitidine must be given twice daily, whereas nizatidine needs to be given only once daily. Famotidine is the most potent H2-receptor antagonist, being approximately 20 times more potent that cimetidine, and requires only once-daily dosing.
In addition to blocking acid secretion, ranitidine and nizatidine have a prokinetic effect on the GI tract. Both drugs increase acetylcholine, the primary stimulatory neurotransmitter of GI smooth muscle, by inhibiting acetylcholinesterase. The effects are to promote gastric emptying, which is helpful in controlling vomiting for patients with gastritis, and to decrease gastroesophageal and enterogastric reflux. Because of the dual prokinetic and acid suppression effects of ranitidine, this drug is a good first-choice H2-receptor antagonist. The reported incidence of side effects from H2-receptor antagonists is low, and use of these drugs is safe in both dogs and cats. Cimetidine can cause vomiting, diarrhea, and depression in dogs and cats. Because cimetidine and ranitidine inhibit the same hepatic enzymes that metabolize drugs such as theophylline and warfarin, these drugs should not be given concurrently.
Proton Pump Inhibitors
Benzimidazole drugs such as omeprazole and lansoprazole block the hydrogen-potassium adenosinetriphosphatase (ATPase) enzyme of the gastric
| TABLE 5-4 | H Drugs Used | in the Treatment of Gastritis and Gastrointestinal Ulcer Disease | ||||
| Generic Name | Mechanism | Product (Mfr) | Suggested Dosage | How Supplied | Side Effects | |
| H2 Receptor | Decrease acid | |||||
| Antagonists | secretion | |||||
| Cimetidine | Tagamet | 2.5-5.0 mg/lb q6h PO, IV, IM | Tablet | 200 mg | Inhibition of hepatic | |
| (GlaxoSmithKline) | 300 mg | microsomal enzymes; may | ||||
| 400 mg | cause drug interactions; | |||||
| 800 mg | mental depression | |||||
| Liquid | 60 mg∕ ml | |||||
| Injection | 150 mg∕ml | |||||
| Ranitidine | Zantac | 1.0 mg/lb q8-12h PO, IV, IM, SQ | Tablet | 150 mg | Similar to cimetidine, but to | |
| (GlaxoSmithKline) | 300 mg | lesser extent | ||||
| Liquid | 15 mg/ml | |||||
| Injection | 25 mg/ml | |||||
| Nizatidine | Axid (Lilly) | 2.5 mg/lb qd PO | Capsule | 150 mg 300 mg | None reported | |
| Famotidine | Pepcid (Merck) | 0.25 mg/lb qd PO, IV | Tablet | 10 mg | Similar to ranitidine | |
| 20 mg | ||||||
| 40 mg | ||||||
| Liquid | 8 mg/ml | |||||
| Injection | 10 mg/ml | |||||
| Proton Pump | Blocks acid | |||||
| Inhibitor | secretion | |||||
| Omeprazole | Prilosec (AstraZeneca) | 20 mg qd PO (>45 lb) | Capsule | 10 mg | Prolonged use can cause | |
| 10 mg PO (11-45 lb) | 20 mg | reversible gastric mucosal | ||||
| 5 mg PO ( | ||||||
| Sucralfate | Carafate (Hoechst | 1 g/15 Ib q6-8h PO | Tablet 1 g | Constipation | ||
| Marion Roussel) | ||||||
| Prostaglandin | Cytoprotective: Increases mucus and bicarbonate secretion | |||||
| Analogue | ||||||
| Enhances mucosal blood | ||||||
| flow | ||||||
| Decreases acid secretion | ||||||
| Misoprostol | Cytotec (Searle) | 1-2.5 μg∕lb q8h PO | Tablet 100 μg | Diarrhea | ||
| zoo μg | Abdominal cramps Vomiting Abortion | |||||
| Prokinetic Drugs Metoclopramide | Enhances gastric emptying; | Reglan (Robins) | 0.15-0.25 mg/lb q8h PO, SQ | Tablet 5 mg | Hyperactivity, constipation | |
| antiemetic | 0.5-1 mg/lb q24h IV | 10 mg | ||||
| Liquid 1 mg∕ ml Injection 5 mg/ml | ||||||
| Erythromycin | Accelerates gastric emptying | Erythromycin | 0.25-0.5 mg/lb q8h PO | |||
| of solids | ||||||
| H2-receptor | Enhances gastric emptying | Zantac | 0.25-0.5 mg/lb q8h PO | |||
| antagonist | and duodenal motility | (Glaxo SmithKline) Axid (Lilly) | ||||
PO, Orally; IV, intravenously; IM, intramuscularly; SQ, subcutaneously
Diseases of the
| UABjEm Antiemetic Drugs and Dosages | |||
| Druq | Primary Site of Action | Dosage | Side Effects |
| Prochlorperazine (Compazine, | CRTZ Vomiting center | 0.25 mg/lb q8h SQ, IM | Hypotension Sedation |
| GlaxoSmithKline) | |||
| Chlorpromazine (Thorazine, | CRTZ Vomiting center | 0.15-0.25 mg/lb q8h SQ | Hypotension Sedation |
| GlaxoSmithKline) | |||
| Yohimbine | CRTZ | 0.15-0.25 mg/lb q12h | Hypotension |
| (Yobine, Lloyd Labs) | Vomiting center | SQ, IM | Sedation |
| Diphenhydramine | CRTZ | 1-2 mg/lb q8h PO, IM | Sedation |
| (Benadryl, Parke-Davis) | |||
| Dimenhydrinate | CRTZ | 2-4 mg/lb q8h PO | Sedation |
| (Dramamine, Searle) | |||
| Haloperidol | CRTZ | 0.01 mg/lb q12h | Sedation |
| (Haldol, Ortho-McNeil) | |||
| Meto clopramide (Reglan, Robins) | CRTZ GI smooth muscle (facilitates gastric emptying) | 0.15-0.2 mg/lb q6h PO, SQ, IM 0.5-1 mg/lb/day as continuous IV infusion | Extrapyramidal signs |
| Domperidone (Mo tilium, J ansse n) | GI smooth muscle cells (facilitates gastric emptying) | 0.05-0.15 mg/lb q12h IM, IV | None reported |
| Cisapride (Propulsid, Janssen) | GI smooth muscle Myenteric neurons (facilitates gastric emptying) | 0.05-0.25 mg/lb q8h PO | None reported |
| Scopolamine (Hyoscine, Fujisawa) | Vestibular system CRTZ | 0.02 mg/lb q6h SQ, IM | Ileus Xerostomia Sedation |
| Ondansetron | CRTZ | 0.05-0.15 mg/lb slow IV | Sedation |
| (Zofran, GlaxoSmithKline) | Blocks vagal afferent neurons | q8-24h or 30 minutes before chemotherapy PO | Head shaking |
CRTZ, Chemoreceptor trigger zone; SQ, subcutaneously; IM, intramuscularly; PO, orally; IV, intravenously.
parietal cell to profoundly and irreversibly inhibit gastric acid secretion. Because these drugs block the final step of hydrogen ion secretion, they prevent secretion of gastric acid stimulated by histamine, acetylcholine, and gastrin. These drugs noncompetitively block the proton pump and therefore are much more potent than the H2-receptor antagonists. Proton pump inhibitors accumulate in the parietal cell and increase with each dose until acid secretion is almost totally inhibited after the fifth dose. Because of this delay in gastric acid suppression, H2-receptor antagonists should be used concurrently with proton pump inhibitors for the first 3 to 4 days of treatment in patients where rapid acid suppression is needed.
Proton pump inhibitors are recommended for the treatment of severe esophagitis and GEU that has not responded to therapy with H2-receptor antagonists and sucralfate. They are recommended as the drugs of choice for treatment of patients with hypersecretion of gastric acid that occurs with MCT and gastrinoma. Omeprazole and lansoprazole are similar in potency, are given once daily, cause no clinical, hematologic, or biochemical abnormalities, and are safe to use in cats and dogs.
Sucralfate
Sucralfate is a sulfated disaccharide—aluminum hydroxide complex that accelerates gastric mucosal healing by adhering to mucosal erosions and ulcers to provide a barrier to acid penetration. Sucralfate inactivates pepsin and adsorbs gastric-damaging bile acids refluxed from the duodenum. Sucralfate also stimulates endogenous prostaglandin synthesis in the gastric mucosa, resulting in increased secretion of mucus and bicarbonate and accelerated ulcer healing. Sucralfate is effective at acidic to near neutral pH and can therefore be used concurrently with antisecretory drugs such as H2-receptor antagonists or proton pump inhibitors. However, because sucralfate can adsorb other orally administered drugs, it should not be given within 2 hours of other oral drugs. Sucralfate is recommended for the treatment of esophagitis, gastritis, and gastric ulcer of any cause in dogs and cats. Its safety is well established, with constipation being the only reported side effect.
Synthetic Prostaglandins
Synthetic prostaglandin analogues such as misoprostol have been developed that impart protection to gastric mucosa in a manner similar to endogenous prostaglandins. Misoprostol stimulates gastric mucus secretion, increases bicarbonate secretion, increases gastric mucosal blood flow, and inhibits gastric acid secretion. Because most NSAIDs inhibit the production of endogenous prostaglandins, treatment with misoprostol helps to prevent gastric ulceration in patients in which chronic NSAIDs are used to control inflammation and pain from degenerative joint disease. Clinical studies of human and canine arthritic patients have shown misoprostol to be effective in preventing NSAID- induced gastric hemorrhage, erosion, or ulceration. Diarrhea, vomiting, and transient abdominal discomfort are potential side effects, particularly if used above the recommended dosage range of 1 to 1.5 μg∕lb every 12 hours. No adverse hematologic or biochemical effects have been reported with the use of misoprostol in dogs; similar information in cats is lacking. Misoprostol will cause abortions and should not be used in pregnant patients.
Prokinetic Drugs
Prokinetic drugs have no direct healing effect on gastric erosion or ulcer. However, these drugs improve gastric emptying and decrease enterogastric reflux, thereby helping to prevent damage to the gastric mucosa from refluxed bile acids and pancreatic enzymes. Metoclopramide is especially effective because it has both central antiemetic and peripheral gastric prokinetic effects. The antiemetic effect is mediated through antagonism of dopaminergic D2 receptors in the chemoreceptor trigger zone (CRTZ) of the medulla to inhibit vomiting induced by drugs, toxins, metabolic disease, and acid-base imbalances. Because serotonin receptors predominate in the CRTZ of the cat, metoclopramide does not appear to be as effective as a centrally acting antiemetic in the cat as in the dog. The prokinetic effect of metoclopramide is mediated through stimulation of serotonergic 5-HT4 receptors on GI smooth muscle to improve coordination of antral, pyloric, and duodenal contractions. The primary prokinetic effects are to accelerate gastric emptying of liquids and to decrease duodenogastric reflux, whereas gastric emptying time of solids does not appear to be shortened.
Metoclopramide is more effective as a centrally acting antiemetic than it is as a prokinetic drug. It is best used to control vomiting caused by nonspecific gastritis, uremia, and chemotherapy. The peripheral effects of metoclopramide to prevent gastric stasis and duodenogastric reflux, and to inhibit retrograde peristalsis that precedes vomiting, further help to diminish the severity of vomiting. Metoclopramide is administered parenterally to the vomiting patient at 0.1 to 0.25 mg/lb body weight every 8 hours. Constant intravenous infusion of 0.5 to 1.0 mg/lb body weight per 24 hours is usually more effective to initially control vomiting, particularly in patients with severe vomiting. Metoclopramide should not be used if gastric outlet obstruction or GI perforation is suspected or if the patient has a seizure disorder. Some patients are very sensitive to the effects of this drug and will actually have increased vomiting, presumably caused by excessive gastric contractions. Central effects of metoclopramide can also cause behavioral changes in some patients, ranging from lethargy in some to hyperactivity and agitated behavior in others. These effects can occur at recommended dosages and occur most frequently in cats. Pacing, vocalization, aggressive or agitated behavior, chewing at an intravenous catheter, and excessive panting are signs that should alert the clinician to sensitivity to or overdosage of metoclopramide. Side effects usually resolve when the drug is discontinued. However, if central nervous system (CNS) signs are severe, treatment with diphenhydramine (Benadryl) at 1 to 2 mg/lb intravenously will effectively reverse the side effects without altering promotility effects of the drug. Because metoclopramide is excreted by the kidneys, the dosage should be reduced by 50% in patients with renal failure.
Cisapride is a serotonergic agonist that binds to 5-HT4 receptors on enteric postganglionic cholinergic neurons to increase release of ' acetylcholine and stimulate GI smooth muscle contraction. Unfortunately, cisapride has been taken off the market in the United States because of an association with fatal arrhythmias in humans. No reports of similar complications occurring in the dog or cat exist. The future availability of this drug for veterinary use is uncertain, which is unfortunate because cisapride does have distinct advantages compared with metoclopramide. However, it is currently readily available through compounding pharmacies. Cisapride does not cross the blood-brain barrier; therefore it does not have the central antiemetic properties or CNS side effects of metoclopramide. Consequently, animals that experience metoclopramide-associated CNS side effects can be switched to cisapride without concern that the same side effects will occur. Cisapride accelerates gastric emptying by stimulating both pyloric and duodenal motor activity, by enhancing antropyloroduodenal coordination, and by increasing the propagation distance of duodenal contractions. As a result, this drug is much more effective than metoclopramide in enhancing gastric emptying, particularly that of solids. In addition, cisapride stimulates smooth muscle contraction throughout the GI tract, from the distal esophagus to the colon. In species such as the cat that have a smooth muscle component to the distal esophagus, distal esophageal contraction and gastroesophageal sphincter tone are enhanced. The effect of stimulating motility in the small intestine and colon has made this drug especially useful for the treatment of constipation and megacolon.
Erythromycin is a macrolide antibiotic that also generates prokinetic effects on the GI tract by stimulation of motilin receptors in GI smooth muscle. The primary effect is to stimulate gastric antral contractions similar to those that occur during phase III of the migrating myoelectric complex (MMC). Normally phase III contractions occur during the interdigestive phase rather than in the fed phase and act primarily to empty the stomach of larger indigestible solids. As a result, erythromycin accelerates gastric emptying of solids. Because of this action, it should be given during the fasted state and not until several hours after a meal has been eaten. The prokinetic dose for erythromycin (0.25 to 0.5 mg/lb orally every 8 hours for dogs and cats) is much lower than the antimicrobial dose, so side effects such as vomiting are uncommon.
Summary
In general, H2-receptor antagonists and/or sucralfate are effective first-choice drugs in treating gastritis, erosions, and ulcers. Although the effectiveness of these drugs in preventing GEU in the dog and cat is not known, treatment with these drugs should be considered for patients with disorders such as immune hemolytic anemia or immune thrombocytopenia that require treatment with high-dose and/or potent corticosteroids. Omeprazole should be considered for those patients not responding to first-line treatment and for those patients with hypersecretory disorders such as gastrinoma. Misoprostol is indicated for patients that require chronic NSAID treatment and possibly for the critically ill patient where endogenous prostaglandin production might be impaired. The duration of treatment with these drugs varies depending on the underlying cause. In most patients, treatment with antiulcer medications for 2 to 3 weeks is adequate, providing that predisposing causes of GEU have been eliminated.
Chronic Gastritis
Chronic gastritis appears to occur frequently in the dog and cat; however, the true prevalence is unknown. More frequent use of endoscopy has led to a significant increase in the diagnosis of chronic gastritis, the causes of which include food allergy, chronic NSAID therapy, and bacterial, parasitic, or fungal infection. Infection with gastric spiral bacteria (Helicobacter spp.) in particular appears to be a common cause of chronic gastritis in dogs and cats. In general the causes of chronic gastritis are similar to those of acute gastritis. In many instances, gastric inflammation is confirmed with biopsy; however, a specific cause cannot be identified. In this circumstance the histologic findings, although nonspecific, might point to an etiologic diagnosis and assist in making therapeutic and prognostic decisions (Table 5-6).
Chronic gastritis is characterized clinically by intermittent episodes of vomiting, sometimes with acute episodes, that have not responded to symptomatic treatment. Other signs are nonspecific and include inappetence, anorexia, weight loss, and abdominal pain. Hematemesis and melena occur if GEU or neoplasia is present. Diarrhea is uncommon unless the patient has inflammatory bowel disease. Diagnosis is based on laboratory tests to exclude metabolic causes of chronic vomiting, radiography, sonography, and endoscopic or surgi-
| EABLeB3 Histologic Classification of Chronic Gastritis | |
| Predominant Histologic Type* | Possible Causes to Consider |
| Eosinophilic | Immune response to dietary antigens, parasites, foreign material Idiopathic eosinophilic gastroenteritis Mast cell tumor Pythiosis |
| Granulomatous | Chronic infections Histoplasmosis Phycomycosis Mycobacteria Parasitic Immune response to foreign material Neoplasia Chronic nonsteroidal antiinflammatory drug (NSAID) therapy |
| Lymphocytic-plasmacytic | Helicobacter (lymphoid nodules in some) Immune response to dietary antigens Idiopathic lymphocytic-plasmacytic gastroenteritis Lymphosarcoma |
*Many gastric diseases cause mixed inflammatory cell reaction.
cal biopsy. Laboratory abnormalities that might occur are nonspecific and include anemia, leukocytosis, eosinophilia, and hypoproteinemia. Survey radiographs help to identify gastric foreign bodies but seldom identify primary gastric lesions. Contrast radiographs may show a thickened gastric wall, mucosal ulceration, mass lesions, or evidence of delayed gastric emptying.
Specific Causes of Chronic Gastritis
Helicobacter-associated Gastritis
Spiral bacteria of the genus Helicobacter infect the stomachs of many mammalian hosts, including humans, dogs, and cats. These gram-negative spiral organisms characteristically produce urease, an enzyme that helps these organisms to adapt to the gastric environment and can be used diagnostically to confirm infection. In humans, infection with Helicobacter pylori has been shown to be the primary cause of chronic gastritis and of gastric and duodenal ulcer disease and has been identified as a predisposing cause of gastric carcinoma and mucosal lymphoma. Several species of Helicobacter are commonly found in the stomachs of dogs and cats, and although the entire clinical significance of Helicobacter infection in these species is not known, evidence indicates that infection is a cause of chronic gastritis in dogs and cats.
Helicobacter heilmannii, Helicobacterfelis, Helicobacter bizzozeronii, and Helicobacter salomonis are the most common types found in dogs, having been identified in clinically normal dogs, as well as in dogs with clinical signs of chronic gastritis and with histologic findings of gastritis. H. felis, H. heilmannii, and H. pylori are the most common types found in cats. The reported prevalence of gastric Helicobacter infection is high in clinically normal dogs and cats, as well as in dogs and cats with signs of gastritis. In our hospital approximately 50% of dogs and cats that have had gastroscopy to determine the cause of chronic vomiting are infected with Helicobacter.
Despite the high incidence of infection, most dogs and cats infected with Helicobacter are not symptomatic for gastritis. However, some infected animals are symptomatic, a situation similar to that observed in humans. These observations pose the obvious question, Does infection cause disease? Most evidence indicates that certain Helicobacter spp. do cause disease, although the incidence of disease is much lower than the incidence of infection. A few anecdotal reports exist that describe resolution of Helicobacter- associated clinical gastritis following treatment with various combinations of antimicrobial-antacid therapy. These reports are limited by having small numbers of patients, by lack of biopsy-confirmed resolution of gastritis, and by lack of clinical controls. Perhaps the most compelling evidence of cause and effect is in a study of 100 animals (62 dogs and 38 cats) with clinical signs of gastritis. Helicobacter spp. were found in 63 animals (43 dogs and 20 cats), 62 of which had histologically confirmed gastritis. Treatment of infected animals with antibiotics plus antacids was associated with resolution of clinical signs in more than 90% of the affected animals. Of 19 animals in which biopsy was performed after treatment, 14 were negative for organisms and histologic gastritis had resolved in all. Other studies of experimental infection in dogs and cats have confirmed that Helicobacter spp. can induce a lymphocytic gastritis in these species. In our hospital, many patients evaluated for clinical signs of gastritis have biopsy-confirmed Helicobacter infection associated with lymphocytic gastritis, where no other cause for the gastritis or clinical signs can be found. Symptoms and histologic disease have resolved in most, but not all, following combination antibiotic-antacid therapy.
Diagnosis of Helicobacter infection is confirmed by gastric cytologic findings or results of biopsy. Cytologic analysis of gastric mucosal biopsy impression smears stained with new methylene blue is a sensitive test to confirm presence of Helicobacter organisms. Cytologic findings obtained by endoscopic brush of the gastric mucosa are less sensitive. Routine hematoxylin and eosin (H&E) stain histopathologic study is usually adequate to identify the organisms in gastric biopsy specimens. Use of a silver stain (e.g., Warthin-Starry stain) is best, especially to identify organisms located in the deeper areas in the gastric glands and mucosa.
Biopsy specimens obtained by endoscopy can be rapidly tested for urease production by placing the biopsy sample in a medium containing urea and a pH indicator. Urease-producing Helicobacter organisms in the specimen convert urea to ammonia, causing a color change in the medium. Commercial test kits are used routinely in humans to rapidly screen endoscopic biopsy samples for Helicobacter (CLO Test[†††]). These tests are sensitive and specific for Helicobacter and work well to detect infection in dogs and cats. In our hospital, gastric biopsy specimens from all dogs and cats undergoing gastroscopic examination for vomiting are screened for the presence of urea-producing organisms using this type of test, in addition to doing cytologic studies of gastric biopsy specimens or mucosal brushings. If cytologic examination reveals the presence of spiral organisms and the urea test is positive, treatment for Helicobacter is started pending histopathologic results. If no other cause of vomiting is revealed by histopathologic studies, treatment for Helicobacter is continued for at least 14 days. (See the following discussion.)
Urease production by Helicobacter spp. is also the basis for the carbon-14 breath test, which was designed to noninvasively detect infected patients and to monitor treatment efficacy. Limited clinical application indicates that this test might eventually be useful in dogs and cats. Measurement of humoral IgG to H.pylori is a sensitive, specific, and noninvasive method of diagnosis in humans. Naturally and experimentally infected dogs and cats also produce antibody titers; however, a serologic test has not been available for use in dogs and cats. Most species of Helicobacter are very difficult to culture, and this method is not recommended for diagnosis. Electron microscopy, polymerase chain reaction, and in situ hybridization are techniques used to identify species and subspecies.
Endoscopic appearance of suspected Helicobacter- associated gastritis is variable, ranging from a normalappearing mucosa to mucosal hyperemia to punctate erosions. Some patients will have a diffuse nodular gastritis with a raised follicular appearance (Figure 5-7; see color plate) caused by accumulations of lymphocytes. Histologic findings associated with Helicobacter in humans, dogs, and cats vary in severity from mild vacuolization of surface epithelium to lymphocytic-plasmacytic or neutrophilic mucosal inflammation. Lymphoid nodules occur in more severely affected patients. Infected dogs and cats that have mild histologic gastritis are often non- symptomatic, whereas those with moderate to severe histologic gastritis are symptomatic.
Uncertainty regarding the pathogenicity of Helicobacter infection in dogs and cats raises another fundamental question for the clinician: Should Helicobacter infection be treated? Based on current information and clinical experience, a logical approach to this question is to first rule out other causes of chronic vomiting. Anthelmintic treatment for gastric nematodes (refer to the discussion of parasitic gastritis), followed by a complete blood count (CBC), biochemical profile, urinalysis, and abdominal radiographs, should be done initially. Endoscopic biopsy to confirm the presence of both Helicobacter infection and gastritis should then be considered. In our hospital, treatment for Helicobacter is recommended for dogs and cats in which biopsy has confirmed the presence of Helicobacter-associated gastritis for which no other cause of the clinical signs can be identified. For symptomatic patients in which endoscopy is not an option, the question that frequently arises is, Should the patient be treated empirically for Helicobacter-associated gastritis? This issue is debatable. If the patient is not systemically ill and is not losing weight, and if metabolic causes of chronic
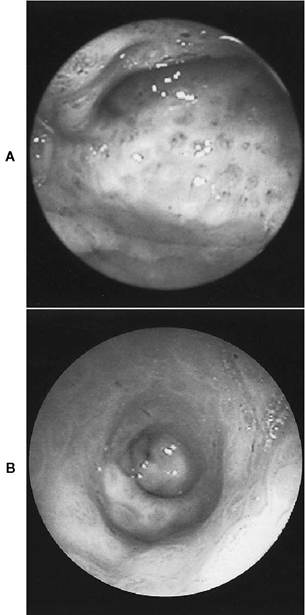
Figure 5-7 Helicobacter gastritis. A, Endoscopic view of the gastric body and incisura in a 3-year-old English bulldog with chronic intermittent vomiting. Raised nodules, some with a central reddened craterlike appearance, were present throughout the body and antrum. B, Endoscopic view of the pyloric antrum from the same dog showing a diffusely nodular mucosa. The pylorus is seen distally in the center of the image. Biopsy revealed the nodules to be accumulations of lymphocytes. Urease-positive Helicobacter organisms were present on the surface musosa and extending into the gastric pits. Clinical signs resolved after treatment with omeprazole (0.3 mg/lb every day) in combination with amoxicillin (10 mg/lb 2 times a day) for 14 days. (See color plate.)
vomiting and GI foreign body have been ruled out, a 14-day therapeutic trial for Helicobacter- associated gastritis is a therapeutically and economically reasonable approach.
Treatment of Helicobacter is difficult because the organism quickly develops resistance to most antibiotics when used as a single-drug treatment. Many regimens have been developed to treat Helicobacter gastritis in humans, using one to three antibiotics in combination with an antisecretory drug and/or a bismuth-containing compound. Acid suppression renders the organism more susceptible to the effects of antibiotics, and bismuth has antimicrobial activity against Helicobacter. Multiple-drug therapy using various combinations of metronidazole or bismuth with an antibiotic (tetracycline, amoxicillin, or azithromycin) and an antisecretory drug (H2- receptor antagonist or omeprazole), given for 10 to 14 days,is considered to be the most effective treatment in humans. However, compliance and side effects are limitations to these multidrug treatments. Dual-therapy protocols using amoxicillinomeprazole or azithromycin-omeprazole for 10 to 14 days are similar in efficacy to the three- or four- drug protocols in humans. Several two-, three-, and four-drug protocols have been extrapolated for use in dogs and cats. In my experience, dual therapy using amoxicillin or azithromycin in combination with omeprazole for 14 days is effective, well tolerated, and economical. The following is a suggested protocol for treatment of dogs and cats:
• Amoxicillin (10 mg/lb every 8 hours) plus omeprazole (0.35 mg/lb every 24 hours) is given for 14 days.
• Azithromycin (2.5 mg/lb every 24 hours for cats, 5 mg/lb every 24 hours for dogs) can be substituted for amoxicillin if incomplete response or relapse appears to have occurred.
• Metronidazole (5 mg/lb every 8 hours) can be added to either of the above treatments to treat suspected relapse for an additional 7 to 14 days.
Parasitic Gastritis
Gastric parasites have generally been regarded to be an infrequent cause of clinical disease in dogs and cats. Infrequency of diagnosis might be explained in part by difficulty finding the ova or adult parasites. Diagnosis of Physaloptera rara in the dog by fecal flotation is difficult because few ova are shed. Diagnosis of Ollulanus tricuspis, the gastric nematode of cats, is also difficult and requires examination of the vomitus for adult parasites. The increased use of endoscopy in chronically vomiting animals has revealed that gastric nematodes might be a more common cause of chronic gastritis than was once thought. In our hospital, gastric parasites have been diagnosed via endoscopy in several dogs and cats
with chronic vomiting where the only abnormality found was a single parasite attached to the gastric mucosa. Treatment for these parasites has resolved the clinical signs. Adult worms are easily identified as 1- to 4-cm-long nematodes in the fundus or antrum, but the smaller larvae are difficult to visualize. Some parasitized animals have gastric erosions and moderate lymphocytic-plasmacytic or eosinophilic gastritis. Because nonendoscopic diagnosis is difficult, it is advisable to treat chronically vomiting dogs and cats that are not systemically ill for gastric parasites before recommending extensive diagnostic tests and endoscopy. Treatment with a single dose of pyrantel pamoate (2.3 mg/lb orally) eliminates Physaloptera from dogs, whereas cats require two doses (2.3 mg/lb) given 3 weeks apart. Treatment for Ollulanus is uncertain; however, fenbendazole (4.5 mg/lb every 24 hours for 2 days) appears to be effective in cats.
Chronic Gastritis of Unknown Cause
Lymphocytic-plasmacytic gastritis is a common histologic diagnosis characterized by gastric mucosal infiltrate with lymphocytes and plasma cells, but without evidence of an underlying cause. Three types have been described based on histologic appearance. Diffuse superficial gastritis is characterized by mucosal infiltrate with lymphocytes and plasma cells, often involving full thickness of the mucosa. Atrophic gastritis is characterized by severe inflammatory infiltrate with reduced mucosal parenchyma and loss of gastric glands and prominent fibrosis. Hypertrophic gastritis is characterized by diffuse or focal mucosal hypertrophy with variable inflammatory infiltrate and fibrosis (see discussion of pyloric mucosal hypertrophy). Plasmacytic-lymphocytic gastritis usually occurs as part of the more diffuse syndrome of IBD and likely has a similar etiopatho- genesis. A permeability defect in the gastric mucosal barrier, possibly caused by dietary sensitivity, drug- induced damage, or infection, might allow abnormal absorption of luminal antigens into the mucosa, thereby initiating an immune-mediated response. Clinical, laboratory, and radiographic findings are nonspecific, and diagnosis is based on results of biopsy. Severe lymphocytic infiltrate can sometimes be difficult to distinguish from gastric lymphoma, particularly when evaluating small endoscopic biopsy specimens. Treatment is essentially symptomatic, centering on dietary protein change coupled with immunosuppressive therapy (Box 5-6).
Eosinophilic gastritis is characterized by diffuse mucosal infiltration predominantly with eosinophils; discrete granulomatous masses with ulceration and necrosis occur rarely. The etiology and pathogenesis are unknown, but hypersensitivity to dietary antigens is a likely cause in some; an immune response to migrating parasites or microbial antigens is another suggested but unproven cause. Many but not all animals with eosinophilic gastritis have peripheral eosinophilia. Diagnosis is based on gastric biopsy results obtained after other causes of vomiting in patients with eosinophilia, such as GI parasitism, hypoadrenocorticism, mastocytosis, and heartworm disease in cats, have been ruled out.
Treatment of lymphocytic-plasmacytic and eosinophilic gastritis in most instances is based on dietary change and immunosuppressive therapy. Dietary change using a diet consisting of a novel protein that has not been part of that animal's previous diet (e.g., fish, venison, rabbit, cottage cheese) may help control the disease but is seldom effective as the sole treatment. Most patients require initial treatment with corticosteroids, and sometimes with azathioprine, to gain clinical remission. Much individual variation in response to treatment occurs. For dogs, initial treatment with prednisone, 0.5 mg/lb every 12 hours orally for 7 to 10 days, followed by an additional 7 to 10 days at 0.5 mg/lb every 24 hours orally is usually effective to induce a remission of clinical signs. The dose should then tapered to an alternate-day treatment for the next several weeks. Depending on the clinical response, prednisone dosage is further tapered by 50% decrements until it can be discontinued without recurrence of clinical signs. Cats tend to require a higher initial dosage, usually 1 to 2 mg/lb every 12 hours orally for 10 to 14 days, followed by gradually tapering doses for the next several months. Occasionally some patients do not respond well to corticosteroids or will require unacceptably high dosages to maintain remission. In this instance azathioprine is a good alternative or can be used as an adjunct to corticosteroids. In dogs azathioprine can be started at a dose of 0.45 mg/lb every 24 hours orally for 10 to 14 days. At the same time the daily dose of corticosteroid is decreased by 50%. Azathioprine and prednisone are then alternated on a daily basis. Depending on the response, the corticosteroid dose can gradually be tapered and eventually eliminated. Remission may require continued alternate- day treatment with azathioprine. Cats are very sensitive to myelotoxic and hepatotoxic effects of azathioprine; a low dose of 0.1 to 0.2 mg/lb every 48 hours is usually safe in cats. Reversible bone marrow suppression, usually occurring within the first 2 to 6 weeks of therapy, is the most common side effect of azathiaprine. A CBC should be done every 14 days during the first 2 months of therapy and at monthly intervals thereafter. If neutropenia or thrombocytopenia occurs, the drug should be stopped. Less frequent side effects are vomiting, hepatopathy, and rarely pancreatitis. The long-term prognosis for most patients with lymphocytic- plasmacytic and eosinophilic gastritis is good. Most respond well to corticosteroids and dietary changes, although some cats do not respond to even aggressive treatment. Remission can often be maintained with carefully controlled diets; however, long-term low-dose corticosteroid or azathioprine therapy is necessary in some. Rarely some patients have large eosinophilic granulomatous masses that initially require surgical resection to relieve partial luminal obstruction. These patients respond surprisingly well postoperatively but still require dietary and immunosuppressive treatment.