DIARRHEA
Decisions frequently revolve around such questions as, What are the most meaningful initial clinical tests? When and for how long should empirical treatment be tried? What are the most appropriate medications to use for empirical treatment trials? When should a detailed diagnostic work-up, which often includes GI function testing and intestinal biopsies, be recommended? This section and the chapters on small intestinal (Chapters 6 and 7) and large intestinal (Chapter 8) disorders describe an organized approach to the problem of diarrhea that is applicable to any practice setting.
Diarrhea is defined simply as passage of feces that contain an excess amount of water. This results in an abnormal increase in stool liquidity and weight. In some patients there may simply be an increase in frequency of defecation. Diarrhea has also been described in broad, simple terms as “the too rapid evacuation of too loose stools.” Definitions notwithstanding, however, it is most important that the clinician carefully determine exactly what the owner means when the term diarrhea is used. The owner’s interpretation is often not as encompassing as the clinician’s. To some people diarrhea indicates only profuse, watery stools. In fact, any variance from what is considered normal for a patient in terms of frequency and consistency should be considered potentially abnormal and worthy of discussion.
Although a variety of symptoms can be caused by intestinal disorders, diarrhea is the hallmark sign of intestinal dysfunction. It can result from primary intestinal disease (e.g., parasitism, various inflammatory disorders, infectious problems, neoplasia), disorders of the liver or pancreas that affect normal intestinal digestive and absorptive processes, and a number of other factors or conditions that adversely affect intestinal function in some way (e.g., dietary indiscretion, adverse food reactions, drugs [e.g., antibiotics, cardiac glycosides], systemic disorders including renal failure, hypoadrenocorticism).
Diarrhea is often classified according to location (small or large intestinal in origin), mechanism^) of diarrhea (osmotic—decreased solute absorption, secretory—hypersecretion of ions, exudative—increased permeability, and abnormal motility), and etiology. Most small animals with diarrhea can be successfully treated. Clinicians are cautioned, however, that patients with diarrhea that do not respond satisfactorily to routine care within a reasonable period of time, as determined by the patient's overall condition, frequency of clinical signs (increasing?), and presence of any significant laboratory abnormalities, should be thoroughly investigated to determine the cause of the problem before it becomes significantly chronic and potentially nonresponsive to any treatment that is administered. Intestinal biopsy is often required for diagnosis in patients with chronic, poorly responsive diarrhea.
Historical Findings—Overview
It is clear that a great number of problems can cause diarrhea. The clinician is faced with the tasks of formulating a well-directed diagnostic plan from a variety of available clinical tests and accurately selecting an effective therapeutic regimen from a wide array of diets and pharmaceuticals. This all too often has to be accomplished with cost-containment factors foremost in the owner's mind.As a result it is extremely important that a thorough history be obtained so that a limited list of most likely diagnostic possibilities can be accurately determined. This is best done by asking a broad-based series of questions in an orderly manner. Box 1-10 provides a list of questions to ask when interrogating an owner whose pet has diarrhea.
The first step involves establishing the duration of clinical signs as clearly as possible. It is important to ascertain how frequently a patient's stools are actually observed. Patients that live primarily outdoors or that are only casually watched when they are outside may have been experiencing abnormal defecations longer or more persistently than the owner may actually realize.
Emphasis is also placed on a review of the clinical course (e.g., acute and short duration, acute onset and then persistent for several weeks or more, intermittent initially but now more persistent, chronic [more than 1 month] and unrelenting).Next, a clear description of the nature and character of the stool is obtained. This will help differentiate small bowel from large bowel disorders (Table 1-4). Tests and treatment often vary for small and large intestinal disorders, making this initial characterization very important. Because large bowel type of problems occur so commonly, I often begin by asking questions relative to this area of the GI tract. Specifically, the presence or absence of mucus (Figure 1-13), fresh blood, straining, and any change in frequency of defecation are discussed. A rough estimate of fecal water content is made (e.g., Are the stools profuse and watery in nature? Generally soft formed?). Small bowel diarrhea is characterized by passage of increased volumes of fecal material.
The vaccination history, dietary history, and environmental history (potential for dietary indiscretion, exposure to any infectious or parasitic agents) are always discussed, and valuable diagnostic clues are often elucidated, especially in patients with acute diarrhea. Any recent history of drug administration should also be reviewed, because some pharmaceuticals could be implicated as causative agents (more so in patients with acute diarrhea). Sometimes the patient's lifestyle plays an important role in the development of diarrhea. For example, working dogs such as sled or police dogs may experience diarrheal episodes during stressful times. Sled dogs sometimes exhibit explosive diarrhea, with or without blood, at the start of or during a race. In police dogs (frequently German shepherds), diarrhea, which may be consistent with either small or large bowel type of signs, and other GI symptoms can be related to intense work situations. Home environment and a patient's individual personality type (e.g., excitable, aggressive) may play a role in causing diarrhea in dogs with irritable bowel syndrome.
The initial phase of the interview is completed with an assessment of the patient's overall condition, with emphasis on attitude (alert/respon- sive/active versus variable degrees of lethargy) and whether there has been any weight loss. The clinician has now had an opportunity to gain perspective regarding how the case should be approached diagnostically and therapeutically and, very importantly, whether or not there should be some sense of urgency in expediting the initial plan (e.g., parvoviral enteritis, intussusception, symptoms including abdominal pain, chronic wasting disease associated with a severe protein-losing enteropathy condition). More detailed information regarding the meaning of historical findings is provided in the following discussion.
Stool Characteristics
Table 1-4 outlines historical and gross fecal characteristics useful in differentiation of small and
BOX 1-10
Questions to Ask in the Investigation of Diarrhea
1. Was the onset recent and acute? If so:
a. Is this a young patient that was just obtained from a locality where there was close contact with other animals (e.g., pet store, kennel, humane shelter)? If so, assume parasitism (including Giardia) and/or viral infection as most likely causes.
b. Are any contact animals in the immediate home environment affected?
c. Has the patient recently been to any area frequented by other animals (e.g., parks, pet shows)?
d. Is the vaccination history current?
e. Has the patient had access to drinking pond or stream water? Strongly consider Giardia in endemic areas.
f. Could the patient have ingested garbage, spoiled food, or any toxins? Concomitant systemic signs are often present (e.g., vomiting, lethargy).
g. Can administration of any drugs, especially antibiotics, be temporally related to the onset of diarrhea?
h. Has there been a sudden diet change, especially to a high-fat, meat-based canned food?
i. Can any stress factors be associated with the onset of diarrhea (e.g., boarding, conflictual problems in the home environment, any situation that causes apprehension)?
j.
Is the diarrhea associated with other symptoms (fever, vomiting, lethargy, weakness)? Diagnostic tests and supportive care are often indicated.2. Is the diarrhea of chronic duration (longer than 2 to 3 weeks)? If so:
a. For how long a period of time?
b. Intermittent? Persistent?
c. Has there been a change in appetite (ravenous, decreased, intermittent changes, pica)?
d. Has there been any weight loss? Chronic wasting disease with a decreased appetite suggests possibility of benign moderate to severe infiltrative disease or neoplasia.
e. Is there any history of flatulence or borboryg- mus?
f. What is the patient’s normal environment like (indoors versus outdoors, contact with parasite- infected environment, working dog or pet, identifiable stressful events in patient’s environment)? Has the patient lived in or traveled to any areas where histoplasmosis is known to be a problem? Parasitism can be a factor in any patient with diarrhea, acute or chronic.
g. Has the patient been eating a poor-quality diet?
h. What is the patient’s breed and character?
German shepherds have a high incidence of inflammatory small intestinal disease, intestinal bacterial overgrowth, and pancreatic disease. Shar-peis have a high incidence of inflammatory small intestinal disease and intestinal bacterial overgrowth. Hyperexcitable or nervous dogs may be prone to irritable bowel syndrome.
i. Is the patient a cat 5 or more years of age? Hyperthyroidism must be considered.
3. What are the characteristics of the stools?
a. Size and volume?
b. Consistency? Watery? Soft formed? Are any of the stools or portions of stools that are passed during a given day normal?
c.Is there any undigested food present?
d. Frequency?
e.Is any blood or mucus present?
f. Is there any incidence of tenesmus? Tenesmus suggests distal colonic, rectal, or anal disease.
g. Timing? Is there a need to defecate frequently during the night? Urgency?
h. If the patient is a cat, does it discharge abnormal stools next to or at a distance from the litter box? This often suggests a large intestinal problem such as colitis.
large bowel disorders.When asking owners questions about stool characteristics, it is often necessary for clinicians to describe what they mean in simple terms.
For example, owners sometimes misinterpret questions about presence of mucus in the stool. If there is uncertainty, it is useful for the clinician to use such descriptive terms as “clear gel,” “appearance of a clear coating around the stool,” or even “appearance of ‘gloppiness’ to the stool.” Owners who initially denied presence of mucus may change their answer to a more accurate one once they have a better understanding of what mucus in fecal material may look like. Indeed, sometimes mucus is difficult to identify, especially in liquid stools in which there is thorough admixture of mucus with water or when loose stool is mixed in with cat litter. Occasionally patients with frequent urgency to defecate will expel only clear mucus. This might be described by the owner as a “thick, ropy, clear liquid.” I have on occasion observed owners entering the examination room with a thick strand of clear mucus on their arm, having been deposited there by their cat or small dog as they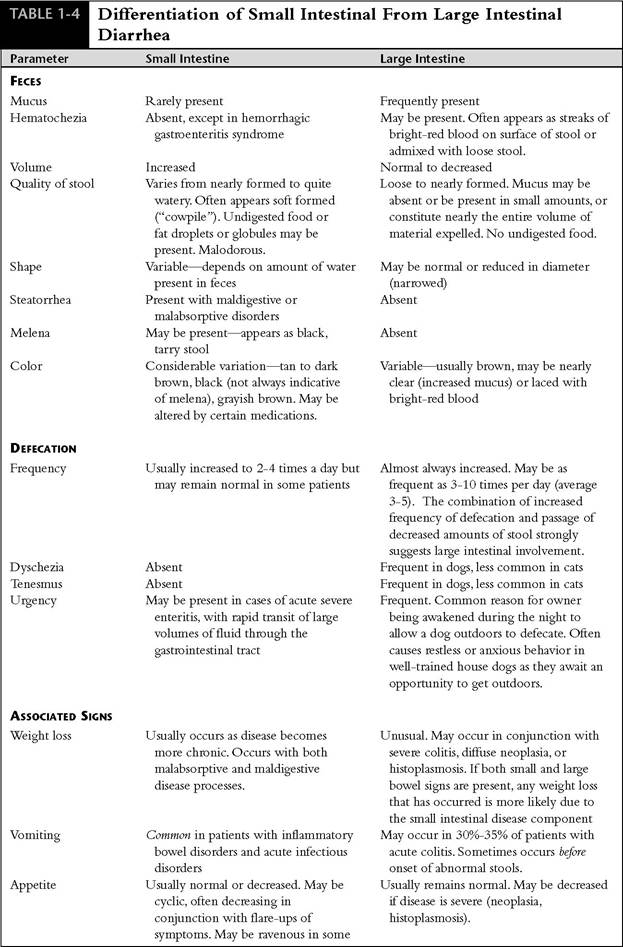
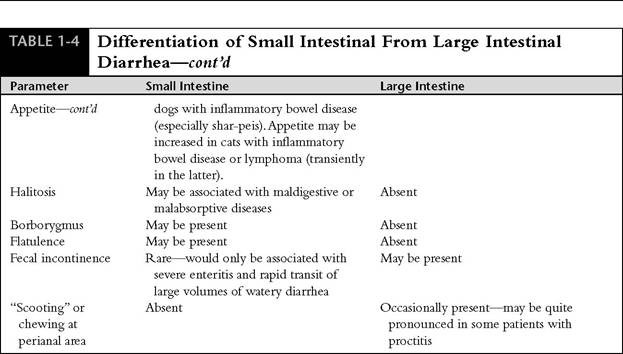
Figure 1-13 Stool passed by a dog exhibiting a sense of urgency. Diarrhea had begun several days earlier. A majority of the stool is mucus, a characteristic that is consistent with a large bowel disorder.
held it in their arms in the waiting room. The initial line of questioning is readily apparent when this occurs!
Two of the most useful questions to ask relative to presence of a large bowel disorder are whether there is any fresh blood (bright-red blood) in the stool or any evidence of straining to defecate (Figure 1-14). Once again, communicating a clear description of our interpretation of these findings, without leading the owner into an answer, is very important. The owner must be made comfortable enough to acknowledge when he or she is not certain of the answer. If the history is unclear, the patient can be hospitalized for further evaluation or the owner can, newly armed with specific ideas about what to look

Figure 1-14 Two-year-old mastiff with signs consistent with chronic large bowel diarrhea. One of the major clinical signs was dyschezia (straining to defecate), which had been occurring over the last year. Typically the dog would crouch for several minutes, as is shown here, while passing only a small amount of stool. The dog would then walk around for a few minutes and then crouch to try to pass stool again. Only small amounts of stool were passed at a time. These signs were consistent with a chronic large intestinal disorder. Colon biopsies were obtained at colonoscopy and revealed chronic moderate to severe lymphocytic-plasmacytic colitis. A stool sample was also positive for Clostridium perfringens enterotoxin. Treatment included both sulfasalazine for chronic colitis and tylosin for C. perfringens enterotoxicosis. Dietary therapy included fiber supplementation.
for, observe more closely in the home environment.
When asked if there has been blood in the stool, the owner may picture large pools of blood, when in fact blood in the stools of patients with a large bowel disorder often appears as small droplets or streaks that could easily be missed by a nondiscerning observer. This is compounded by the fact that blood may be present only intermittently. A differentiation must also be made regarding stool color when blood is present (hematochezia versus melena). The origin of bright-red blood (hema- tochezia) is generally anal, rectal, or descending colon. The cause of hematochezia can usually be more clearly determined by asking if the stools are consistently formed, with blood present on the surface of the stool, or loose, with blood on the surface or admixed in the stool. Dogs that pass formed stools with blood on the surface usually have rectal polyps (passage of stool over a polyp often causes it to bleed) (Figure 1-15), whereas those that pass soft stools with blood most often have some type of inflammatory or irritative disorder. Passage of formed stools with fresh blood in cats is most often related to the presence of abrasive material (e.g., hair, particulate matter from ingestion of prey) passing along the colonic mucosa (Figure 1-16). Rectal polyps are extremely uncommon in cats. Occasionally cats with colitis will pass consistently formed stool with blood on the surface (this is unusual in dogs).
The various causes of hematochezia are summarized in Box 1-11. Melena describes dark, tarry stools resulting from digested blood. The origin may be from the pharynx, lungs (i.e., coughed up and swallowed), esophagus, stomach, or upper
Figure 1-15 Close-up endoscopic view of a large rectal polyp with a friable surface in a 10-year-old neutered male Great Dane. The primary clinical sign was passage of consistently formed stools that occasionally had streaks of fresh blood on the surface. The polyp was exteriorized through the anus and excised.
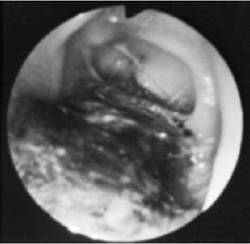
Figure 1-16 Abrasive clumps of hair in the colon of a cat with intermittent hematochezia and mild lymphocytic-plasmacytic colitis. Commonly the cat’s stools were formed but had blood on the surface and contained hair. The hematochezia was thought to be primarily a result of the abrasive effect of hair on the colonic mucosa. The hair clumps observed in this photograph remained after two warm-water enemas were administered in preparation for colonoscopy. (From Leib MS: Colonoscopy. In Tams TR, ed: Small animal endoscopy, St. Louis, 1990, Mosby.)
small intestine. Tarry stools result from bacterial breakdown of hemoglobin. There must be a sufficiently large amount of blood present before stools will appear tarry. In one retrospective study that evaluated 43 dogs with gastric and/or duodenal ulceration, it was found that only 40% of the dogs had melena. It must also be noted that not all patients with dark stool have melena.
Dyschezia is defined as difficult and/or painful defecation. Tenesmus refers to persistent or prolonged straining that is usually ineffectual. It generally indicates a sense of urgency. Both dyschezia and tenesmus can be associated with alimentary, as well as genitourinary, disorders. The most common alimentary tract causes are colitis, proctitis (inflammation of rectal mucosa), and constipation. Because owners frequently interpret straining to indicate constipation, it is essential that the clinician differentiate constipation from the straining that is often associated with large bowel inflammation and diarrhea at the outset. Experienced clinicians recognize that many telephone calls involving a request for advice on how to treat a constipated pet at home actually involve an inaccurate assumption by the owner. Frequently tenesmus is caused by colitis and/or proctitis in these patients. The differentia-
BOX 1-11
Causes of Hematochezia
Anal Canal
Fissures
Anal sacculitis
Trauma
Neoplasia
Rectum and Colon
Proctitis
Colitis
Idiopathic
Infectious
Campylobacter
Clostridium perfringens
Parvovirus
Parasitism
Whipworms
Coccidia
Hookworms
Mucosal trauma
Passage of foreign material (common cause of hematochezia associated with formed stools in cats—especially hair)
Automobile trauma
Iatrogenic (e.g., thermometer or enema tube damage)
Prolapsed rectum
Neoplasia
Rectal polyp (common cause of hematochezia associated with formed stools in dogs)
Rectal adenocarcinoma
Lymphoma
Ileocecocolic Area
Ileocolic intussusception Cecocolic intussusception tion is readily made through a review of the history and physical examination.
Other important clues that indicate the onset of a large bowel diarrhea disorder include increased frequency of defecation with evacuation of only small amounts of stool (and in some patients eventually only mucus), defecating in abnormal places (cats), well-trained house dogs acting out of character by defecating in the house (usually due to a sense of urgency to defecate) while the owner is away or unavailable to allow them outside, and dogs waking their owner frequently during the night to go outside (sense of urgency) when normally they sleep through the night. Sometimes cats with colitis will defecate next to but not in the litterbox. The first question to ask if any of these abnormal patterns is described is whether the stools and act of defecation (if observed) are normal or abnormal. Frequently information to support existence of a large bowel diarrhea disorder will be elucidated. If the stools are consistently normal, a behavior disorder should be suspected (e.g., cognitive dysfunction syndrome in older dogs and cats). Diagnostic work-up and/or initial empirical treatment can then be accurately directed.
Small bowel diarrhea is often characterized by an increased frequency of defecation with evacuation of larger than normal amounts of soft-to- watery stool. Color variations range from light tan to darker brown to orange to black (melena). Dyschezia and tenesmus are not characteristics of a small bowel disorder and are apparent only if a large bowel disorder is present as well (this is an important historical point, indicating probable diffuse intestinal involvement). Urgency may be present in acute small bowel disorders or in those associated with cramping. Generally, rapid evacuation of a large volume of watery diarrhea ensues (as opposed to large bowel problems in which only a small volume is passed). Steatorrhea may cause the feces to have an oily appearance and/or a grayish coloration. Presence of undigested food indicates maldigestion, which is generally due to either EPI or rapid bowel transit time. Weight loss that occurs in conjunction with chronic diarrhea is most often due to a significant disorder of malabsorption or maldigestion and may be associated with a guarded prognosis. Diagnostic testing sufficient to determine a definitive diagnosis should be expedited.
Associated Clinical Signs
Clinical signs that occur in conjunction with diarrhea often provide important clues regarding area of involvement and the potential seriousness of the condition. Important ancillary clinical signs that the clinician should ask about when reviewing the history include vomiting, weight loss, appetite change, flatulence, and borborygmus. Flatulence and borborygmus most often indicate small intestinal dysfunction. These symptoms are discussed in detail later in this chapter. Whereas vomiting commonly occurs in patients with small intestinal disease, especially inflammatory and parasitic disorders, it is also sometimes observed in patients with large intestinal problems. It is estimated that up to 35% of dogs with acute colitis vomit in addition to exhibiting typical signs of large bowel diarrhea. A majority of these patients that undergo gastroscopy and colonoscopy have normal findings on stomach biopsy. In fact, in some of these patients, vomiting actually precedes the onset of diarrhea by several hours to 1 to 2 days.Vomiting and inappetence often precede the onset of diarrhea in dogs with parvovirus enteritis. These facts highlight the importance of looking for physical evidence of intestinal disorders in patients presented for acute vomiting. This is accomplished through a physical examination, which must include a rectal examination to evaluate for increased mucosal sensitivity (suggestive of procti- tis/colitis) and stool characteristics. Dogs with severe enteritis that have not yet passed any stool may release a large amount of watery, bloody diarrhea as soon as a rectal examination is performed.
The presence of weight loss and inappetence in conjunction with chronic diarrhea suggests a significant small intestinal disorder (e.g., inflammatory bowel disease, lymphangiectasia, histoplasmosis, neoplasia), and their presence should hasten the clinician’s efforts toward making a definitive diagnosis. The combination of chronic diarrhea, weight loss, and increased appetite in cats suggests hyperthyroidism, inflammatory bowel disease, EPI, (rare in cats), and occasionally lymphosarcoma (some cats with GI lymphoma actually have an increased rather than decreased appetite). This combination of signs in dogs is most consistent with EPI. Characteristics of diarrhea in patients with EPI include voluminous “cowpile”- consistency stools that are often rancid in nature. Coprophagy is an ancillary sign that frequently occurs in dogs with EPI.Weight loss and inappetence rarely occur in dogs and cats with intestinal disorders limited to the large bowel.
Young to middle-age dogs that have chronic unrelenting diarrhea with minimal to no weight loss and a consistently normal appetite most often have a more significant problem in the large intestine than in the small bowel. I have found that the large bowel signs in these patients are often mild to subtle (e.g., mild dyschezia with transient flare-ups, soft stools that only occasionally contain blood, intermittent passage of mucus). The prevailing sign is that the stools are never consistently normal. If small bowel disease is present as well it is generally mild, so inappetence and weight loss would not be expected. The most common combination of findings is mild to moderate colitis, mild inflammatory bowel disease of the small intestine, and intestinal bacterial overgrowth. Each of these problems needs to be treated appropriately before adequate resolution of signs can be expected. Significant weight loss and/or inappetence occur in association with primary large bowel disorders only when they are severe (e.g., severe colitis, including histiocytic ulcerative colitis of boxer dogs, diffuse neoplasia, or histoplasmosis).
Physical Examination
Physical examination of patients with diarrhea is similar to the thorough evaluation that is done on vomiting patients (see earlier discussion). Along with the history, physical findings help direct the clinician regarding what specific tests, if any, should be done and how quickly work-up should be expedited. Particular attention is paid to the patient’s attitude, hydration, and posture. Depression and dehydration occurring in conjunction with acute diarrhea suggest an infectious or toxicity-related cause. Careful evaluation for any signs of sepsis (fever or hypothermia, tachycardia, tachypnea, and signs of shock, which may include changes in mucous membrane color to brick red or, alternatively, pale, cool extremities and injected membranes) is conducted initially and at any indication that a patient’s condition may be destabilizing again. Abnormal posture (e.g., arched back) may indicate abdominal pain that can be associated with acute or chronic disorders. The neck should be carefully palpated in cats with diarrhea for evidence of an enlarged thyroid nodule (indicating hyperthyroidism). Body weight and overall physical stature should be noted. The act of defecation, especially if there is a history of dyschezia or tenesmus, should be observed by the clinician whenever possible.
Careful abdominal palpation is done to examine for thickened bowel (inflammatory or neoplastic infiltration), intussusception, presence of a mass that could be causing partial intestinal obstruction with resultant diarrhea, and lymphadenopathy (benign or neoplastic). Hepatomegaly suggests the possibility of hepatic disease in a causative role, and patients with acute or chronic severe small bowel diarrhea may have markedly increased fluid in the small bowel. Sensitivity localized to the caudal dorsal abdomen can often be detected in patients with colitis. This area is often not palpated carefully enough by veterinary clinicians.
A rectal examination is always done in dogs to examine for increased mucosal sensitivity, presence of narrowing (e.g., infiltrative disease, stricture), foreign body, or mass effect, and to obtain a fresh stool sample for gross examination. The finger should be rotated 360 degrees in the rectal canal so that as much mucosal contact as possible is made. Rectal polyps, which are often soft, can easily be missed on cursory examination. The perineal area is also examined for evidence of perianal fistulas, perineal hernia, and anal gland disease, all of which can cause symptoms of large bowel disease.
Diagnostic Plan
Specific diagnostic studies performed in patients with diarrhea are generally determined by the following considerations: (1) duration (acute versus chronic [2 to 3 weeks or more]); (2) presence of associated clinical signs such as inappetence, weight loss, frequent vomiting, severe bloody diarrhea, listless behavior (expedite diagnostic efforts if any of these signs are present); (3) environmental history; (4) signalment; (5) localization of the diarrhea to either small or large bowel or both; (6) frequency of diarrhea (intermittent versus chronic and persistent); and (7) physical examination findings. This will help the clinician determine whether a conservative step-by-step approach is feasible (e.g., diagnostic dietary trials, empirical treatment for parasites if screening fecal examinations are negative for parasites, treatment for mild acute colitis) or a more aggressive diagnostic effort is indicated. When evaluating patients with chronic diarrhea, the list of diagnostic tests need not be extensive, just well directed (Figure 1-17).
Acute Diarrhea
Diet-induced problems, viral infections, and parasites are the major causes of acute diarrhea in dogs and cats. Because intestinal parasites may be a factor in any diarrheic state, fecal examinations (direct and flotation) should be routinely done in all patients. Multiple examinations may be required to identify Giardia and Trichuris infections. Examination of fresh saline smears may identify ova, larvae, or motile protozoan parasites. High magnification with moderate light intensity should be used. Adding a drop of iodine may enhance the visibility of Giardia trophozoites and will stop any motion of the organism. Unfortunately, saline smears are not very reliable for diagnosis of Giardia infections (only 40% of dogs infected with Giardia were diagnosed in one study when saline smears were done using fresh stool on 3 separate days). The most accurate practical test for Giardia is zinc sulfate centrifugal flotation for identification of Giardia cysts. Examination of duodenal lavage fluid, obtained via endoscopy or at laparotomy, for trophozoites may also be done but is impractical as an early diagnostic test. A fecal enzyme-linked immunosorbent assay (ELISA) for Giardia- specific antigen has also become available (Figure 1-18). This is a sensitive test and can be easily performed in-house or at commercial laboratories. My preference when examining for parasites in patients with acute diarrhea is to run both a zinc sulfate assay and a test for Giardia antigen. This gives me a high level of confidence in my efforts to more accurately determine whether or not intestinal parasites are present. Empirical treatment for parasites using such drugs as fenbendazole (Panacur) or febantel (contained in Drontal Plus, Bayer, along with pyrantel pamoate and praziquantel) for whipworms and giardiasis may also suggest a diagnosis if their use is successful in resolving the diarrhea.
Although diet-induced enteropathies are common, they are sometimes difficult to diagnose definitively. Acute diarrhea may result from overeating, a sudden change in diet (especially to a canned meat-based food), ingestion of spoiled food, food intolerance, or food sensitivity. The diagnosis is most likely to be made based on history, ruling out other causes, and response to treatment. Strict dietary trials with hypoallergenic diets are indicated more for patients with more chronic signs (e.g., 2 weeks or longer in duration). Dietary therapy for patients with acute diarrhea includes dietary restriction for 24 to 48 hours (to place the intestinal tract in a state of physiologic rest) followed by gradual reintroduction of food using a bland, readily digestible but low-fat diet (e.g., chicken and rice or boiled hamburger and rice in a 1:4 ratio, or a commercial diet of similar formulation) provided in small, frequently fed amounts for several days. Finally, either the regular diet is resumed or a change is made to a new maintenance diet if the previous food is considered unsatisfactory or is thought to have played a causative role in development of the diarrhea.
Patients with such signs as depression, dehydration, and fever in conjunction with acute diarrhea, with or without blood, should be evaluated for systemic abnormalities. The minimum database always includes a CBC, looking for leukocytosis or leukopenia, presence or absence of left shift, and supportive evidence for dehydration (elevated packed cell volume [PCV] and total solids). A blood smear can be evaluated quickly and easily
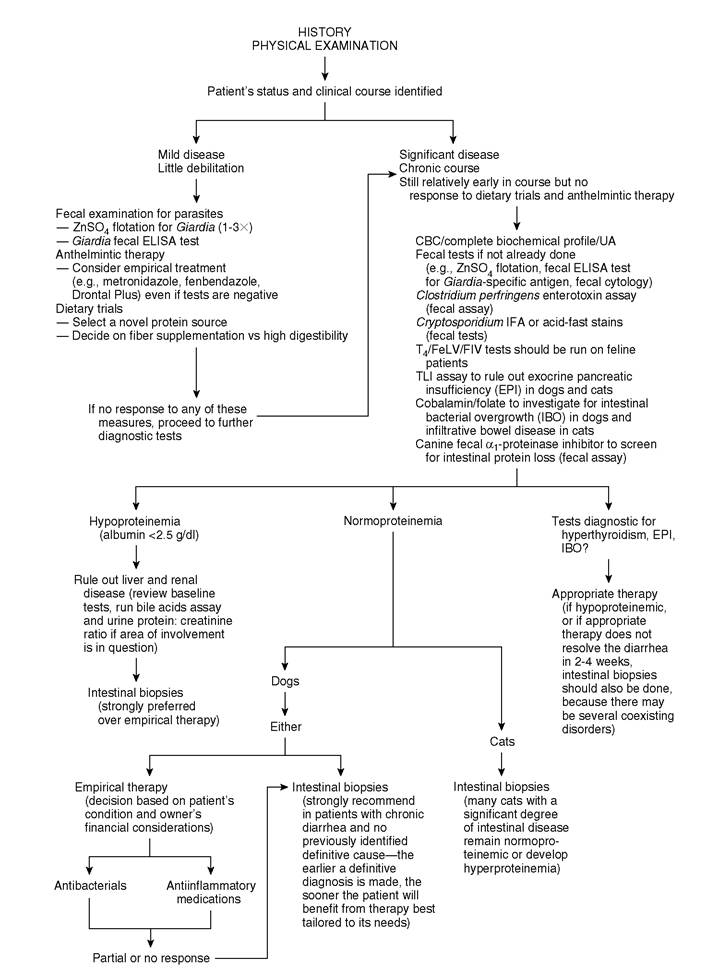
Figure 1-17 Sequential diagnosis of chronic small bowel diarrhea in dogs and cats. ZnSO 4, Zinc sulfate; CBC, complete blood count; UA, urinalysis; ELISA, enzyme-linked immunosorbent assay; T4, thyroxine; FeLV, feline leukemia virus; FIV,feline immunodeficiency virus; TLI, trypsin-like immunoreactivity.
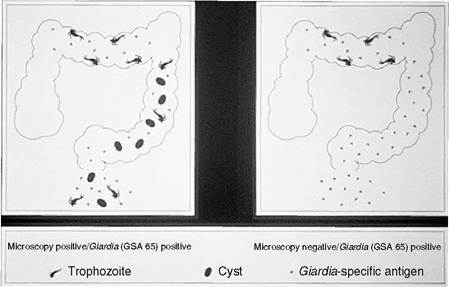
Figure 1-18 This schematic illustrates how the Giardia antigen test works (ProspecT Giardia Rapid Assay, Remel). On the left side there is a depiction of an intestine that contains Giardia trophozoites, Giardia cysts (the oval objects), and Giardia antigen (the small triangles). All three are being passed in the stool, and a direct saline smear for trophozoites, a zinc sulfate test for Giardia cysts, and a Giardia antigen test could all be positive. The right schematic shows a patient that has Giardia trophozoites in the intestine, but there are no trophozoites or cysts being passed in the feces. The only test that will be positive in this situation is an antigen test. Humans and animals that are infected with Giardia can shed cysts intermittently. Therefore, if an antigen test is not done, the diagnosis will be missed if there are no cysts present in the stool sample. I prefer to run this test in addition to running a zinc sulfate test to help make an accurate diagnosis for Giardia. This test can also be used after a course of treatment to check to see if a Giardia infection has been successfully eradicated (the test is run 14 days after the conclusion of therapy).
for an estimated white blood cell count. In patients with hemorrhagic gastroenteritis, there may be a dramatic increase in PCV to levels as high as 70% to 75%. This degree of increase in PCV contrasts with that in parvovirus infection and is the key to diagnosis of hemorrhagic gastroenteritis. If CBC results will not be readily available, a blood smear should be examined for estimation of the white blood cell count. Serial blood counts may be necessary because leukocytosis or leukopenia may be transient. A CBC may also suggest a possible diagnosis of hypoadrenocorticism (lymphocytosis, eosinophilia, mild anemia). Electrolytes (including sodium and potassium), serial blood glucose assessments for evidence of sepsis, and urinalysis both for baseline evaluation of renal function and for serial urine specific gravity levels as an aid in monitoring hydration in patients with normal renal function should also be run.
Hemagglutination, hemagglutination inhibition, or ELISA tests are used to test for fecal shedding of viral antigen. In-office ELISA tests have proven useful in detecting fecal shedding of parvovirus in acute cases and are probably more sensitive and specific than is hemagglutination.
Fecal shedding of viral particles often decreases rapidly, however, so a negative result does not rule out infection. Fecal cultures to examine for Salmonella spp., Campylobacter jejuni,Yersinia entero- colitica, and Shigella are indicated in some situations (e.g., kennel outbreaks, patients recently obtained from pet stores or shelters, households where more than one animal has diarrhea). It is extremely important that proper technique be used when obtaining feces for stool culture (see Chapter 6).
Chronic Diarrhea
Diarrhea that has not responded to conventional therapy within 2 or 3 weeks can be considered chronic. It is then appropriate to recommend that the problem be more thoroughly evaluated by using specific diagnostic tests. Considerable expense may be involved in some cases, so it is always best to start by reviewing the history once again (including differentiation between small and large intestinal involvement or determining that both areas are likely involved) to be as accurate as possible in selecting tests that are likely to provide useful information. Suggested diagnostic strategies for small intestinal and large intestinal diarrhea are presented separately here. An algorithm for sequential diagnosis of chronic small bowel diarrhea is presented in Figure 1-17.
Small Intestinal Diarrhea
Chronic small intestinal diarrhea can be broadly categorized into three groups: maldigestive disease, malabsorptive disease, and functional disorders. A majority of canine and feline patients with chronic small intestinal diarrhea seen in clinical practice have malabsorptive type of problems. There are many causes of intestinal malabsorption. Maldigestive disease is principally caused by EPI.
Maldigestive Disease
EPI is uncommon in dogs and cats. In the past EPI was greatly overdiagnosed and many patients were needlessly and ineffectually placed on pancreatic enzyme replacement therapy. Much of the confusion was caused by the lack of a reliable and definitive test for EPI. Tests commonly used in the past, including the x-ray film digestion test for fecal trypsin activity and the fat (lipomul) absorption test, proved to be insensitive and extremely unreliable. Tests for steatorrhea (staining feces for fat with Sudan stain), amylorrhea (staining for starch with Lugol’s solution), and creatorrhea (staining for protein with standard stains) are reasonable and inexpensive in-house screening tests that can be run, but a significant drawback is that there can be false-negative and false-positive results. The ben- tiromide (BT-PABA) test is sensitive and reliable but cumbersome to perform.
Without question the most sensitive and specific test for EPI is the serum trypsin-like immunoreactivity (TLI) assay. This test simply involves obtaining a serum sample after fasting the patient for 12 to 18 hours (see Chapter 10). Serum TLI has been validated for use in both dogs and cats. Previously the fecal proteolytic activity (FPA) assay was the test of choice in cats. Although EPI is an uncommon disease, it is recommended that a TLI test be run in patients with chronic diarrhea so that EPI can be definitively ruled out early in the course of diagnostic evaluation. Failure to run this simple and inexpensive test may result in needless intestinal biopsies for diagnosis of a suspected malabsorption disorder.
Malabsorptive Disease
Malabsorptive intestinal disease can be divided into protein-losing and non-protein-losing enteropathies. Use of this classification scheme helps the clinician determine to some extent the current degree of seriousness of the condition and thus aids in the decision regarding whether a detailed work-up, including intestinal biopsies, should be expedited versus the feasibility of pursuing conservative therapeutic trials first (e.g., timeconsuming strict dietary trials). In general, dogs with GI signs and a total protein of less than 5.5 g/dl should undergo intestinal biopsy. Dogs with mild hypoproteinemia (5.5 to 5.9 g/dl) should be watched carefully. Cats develop hypoproteinemia much less commonly than dogs. Hypoproteinemia usually indicates a significant degree of disease in cats, and intestinal biopsies should definitely be done if the intestine is considered to be the likely source of the problem.
Baseline tests, including CBC to identify leukocytosis (which suggests inflammatory disease), eosinophilia (eosinophilic enteritis, chronic previously undiagnosed endoparasitism), absolute lymphopenia (often observed in lymphangiectasia), and anemia (blood loss, anemia of chronic disease, nutrient malabsorption); biochemical profile (e.g., hypoalbuminemia, hypoproteinemia, abnormal liver enzymes, exclusion of metabolic disorders); and urinalysis to evaluate renal function and check for proteinuria, should be run in all patients with chronic diarrhea. Even if a CBC and biochemical profile were run previously, during the early days of onset of the diarrhea, it is often useful to repeat these tests at a later time because tests that were previously normal may then be found to be abnormal (see example in Table 1-5).
Hypoproteinemia most often results from disorders of the small intestine (protein loss involves albumin or both albumin and globulin), liver (primarily hypoalbuminemia due to decreased production), and protein-losing glomerulonephropathy (primarily hypoalbuminemia). Although the combination of chronic diarrhea and hypoproteinemia is usually consistent with small intestinal disease, there may still be concurrent disease in the liver or kidneys. It may therefore be necessary in some cases to evaluate these organs thoroughly (e.g., bile acids assay for liver function, urine protein: creatinine ratio to more accurately identify degree of proteinuria).
Fecal cytology may be useful in evaluating patients with chronic diarrhea. A thin smear of stool is stained (e.g., with new methylene blue, Diff-Quik, Wright’s) and examined under high power or oil immersion for the presence of inflammatory cells. Increased numbers of neutrophils appear with inflammatory small or large
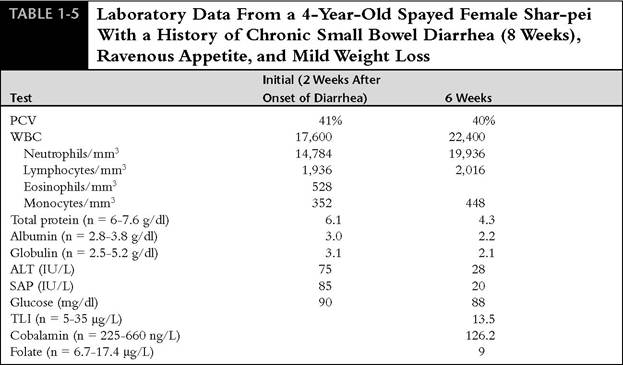
PCV, Packed cell volume; WBC, white blood cell count; n, normal values; ALT, alanine aminotransferase; SAP, serum alkaline phosphatase; TLI, trypsin-like immunoreactivity.
*Note the marked decrease in protein levels over the 6-week time period between sampling, indicating the presence of a significant degree of disease. Intestinal biopsies obtained via endoscopy revealed moderate lymphocytic-plasmacytic duodenitis and ileitis. A TLI test was normal. The low cobalamin level suggests the possibility of intestinal bacterial overgrowth.
intestinal disease or secondary to invasive bacterial enteritis.
The clinician or owner may reasonably elect to try therapeutic trials as the next step in noncompromised normoproteinemic patients. Therapeutic trials could include treating for adverse food reactions (dietary intolerance, food sensitivity); occult parasitic infections (especially giardiasis and whipworm infestation) if this has not already been done (also, successful treatment of giardiasis may require longer than one course of treatment); small intestinal bacterial overgrowth; and Clostridium perfringens enterotoxicosis (usually causes large bowel diarrhea). Dietary trials using hypoallergenic diets or high-quality commercial foods with a novel protein source are the primary diagnostic tool for identifying adverse food reactions. Radioallergosorbent tests, which determine serum levels of antigen-specific immunoglobulin E, have shown poor correlation with oral challenge, skin, and intragastric tests for food allergy. A response to treatment for any of the conditions listed above supports a diagnosis and precludes further work-up. Dietary trials are generally prescribed for 3 to 4 weeks in patients with GI disorders. Some patients will respond favorably within 3 to 14 days.
The next step in diagnosis of suspected malab- sorptive disease, after baseline evaluation has been completed, is to look for evidence of intestinal bacterial overgrowth. The most accurate means of diagnosis is to obtain samples of duodenal fluid for both qualitative and quantitative analysis. This must be done using meticulous sterile technique either at laparotomy or with endoscopic instrumentation. Quantitative duodenal culture is expensive and cumbersome and is generally available only in academic institutions. The most practical method of testing for intestinal bacterial overgrowth is by measuring serum concentrations of vitamin B12 (cobalamin) and folate (see Chapter 7). These assays can be done in both dogs and cats. Because bacterial overgrowth is not uncommon in patients with pancreatic insufficiency, the cobalamin and folate assays should be run if this disorder is suspected. In fact, I generally submit enough serum to run all three special assays (TLI, cobalamin, and folate) rather than running just one or two of the tests. If intestinal bacterial overgrowth is diagnosed, it may be the primary problem or it may be present secondary to some other abnormality that has allowed it to persist. Treatment for bacterial overgrowth involves antibiotics, which may have to be administered for as little time as 1 to 2 weeks or as long as many weeks to months. If a decision is made to treat for bacterial overgrowth rather than do further tests, 2 to 3 weeks is an adequate trial period. If the problem is not resolved at this point, it is generally best to move ahead and look for other concurrent problems.
In addition to intestinal bacterial overgrowth and EPI, low serum cobalamin concentrations have been observed in dogs and cats with severe intestinal disease, in giant schnauzers with inappetence and failure to thrive and the laboratory findings of anemia, leukopenia, and methylmalonyl aciduria, and in many shar-peis with intestinal disease. It is important to evaluate serum cobalamin levels in cats with chronic GI disorders because supplemention with cobalamin by injection can be quite beneficial therapeutically (see Chapter 7).
At this stage the next best step is usually to perform intestinal biopsies. Other procedures that might be indicated in some patients include contrast radiography and abdominal ultrasonography. Contrast studies of the small intestine may help identify segmental lesions, tumors, or foreign bodies. Accurate interpretation of mucosal lesions on contrast studies is very difficult. The decision regarding whether or not a contrast study is done is usually based on physical examination findings (suggestion of a mass or well-localized pain) and survey radiographs. Ultrasonography is frequently recommended over contrast radiography in patients with suspected intestinal disease because intestinal wall thickness can be much more accurately assessed and lesions such as masses and enlarged lymph nodes can be readily detected and also aspirated under ultrasonographic guidance.
Ultrasound scanning of the intestinal tract provides an evaluation of peristalsis, wall thickness and diameter, lesion location, and appearance of luminal contents. Ultrasound is particularly useful in identification of obstruction and its various causes (e.g., masses, foreign objects, inflammatory disease, intussusception). Thickening of the bowel wall can occur in either inflammatory or neoplastic disease processes. Probably the greatest value in performing contrast radiography and/or abdominal ultrasonography in a patient with chronic diarrhea lies in helping make a decision on whether endoscopy will be adequate for obtaining diagnostic intestinal biopsy samples or whether exploratory surgery is indicated (e.g., if there are focal intestinal lesions that may not be reached with endoscopic instrumentation, a mass is present, or there is lymphadenopathy or an intussusception).
The definitive diagnostic step in many patients with chronic, nonresponsive diarrhea is to perform intestinal biopsies either via endoscopy or surgery. In a majority of cats and dogs with chronic diarrhea that exists with or without associated clinical signs (eg., vomiting, appetite change, weight loss), a definitive diagnosis can be established based on endoscopic examination and biopsies. The advantages and limitations of endoscopy are discussed in detail in Chapter 3. In most patients with chronic diarrhea, it is preferred that both upper and lower endoscopy be done so that sections from both the small and the large intestine can be evaluated histologically to determine the extent of a disease process as accurately as possible. In addition, in a majority of dogs weighing more than 8 to 10 lb, a pediatric endoscope can be advanced into the ileum via the colon by an experienced operator. Thus, complete colonoscopy followed by ileoscopy allows for more detailed evaluation of the small intestine (i.e., both upper and lower small intestine are examined and sampled for biopsy). This is especially important in cases in which a disease process may not yet diffusely involve the small intestine (e.g., occasionally, benign inflammatory disease or lymphoma will be found in the ileum but not in the duodenum). Ileum biopsy samples can often be obtained from cats by advancing the biopsy forceps through the ileocolic junction area with the endoscope tip situated in the ascending colon. Multiple forceps biopsy samples (6 to 10) are obtained from each area of intestine examined.
If an exploratory laparotomy is done to obtain intestinal biopsies, the entire bowel should be carefully evaluated. Biopsies of focally abnormal areas should be performed (full-thickness samples) along with one to two normal areas. Many patients with chronic small bowel diarrhea have grossly normal intestine as observed at surgery. Biopsy samples must still be procured! Two or three full-thickness samples are obtained (duodenum and ileum, or duodenum, jejunum, and ileum). A biopsy of any other tissue that appears abnormal (e.g., liver, pancreas, stomach, lymph nodes) should also be performed during exploratory laparotomy.
Biopsies are not often performed as early as they should be in patients with chronic GI disorders. Although the availability of endoscopy and its minimal risk in obtaining tissue samples is well recognized, some clinicians still wait too long to advise owners that a biopsy procedure is definitely needed. Progressive symptoms such as persistent or worsening diarrhea, weight loss, and decrease in appetite, as well as abnormal laboratory parameters such as hypoproteinemia, are reliable indicators that biopsies should be performed. It is important to remember, however, that some chronic intestinal disorders may manifest with only mild symptoms until the disease becomes serious. The patient's condition may then rapidly decline. Routine tests such as a hemogram and biochemical profile are generally very useful in screening for significant intestinal problems. For example, hypoproteinemia should be thoroughly investigated whether or not a patient is demonstrating significant symptoms. If screening tests indicate that the intestinal tract is most likely involved, a strong effort should be made to obtain biopsy samples. A representative case example is illustrated in Table 1-6. This patient should have undergone a small intestinal biopsy procedure much closer to the time the total protein and albumin levels were determined to be 4.1 g/dl and 1.6 g/dl, respectively, rather than 10 weeks later, when the protein level dropped to 2.8 g/dl and the patient was in a somewhat more compromised
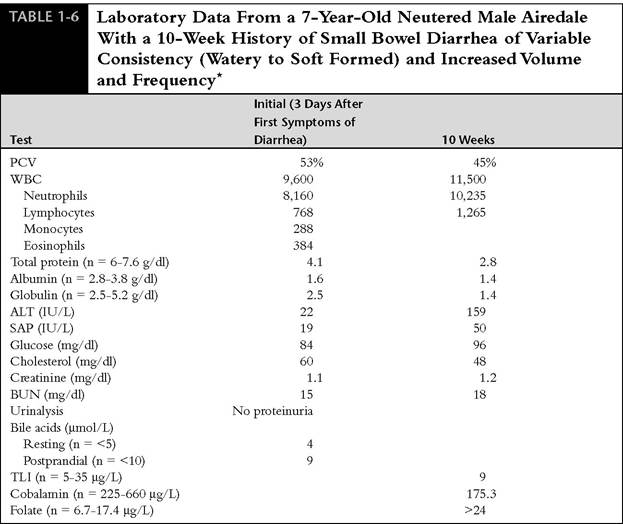
PCV, Packed cell volume; WBC, white blood cell count; n, normal values; ALT, alanine aminotransferase; SAP, serum alkaline phosphatase; BUN, blood urea nitrogen; TLI, trypsin-like immunoreactivity.
*The appetite was fair to good and there was mild weight loss. Initial blood tests 3 days after the onset of diarrhea revealed marked hypoproteinemia (total protein 4.1 g/dl). Based on the degree of hypoproteinemia and hypocholesterolemia, strong consideration should have been given to obtaining small intestinal biopsies at that time rather than waiting to see what type of response could be achieved using empirical treatment. Not all patients with protein-losing enteropathy have chronic diarrhea and/or vomiting. The total protein level dropped to 2.8 g/dl by 10 weeks after the initial tests. Endoscopic biopsies were then obtained from the duodenum and ileum. The diagnosis was lymphangiectasia and mild lymphocytic-plasmacytic enteritis. Note that the absolute lymphocyte levels were subnormal on the initial test and low normal on the follow-up. Many lymphangiectasia patients have an absolute lymphopenia or persistently low normal lymphocyte numbers. The cobalamin and folate levels were consistent with intestinal bacterial overgrowth.
condition. Screening tests for liver and kidney disease done during the initial screening period were normal.
Treatment is then based on a review of the laboratory tests and biopsy results. It is emphasized that some patients with chronic diarrhea may have several disorders at the same time (e.g., inflammatory small bowel disease, intestinal bacterial overgrowth, colitis). A thorough work-up will lead to diagnosis of each disorder, with subsequent development of a comprehensive treatment plan. The likelihood of more rapid resolution of symptoms is much greater when each existing problem is properly treated.
Large Intestinal Diarrhea
As previously stated, large bowel disorders are common in dogs and cats. In mild cases, a diagnosis is often established based on fecal parasite examination (e.g., hookworms, whipworms, coccidia, and Giardia); positive response to empirical treatment for difficult-to-diagnose parasite problems (Giardia and whipworms); response to dietary trials (high-fiber diet, elimination diets); or response to empirical treatment for acute colitis.
Diagnostic tests for chronic large bowel diarrhea principally involve the following:
1. Fecal cytology to look for increased numbers of C. perfringens spores and inflammatory cells (specifically neutrophils), which suggest bacterial or primary inflammatory disease. Fecal or rectal scrape cytology is also useful in identifying Histoplasma organisms.
2. Fecal culture if history or fecal cytology suggests the possibility that bacterial infectious disease exists (Campylobacter, Salmonella).
3. Enterotoxin assay on stool to evaluate for C. perfringens enterotoxicosis.
4. Colon biopsy via colonoscopy (preferred technique) or surgery.
Complete colonoscopy with examination of the rectum, descending, transverse, and ascending colon, cecum, and ileocolic orifice area is preferred. Although examination and biopsy of the descending colon with a rigid colonoscope is commonly diagnostic in patients with large bowel diarrhea, such problems as occult trichuriasis, in which whipworms may be grossly evident in the cecum but not in the descending colon, ileocolic or cecocolic intussusception, typhlitis, or neoplasia that is localized in the transverse or ascending colon may be missed unless a complete examination of the colon is done with a flexible endoscope. Another advantage of using a flexible endoscope is that ileoscopy may be accomplished in many dogs after complete colonoscopy. Biopsy samples should always be obtained during colonoscopy, regardless of gross appearance. Indeed, it is not uncommon for patients with histologic evidence of colitis to have grossly normal colonic mucosa. If biopsy samples are not obtained, the diagnosis may well be missed.
Although it is a sound idea to evaluate patients with chronic large bowel diarrhea thoroughly by including a CBC, biochemical profile, urinalysis, and survey abdominal radiographs in the work-up, it is not always financially feasible for the owner to approve this detailed approach. If cost containment is essential, emphasis should be placed on a thorough history, physical examination with careful abdominal palpation and rectal examination, serial fecal examinations for parasites (preferably using zinc sulfate concentration with centrifugation because this test is more reliable for detecting Giardia), fecal or rectal scrape cytology, and colonoscopy with biopsy. A great majority of patients with disease localized to the large intestine will be diagnosed correctly if this approach is followed. However, if there is any evidence of systemic signs, such as PU/PD, inappetence, weight loss, or vomiting, in addition to large bowel diarrhea, baseline data, including CBC, biochemical profile, urinalysis, and survey abdominal radiographs, should be obtained. The scope of any further work-up is then expanded based on these results (e.g., panhypoproteinemia suggests that a small intestinal disorder is concurrently present, azotemia and low urine specific gravity indicate renal disease). It is once again emphasized that if there is any possibility that both small and large intestinal disease are present, biopsies of both regions should be performed. All too often, incomplete diagnosis and only partially effective treatment regimens are established if a less than thorough approach is made once the step of intestinal biopsies is reached.