GRASS INGESTION/ COPROPHAGY/PICA
It is not uncommon for dogs and cats to ingest grass and for dogs to demonstrate a tendency toward coprophagy or pica. Occasionally, certain cats may excessively lick materials such as soil, litter, wool, and other items.
Although the tendency to do this may be related to a group of syndromes termed ingestive behavior problems, these conditions may also occur as a result of some type of digestive system disorder. Questions are frequently asked about the significance of these activities, especially grass ingestion and coprophagy. A brief discussion of each problem follows.Grass Ingestion
Many dogs and some cats enjoy eating grass for no proven reason and with no apparent untoward effects. For some it may represent a normal physiologic event. Perhaps these animals simply enjoy “grazing,” or they may be seeking a source of roughage to supply minerals or fiber. If grass ingestion is not associated with any immediate symptoms of a GI disturbance, such as nausea, bloating, or vomiting, its significance is probably minor and there is no need for concern on the part of the owner. Cats that do not get vegetable matter in their diets may have a tendency to eat parts of house plants. This problem can often be successfully eliminated by providing a small flower pot with grass for the cat to eat. For cats that develop an undesirable habit of eating certain house plants, measures such as removal of the plant or aversion taste-smell conditioning with pepper sauce or vinegar often work. Plant ingestion may cause vomiting from irritant or toxic effects, and it should certainly be discouraged if these symptoms develop.
I commonly encounter canine patients that are reported to ingest grass only at times when they seem to be experiencing some type of distress related to the digestive system. The most common of these is nausea, exhibited by such signs as licking of the lips, exaggerated swallowing motions, salivation, and often disinterest in eating food.
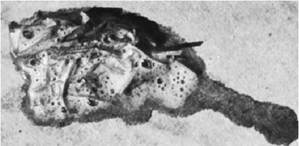
Figure 1-12 Grass and bile fluid vomited by a dog that was demonstrating symptoms of nausea before ingesting the grass.
Frequently the dog, when allowed outside, moves quickly to a grassy area and begins ingesting grass. Shortly thereafter, the grass, usually along with fluid that is often bilious (Figure 1-12),is vomited, and the dog often subjectively appears to feel much better after the stomach has emptied (based on improved appetite and energy). In my experience this is not an uncommon occurrence in dogs with the bilious vomiting syndrome, which is frequently associated with some degree of gastric hypomotility. Dogs with this syndrome that eat grass often do so more in the early morning hours (although it can occur at any time). They most likely awaken from a period of sleep while experiencing nausea, and they tend to pace around until they can gain outdoor access, where they often head directly to a grassy area.
Some large-breed dogs will impulsively eat large quantities of grass in the early stages of a gastric dilatation event. Perhaps grass has some type of soothing property for dogs and cats with esophageal or gastric irritation that can result from any of a number of causes. These may include gastroesophageal reflux, erosive gastritis, superficial irritation from bile reflux, vomiting related to chronic gastritis or inflammatory bowel disease, and others. For many years it has been theorized by laypeople that dogs with GI upset may eat grass because they have a sense that doing so will help them vomit. Dogs that eat grass as a result of a digestive system disorder generally do so only on an intermittent basis that often coincides with their periods of discomfort. I definitely consider this to be a meaningful clinical sign, and I make a point of asking owners whose pets are presented for evaluation of disorders characterized by inappetence, nausea, or vomiting if they ever see their dog eating grass during periods of apparent GI discomfort.
Not uncommonly the answer is yes. In fact, the act of grass ingestion can actually become a valuable monitoring tool for owners, providing an indication that their pet is uncomfortable and in need of some type of treatment.My own Doberman pinscher, which was afflicted with a gastric hypomotility disorder for much of her life, demonstrated very clear signs of nausea with subsequent grass ingestion, followed by vomiting, on days on which I failed to medicate her properly (she was on lifelong twice-daily metoclopramide therapy to improve gastric motility) or to feed her on time. On occasion even when I did administer the medication in a timely manner, she would still exhibit signs of nausea and have a propensity to eat grass. My response, which often seemed to provide relief, was to increase the frequency of metoclopramide to three times a day and to add an H2-receptor antagonist (famotidine) to lower gastric acid levels, both for several days. She rarely showed any interest in eating grass when her GI symptoms were well controlled.
Other veterinarians have recounted stories to me about their own dogs that have had grasseating tendencies. Some have not shown any concurrent GI symptoms such as nausea or vomiting but dramatically decreased or stopped altogether the grass ingestion when they were treated with H2-receptor antagonist therapy on an empirical basis. In some, as soon as this medication was stopped, the grass ingestion behavior was resumed. Ideally these dogs should undergo upper GI endoscopy to examine for evidence of reflux esophagitis, gastritis, bile retention in the stomach, upper small bowel inflammation, and other conditions. One can only speculate that for these particular dogs the ingestion of grass may truly have some type of therapeutic effect. The difficulty for us in working with our patients, of course, is in clearly determining whether or not there is any significant reason for a particular patient to ingest grass, especially when there are no obvious associated symptoms.
Certainly care must be taken not to overinterpret the significance of grass ingestion. Further investigation is needed before any conclusions can be drawn.Coprophagy
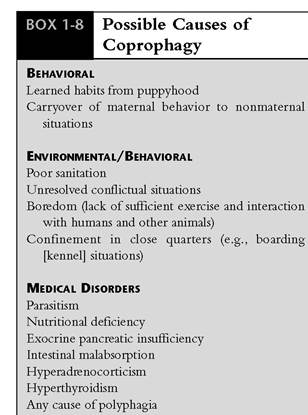
Coprophagy is the ingestion of feces. This is common behavior in some species, most notably rabbits, and in the young of most species. Cats rarely become coprophagic, but to the dismay of many dog owners it is a frequently occurring canine misbehavior. The idea of coprophagy is revolting to most humans, and there is potential for its occurrence to seriously alter an owner's attitude toward his or her dog. Most will try any suggestions offered by their veterinarian, trainer, or any other opinionated person. Some owners, however, come to accept their dog's habit. Many dogs also display a great preference for ingesting cat feces. Potential causes of coprophagy are listed in Box 1-8.
Many theories, none scientifically accepted, about why coprophagy occurs in dogs have been proposed by veterinarians and laypeople. It is adaptive behavior during the first 3 weeks of nursing for the mother to keep the nest free of urine and feces. It is possible that, for some dogs, consuming the feces of the young may predispose them to coprophagy in nonmaternal situations. It is also possible that the habit of coprophagy may be an example of neonety, that is, the retention of juvenile behavior in the adult dog.
Common reasons for coprophagy probably include boredom, lack of attention from an owner, unresolved conflictual situations in the environment, insufficient exercise, consumption of nutritionally incomplete rations, poor hygiene in the environment, and digestive system disorders that result in malabsorption or maldigestion. Bored or fastidious dogs might first begin ingesting their
feces during confinement situations (e.g., cage confinement in a kennel). Coprophagy may then become a habit. Dogs with exocrine pancreatic insufficiency (EPI) may become coprophagic, probably secondary to polyphagia and as a consequence of specific nutritional deficiencies.
In fact, any disorder that causes polyphagia can also potentially cause coprophagy. In addition to malassimilation disorders, other problems that have been reported to be associated with coprophagy include hyperadrenocorticism, intestinal parasitism, and hyperthyroidism; glucocorticoid therapy also appears to be associated with coprophagy.A few significant deleterious consequences are usually associated with coprophagy. The severe halitosis that results is particularly offensive to most owners. Depending on the timing of their activity, dogs may find themselves relegated to areas where they are unable to gain access to the owner. The potential for acquiring parasitic infections from ingesting stools always exists. Bacterial and viral infections can also be transmitted in this way. Occasionally dogs with access to horse manure are presented in acute distress that results from partial or complete intestinal obstruction. Surgery is sometimes necessary to relieve these impactions.
The diagnostic evaluation for the problem of coprophagy starts with obtaining a thorough history. A differential diagnosis should be made regarding the likelihood of the presence of a significant medical problem versus environmental problems or primary behavior tendencies. The quality of the diet should be assessed. If a poor quality diet is being fed, it may simply be enough to change to a higher quality ration, preferably one with a high digestibility ratio. Dogs that are fed only one meal per day may have a lesser tendency toward coprophagy if food is provided two to three times a day.
Questioning regarding the environment includes information about hygiene practices, level of daily exercise that patient gets, amount of interaction with humans or other animals, and whether there are any known stresses or conflicts that the patient undergoes in its environment. Delayed cleanup and disposal of stools can contribute to the initiation and maintenance of a habit of coprophagy.
Efforts must be made by the owner to remove stools from the environment as quickly as possible. Boredom can be a contributing factor to coprophagy. Dogs that spend much of their time alone all day, especially outdoors, may eventually get into the habit of eating their stools. Extra exercise and human interaction every morning and evening, which includes walks and periods of play with the owner, as well as providing another animal with which to interact, may be of some help in these situations. Proffering the dog fresh rawhides on a daily basis may help lessen the tendency for coprophagy.If coprophagy involves ingestion of cat feces from litter boxes, the only realistic methods of control include placing the litter boxes in areas where dogs are unable to gain access, using covered litter containers, and cleaning the litter as frequently as possible.
If the history suggests that there may be a medical disorder present, appropriate diagnostic evaluation should be undertaken to identify or rule out any potential problems. Treatment is then directed toward whatever problem is identified. Examinations for intestinal parasites should be done routinely. If there is any possibility of EPI, a trypsin-like immunoreactivity (TLI) assay should be run. It should be noted that some dogs with EPI only infrequently have diarrhea. The canine TLI test is readily available at many commercial labs and is highly diagnostic for EPI. Treatment includes pancreatic enzyme replacement therapy and dietary management (mild to moderate fat restriction and low fiber content). Coprophagic tendencies often stop in dogs with EPI once appropriate therapy is instituted.
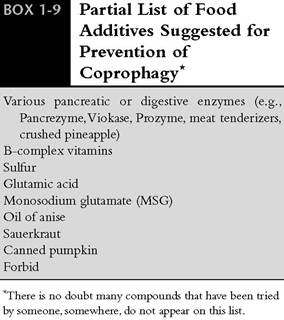
Myriad compounds that can be added to the food in an attempt to decrease or alleviate coprophagic behavior have been recommended and tried over the years. These compounds include various types of digestive enzymes and vitamins used to improve digestion and subsequent absorption of nutrients, or chemicals that are added to the food to make stools that are subsequently passed less desirable to eat for copro- phagic dogs by creating an offensive taste. In my experience this approach unfortunately rarely works. However, these ideas should be discussed with owners who are willing to try anything to curb their dog's habit of coprophagy. A list of various enzymes or chemicals that have been recommended by veterinarians, breeders, and behavior specialists appears in Box 1-9.
Once the habit of coprophagy is started, it can be very difficult to break. Treatment may require retraining the patient. Use of a muzzle to prevent prehension of stool may be a useful starting point in the retraining process. Moreover, several recently
proposed behavior modification techniques, used alone or in combination, have shown promise in fairly consistently stopping coprophagic tendencies in dogs whose problem has been found to be behavioral rather than medical. First, an owner may condition a dog to expect a treat immediately after stooling. In this fashion its expectation of a delicious food treat may inhibit the tendency to feed on stools. Second, a way may be found to punish the activity or make the activity aversive. One method is to inject the commercial product Bitter Apple into the stool. Simply spraying this product on the surface of the stool will not be likely to have any lasting effect because the dog will shy away before it touches the stool. The element of surprise is lost if this is done. Biting into stool that is impregnated with Bitter Apple will often cause a very significant aversive sensation. Dose depends on the size of the stool, but a general range of 1 to 3 ml is suggested. This method may also help prevent a dog from ingesting cat feces. An alternative would be to inject the feces with the emetic drug apomorphine. Ingestion of feces followed shortly by a strong sensation of nausea and then vomiting may suffice to cause a strong aversion to the stool.
As a last resort, owners who strongly desire to stop coprophagic behavior can try remote punishment with a shock collar. Remote punishment is applied the moment the dog begins to explore or prehend stool. Behavior modification with shock collars has been reported to be very effective. It must be noted that this method of treatment should be carefully discussed with any owner who expresses interest in trying it. The owner's ethical
concerns and other issues surrounding the application of this procedure need to be taken into consideration. For some this form of treatment may be unacceptable. The reader should consult the references at the end of the chapter for an overview of using this kind of treatment to solve behavioral problems.
Pica
Pica is defined as a craving for and ingestion of unnatural articles of food. Dogs may eat dirt (geophagy), cloth, carpet, rocks, sticks, cat litter, or other materials or may show a distinct interest in licking carpet or concrete. Cats may eat soil, grass, or even cat litter. Anemic cats sometimes lick soil, litter, walls, or rusty objects. Wool sucking is an abnormal behavior disorder known to occur in Siamese, part-Siamese, and Burmese cats. Cats with this tendency may actually destroy woolen articles by sucking or chewing on them.
Nutritional deficiencies should be corrected if they exist. The diagnostic approach is similar to that followed for coprophagy. Dietary and environmental factors should be investigated. Occasionally, geophagic animals are found to be iron deficient. Dogs that lick or chew on foreign objects may have acute or chronic vomiting that may be related to the presence of a gastric or intestinal foreign body. I have seen dogs with large clumps of carpet fibers that probably took weeks to months to build up before endoscopic retrieval or gastrotomy became necessary to remove the material.
Most of the time, animals with pica have a behavioral tendency rather than a true medical disorder. Treatment usually involves preventing access, if at all possible, to favored objects or limiting access to one to two items. Taste aversion methods can also be tried. Thyroid hormone supplementation works well in some wool-sucking cats.