DYSPHAGIA
Dysphagia is defined as difficult or painful swallowing. It may be due to obstruction, motility disturbance, or pain. Although dysphagia most commonly indicates a disorder involving the oral cavity or pharynx, esophageal disorders can cause this clinical sign as well.
Oropharyngeal dysphagia can generally be differentiated from esophageal dysphagia on the basis of history. Characteristic signs of oropharyngeal disorders include acute gagging, exaggerated swallowing movements, and increased frequency of swallowing. Food is frequently dropped from the mouth within seconds of prehension. In contrast, patients with esophageal dysphagia do not exhibit exaggerated swallowing motions and food is not dropped from the mouth. If clinical signs are acute and persistent or progressive, a morphologic lesion (e.g., foreign body, mass, inflammation) should be suspected. Intermittent occurrence of clinical signs is usually consistent with a motility disturbance.The causes of oropharyngeal dysphagia are listed in Box 1-2.A careful review of the history and observation of the patient as it eats will confirm the presence of dysphagia, identify its primary anatomic location (oropharyngeal in most cases), and help determine a diagnostic plan. Typically patients with oropharyngeal dysphagia eat readily but have trouble swallowing the food normally. If the tongue is not functioning normally, there may be problems with prehension and mastication as well. Affected patients may extend, ventroflex, or throw their heads back during exaggerated efforts to swallow. Additional signs that may be observed include salivation (related to inability to swallow and/or secondary to pain), nasal discharge secondary to passage of liquid and food into the nasopharynx and nasal cavity, and coughing resulting from aspiration of food retained in the phar- ynx.Weight loss or failure to grow may also occur in some cases.
The initial step in diagnosis is to differentiate among oral, pharyngeal, and cricopharyngeal dysphagias. Signalment, clinical course (i.e., acute and persistent versus gradual onset), and physical findings are reviewed first. Clinical signs associated with cricopharyngeal achalasia are generally initially observed at the time of weaning onto solid food and, if not this early, almost always by 1 year of age. Dogs with congenitally short or cleft palate will also exhibit signs at a very young age. Young to middle-age patients are most prone to
BOX 1-2
Causes of Oropharyngeal Dysphagia
Oral Pain
Stomatitis/glossitis/pharyngitis
Feline viral rhinotracheitis, calcivirus
FeLV infection
FIV infection
Immune-mediated disease (e.g.,pemphigus, SLE) Foreign body
Uremic glossitis
Sepsis
Ingestion of caustic agents (acids, alkalis, thallium) Tooth-related problems
Periodontitis
Tooth root abscess
Fractured teeth
Fractured bones
Osteomyelitis
Electric cord burns
Retrobulbar abscess
Oral Mass
Neoplasia (benign or malignant)
Squamous cell carcinoma
Fibrosarcoma
Melanoma
Eosinophilic granuloma
Foreign body obstruction (oral, pharyngeal, nasopharyngeal, proximal esophageal)
Sialocele
Neuromuscular Disease
Myasthenia gravis (focal or generalized) Acute polyradiculoneuritis
Tick paralysis
Botulism
Oral, pharyngeal, cricopharyngeal dysfunction Polymyositis
Temporomandibular joint disease
Neurologic Disorders
Rabies
Trigeminal paralysis
Neuropathies of cranial nerves VII, IX, X, XII
CNS lesions (brainstem lesions)
FeLV, Feline leukemia virus; FIV, feline immunodeficiency virus; SLE, systemic lupus erythematosus; CNS, central nervous system.
lodgment of foreign bodies in the mouth and pharynx and accidental ingestion of caustic materials (such as petroleum products or alkalis), and signs of dysphagia are acute and persistent until definitive treatment is administered.
Older dogs with an insidious onset of clinical signs are more likely to be afflicted with neoplasia (e.g., glossal neoplasia, pharyngeal tumors such as squamous cell carcinoma, fibrosarcoma, melanoma, tonsillar carcinoma, retropharyngeal mass causing compres- sion).Weight loss and reluctance to eat are generally present in chronic cases. Presence of systemic signs, such as weakness that worsens with exercise, with or without cough and dyspnea, suggests myasthenia gravis. Signs of myasthenia gravis may be limited to pharyngeal dysfunction. Weakness may also be caused by polymyositis or central nervous system disease. Dysphagia occurring in conjunction with dementia suggests cerebral disease as the underlying problem. Rabies vaccination history and potential for exposure (environment) must always be determined early in the evaluation of any patient with dysphagia.Thorough physical examination will successfully identify the cause of dysphagia in some cases. Physical signs may also alert the clinician to the presence of any significant complications (e.g., pneumonia) and help determine specific tests that should be done to establish a definitive diagnosis. Physical examination should include a thorough evaluation of the head (temporal muscle atrophy, pain associated with muscles of mastication, ocular areas for inflammation or proptosis of one of the eyes to suggest retrobulbar mass or cellulitis), oral cavity, external pharyngeal and cervical soft tissue areas for any mass effect, lymphadenopathy, or draining tract; recognition of any pain related to opening of the mouth (e.g., masticatory muscle myositis, retrobulbar inflammation, temporomandibular joint disease); and a neurologic examination. Specific neurologic tests include evaluation of cranial nerves IX (glossopharyngeal) and X (vagus) by checking the swallow and gag reflexes, respectively, evaluation of cranial nerve XII (hypoglossal) via observation and palpation of the tongue, and evaluation of gait and strength.
Focal lesions of the medulla oblongata and diffuse neuromuscular disease may cause ataxia, conscious proprioception deficits, and limb weakness. Patients that exhibit any evidence of systemic signs (e.g., weakness, polyuria/polydypsia [PU/PD], muscle pain) in conjunction with dysphagia should initially be evaluated by complete blood count (CBC) (infection, inflammation, anemia of chronic disease), biochemical profile (including creatine phosphokinase [CPK] for polymyositis), and urinalysis. For example, a biochemical profile and urinalysis may confirm that lingual ulceration or necrosis is due to uremia.Sedation or general anesthesia is often required for thorough examination of the oral cavity, pharynx, and larynx. The dental arcade, tongue (including frenulum area), palate, tonsils, and tonsillar crypts should be carefully evaluated for the presence of inflammation, mass, or foreign body. Biopsies of masses should be deep to determine diagnosis and prognosis accurately. A superficial biopsy may fail to harvest neoplastic cells from a cancerous mass because the changes at the surface may be limited to inflammation and necrosis. Electrocautery can be used to control postbiopsy hemorrhage. It is important to evaluate the nasopharynx (for significant inflammation, foreign body, mass) and the proximal esophagus as well. On occasion I have found foreign bodies such as long blades of grass, peanut shells, or small needles lodged in the nasopharynx and not extending caudal to the free border of the soft palate (i.e., not readily visible on initial oral examination). Use of a flexible endoscope that is small enough to allow retroflexion over the soft palate greatly facilitates examination of the nasopharynx (Figure 1-1). Survey pharyngeal radiographs may be indicated as part of the preliminary work-up if history or physical examination suggests that a mass, foreign body, or injury (e.g., hyoid bone fracture) may be present. Contrast radiographic studies with fluoroscopy while observing swallowing of both liquids and food are required for differentiation of pharyngeal and cricopharyngeal dysphagia.
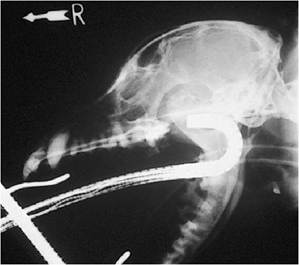
Figure 1-1 Lateral skull radiograph of a dog, demonstrating correct placement of a flexible endoscope for posterior rhinoscopy. Examination of the nasopharynx and choanae is facilitated by the use of a scope with a tip deflection capability of 180 degrees or more.
An acetylcholine receptor antibody titer test (see Chapter 4) should be run if there is any possibility of myasthenia gravis (signs of focal myasthenia gravis may be limited to pharyngeal dysfunction and regurgitation). A Tensilon (edrophonium chloride) test could also be done, but the clinician should observe carefully for and be prepared to treat cholinergic overstimulation if it occurs. If central nervous system disease is suspected, testing may include cerebrospinal fluid analysis, nuclear scintigraphy, and/or computed axial tomography or magnetic resonance imaging (MRI).