ENDOSCOPY
Endoscopy is one of the best and yet most fundamental methods of examining the gastrointestinal (GI) tract. It is now a well-established procedure in veterinary medicine. The opportunity to directly examine and obtain tissue samples from the esophagus, stomach, and intestinal tract in a minimally invasive way has greatly altered the clinical approach to diagnosis and has made significantly more accurate the treatment of disorders of the digestive system.
Despite the tremendous diagnostic advantages that endoscopy offers, it is still best used by the clinician as an adjunctive procedure in the evaluation of GI disease.A thorough review of the history, complete physical examination, and selected laboratory and radiographic examinations as appropriate for each individual case are still important for thorough patient evaluation.When used judiciously, endoscopy offers a valuable alternative to exploratory surgery for direct examination of tissues, procurement of biopsy samples, and retrieval of foreign bodies.Selection of an Endoscope
Endoscopic equipment is no longer considered a luxury that only large referral centers or veterinarians practicing in affluent areas can justify purchasing. An endoscope is one of the most versatile and diagnostically valuable pieces of equipment that a veterinary practice can have in its armamentarium. The selection of equipment to be used for performing endoscopy often depends on its versatility of application, durability, and expense. Many practices have been able to financially justify the purchase of high-quality endoscopic equipment. When consideration is given to the purchase of an endoscope, the most important factors to be reviewed should be the probable frequency of usage and versatility of the instrument rather than the purchase price.
Other important considerations are the quality of the optical system and ease of operating the endoscope.
Significant differences exist, so equipment purchases should be made carefully! Too frequently veterinarians rank a lower purchase price as one of the most important factors. This can be a significant mistake because even the most skilled endoscopist may find performing a complete examination and making the correct diagnosis difficult while using an endoscope of poor quality.My recommendation to veterinarians interested in purchasing their first endoscope is to buy a single high-quality endoscope that may be used for a variety of procedures (e.g., esophagogastroduodenoscopy, colonoscopy, bronchoscopy, and nasopharyngoscopy in dogs) in cats and small dogs, as well as in large dogs. A pediatric endoscope with four-way tip deflection capability meets these criteria well (Figure 3-1).Endoscopes
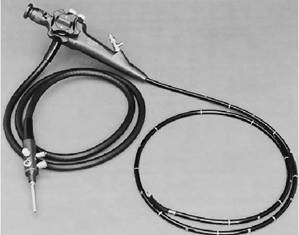
Figure 3-1 Storz pediatric veterinary endoscope. Specifications include 8.5mm-diameter insertion tube, 100-degrees forward-viewing field of view, 150-cm working length, 2.5mm-diameter accessory channel, and four-way tip deflection.
with two-way distal tip deflection capability have very limited use in GI endoscopy. Most of these endoscopes are relatively short (50 to 80 cm) and are intended to be used primarily as bronchoscopes. It is somewhat more difficult to maneuver an endoscope that is limited to two-way distal deflection through the antral canal, pylorus, and duodenum. The preferred insertion tube diameter should range from 7.8 to 9 mm. The major limitation of a large insertion tube (diameter of 9.8 mm or greater) is that there is more difficulty in passing it through the pyloric canal to the duodenum in cats and small dogs. This is an important consideration because an effort should be made to examine the duodenum in all cases in which vomiting, diarrhea, or weight loss is part of the clinical presentation. Larger endoscopes can be used quite effectively in many animal patients, but there are inherent difficulties in performing a complete examination in very small animals.
This becomes an important factor for any urban practice in which many cats and small dogs are seen. A standard working length of 100 cm or more is adequate for performing a thorough examination in cats and most dogs. Unfortunately 100-cm endoscopes are occasionally not long enough to reach the duodenum in large breed dogs. Newer, more versatile pediatric veterinary endoscopes with an insertion tube length of 140 to 150 cm are now available. With these longer endoscopes it is possible to easily reach the duodenum in even the largest dogs.In addition to the endoscope, other equipment that is needed includes a light source, a suction pump (any standard suction pump system can be used by attaching the tubing to the suction connector port on the endoscope), a biopsy instrument, and foreign body graspers. A number of different light source models are available that have a wide variety of features. There are two basic types of light sources. Smaller, lower-priced units that use a low-wattage (e.g., 150 watts) halogen lamp are quite adequate for most veterinary applications. Xenon lamps produce a brighter and whiter light than halogen lamps. Xenon light sources provide the best illumination for video documentation. If a light source is to be used for both flexible and rigid endoscopic applications, xenon is clearly preferred. Video cameras that can be attached to the eyepiece of the endoscope and high-resolution monitors are also available (Figure 3-2). Use of this equipment allows simultaneous viewing by any number of observers.

Figure 3-2 High -resolution endoscopic video camera and monitor. The camera (top) is attached to the eyepiece of the endoscope. The endoscopist performs the procedure while watching the image on the video monitor. The camera can be fully immersed and features automatic exposure control.
Learning Endoscopic Techniques Once the decision is made to purchase an endoscope, whether new or used, every effort should be made to become proficient in its use.
This is accomplished through attending one or several formal wet lab courses and then practicing the basic skills of maneuvering an endoscope and procuring biopsy samples. If proper skills of maneuvering and observation are not developed, even the most sophisticated endoscopes are of little value. Frustration resulting from unfamiliarity with proper instrument handling and unavailability of necessary ancillary equipment too often leads to disuse.Indications for Gastrointestinal Endoscopy
During its early development, fiberoptic endoscopy was used primarily as an adjunct to other diagnostic methods, especially barium contrast x-ray examinations. However, in recent years many veterinary gastroenterologists have come to regard endoscopy as one of the most sensitive methods of evaluating GI tract symptoms. This has resulted in a substantial increase in the use of endoscopy in many veterinary hospitals, corresponding with a decrease in the number of barium series that are performed. This trend is expected to continue as more veterinarians become familiar with the distinct diagnostic advantages of endoscopy.
Most of the commonly encountered disorders of the GI tract involve either the mucosa of the organ in question or disrupted mucosal anatomy. Endoscopy offers the clear advantage of complete mucosal examination of the esophagus, stomach, descending duodenum (in cats and small dogs, the ascending duodenum and sometimes the proximal jejunum as well), terminal ileum in most dogs 10 lb or larger, and colon. Endoscopic biopsies provide rapid assessment and evaluation of many disorders. In addition, endoscopy plays an important therapeutic role in foreign body removal, guided bougienage or balloon dilation of esophageal and colonic strictures, and placement of gastric feeding tubes. Well-established indications for endoscopy are listed in Table 3-1. Disorders that can be reliably diagnosed via endoscopy are listed in Table 3-2.
Diagnosis of Esophageal Abnormalities
Esophagoscopy should be considered for any patient with signs of esophageal disease.
The decision whether or not to actually perform an endoscopic examination of the esophagus is based on clinical impression and a review of any indicated laboratory tests and radiographic studies. Common signs of esophageal disease include regurgitation, dysphagia, excessive salivation, and change in appetite, which may be either increased or decreased.In the esophagus, as elsewhere in the GI tract, endoscopy is most effective in diagnosis of disorders that affect the mucosa. Hence, it can be expected that diagnosis of inflammatory, neoplastic, and obstructive lesions (e.g., stricture, foreign body) will be relatively precise. Whereas survey or contrast radiography is useful for identifying an obstructive lesion, esophagoscopy provides a means of obtaining a definitive diagnosis and in some cases offers important therapeutic options. Esophageal foreign bodies (e.g., fishhooks, bones) can often be successfully removed using graspers that are passed through or alongside the endoscope. Any erosive damage to the esophagus can be assessed after a foreign body has been removed.
TABLE 3-1
Potential Indications for Gastrointestinal Endoscopy
Initial Follow-up
| Regurgitation | Repeat esophageal stricture |
| Dysphagia | balloon dilation or bougienage |
| Retching | Follow-up biopsies in patients |
| Unexplained | with moderate to severe |
| salivation | gastritis, inflammatory bowel |
| Unexplained | disease, colitis, neoplasia (i.e., |
| nausea | assess progression of disease, |
| Unexplained | efficacy of therapy) |
| inappetence | |
| Vomiting | |
| Hematemesis | |
| Diarrhea | Serial assessment during ulcer |
| healing | |
| Melena | |
| Dyschezia | Serial assessment of mucosal |
| Constipation | healing and examination for |
| Fecal | possible stricture |
| incontinence | formation following |
| Foreign body | esophageal mucosal damage |
| retrieval | from a foreign body |
| Feeding tube | |
| placement | |
| Guided stricture | |
| dilation |
Modified from Tams TR: Endoscopy.
In Kirk RW Bonagura JD, eds: Current veterinary therapy X. Philadelphia, 1989,WB Saunders.
Bougienage or balloon dilation procedures to dilate esophageal strictures are most safely performed under endoscopic visualization. Esophageal tumors can be diagnosed by guided biopsy. In human medicine, endoscopic laser therapy has been successfully used for ablation of neoplastic tissue. This is a palliative measure undertaken in esophageal cancer patients primarily to relieve luminal obstruction and hemorrhage.
Unexplained salivation is an important indication for esophagoscopy in animals because, in some cases of esophagitis or neoplasia, salivation may be the only prominent sign or one of several subtle signs that is exhibited early in the course of the disorder.
The diagnosis of reflux esophagitis cannot be made consistently solely on the basis of gross examination because in some cases changes are limited to microscopic inflammation. Certain endoscopic “clues” may be observed by an experienced endoscopist, however, that will suggest the
Gastrointestinal Disorders Amenable to Diagnosis by Endoscopy
TABLE 3-2
| Site of Disorder | Type of Disorder | |||
| Inflammatory | Infectious/Parasitic | Anatomic | Neoplastic | |
| Esophagus | Esophagitis Chemical injuries (acid, alkali) | Strictures Foreign bodies Hiatal hernia Diverticula Megaesophagus (endoscopy rarely necessary for diagnosis) | Squamous cell carcinoma Adenocarcinoma Metastases Others | |
| Stomach | Gastritis (e.g., lymphocytic- plasmacytic, eosinophilic, histiocytic) Chemical injuries Ulcer—benign and malignant | Physaloptera | Foreign bodies Hypertrophic gastropathies Polyps Extraluminal compressive masses | Lymphoma Adenocarcinoma Others |
| Duodenum | Inflammatory bowel disease | Giardiasis Histoplasmosis | Polyps (rare) | Lymphoma Adenocarcinoma Others |
| Colon | bgcolor=white>ColitisTrichuriasis Cestodiasis Protozoal infections (examine mucosal brushings) Histoplasmosis | Polyps Strictures Cecal inversion Ileocolic intussusception | Lymphoma Adenocarcinoma Others | |
Modified from Tams TR: Endoscopy. In Kirk RW, Bonagura JD, eds: Current veterinary therapy X. Philadelphia, 1989,WB Saunders.
likelihood of reflux esophagitis (e.g., distal esophageal erythema, gastroesophageal sphincter dilation, pooling of fluid in the distal esophagus). Monitoring distal esophageal pH with a probe and performing a suction biopsy of the distal esophageal mucosa provide a more sensitive means of diagnosis of reflux esophagitis than visualization alone.
Esophageal motility disorders in which there is not easily detected radiographic evidence of marked esophageal dilation are best recognized by esophageal fluoroscopy and manometry studies. Endoscopic examination of the esophagus reveals certain appearances, however, that may suggest the possibility of a motor abnormality, and, in hospitals where fluoroscopy equipment is not available, esophagoscopy can still be useful as a diagnostic aid. Often a diagnosis of clinically significant decreased lower esophageal sphincter pressure can be inferred from the presence of grossly evident esophagitis lesions and variable degrees of dilation of the gastroesophageal junction.
In most patients with megaesophagus, endoscopic examination is not necessary for diagnosis and is rarely of benefit in determining a cause of the disorder. Megaesophagus is a specific syndrome characterized by generalized esophageal dilation and hypoperistalsis, and it is differentiated from other causes of esophageal dilation such as esophageal foreign body, vascular ring anomaly or other stricture disorders, and neoplasia. If pneumonia is ruled out in a megaesophagus patient that is anorexic, esophagoscopy may be indicated to examine for esophagitis.
Diagnosis of Gastric Abnormalities
Indications for gastroscopy include signs referable to gastric diseases, including nausea, salivation, vomiting, hematemesis, melena, and anorexia. Gastroscopy mainly defines abnormalities of the gastric mucosa, but it may also reveal distortion of the stomach's normal anatomic relationships by displacement or extrinsic compression as a result of a mass or enlargement of an adjacent organ structure. With proper technique the entire mucosal surface of the stomach and the antral- pyloric canal can be examined. The most common disorders diagnosed include chronic gastritis, gastric foreign bodies, and gastric motility disorders (Figure 3-3). Ulcers, neoplasia, and hypertrophic gastropathy can be readily diagnosed but are less commonly found (Figure 3-4). Special therapeutic considerations include foreign body
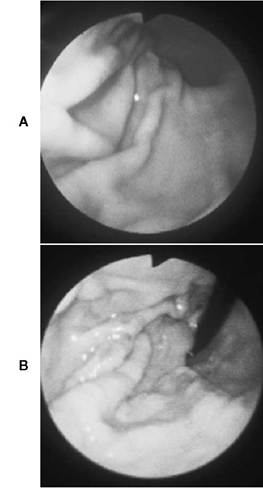
FIGURE 3-3 Endoscopic photos from feline stomach. A, Normal stomach of a cat, showing the midgastric and distal gastric body. Rugal folds are clearly in view, and the mucosa is smooth. B, Chronic gastritis in a cat. This is a retroversion view of the proximal stomach, with the endoscope in a curved position looking back on itself. The gastric mucosa is irregular throughout, and there are erosive changes on the rugal fold in the right field of view. Biopsies confirmed a diagnosis of chronic moderate lymphocytic-plasmacytic gastritis.
removal and endoscopy-guided percutaneous gastrostomy tube placement. Gastrostomy tube placement is a quick and simple procedure (see Chapter 12) and provides an excellent means of temporarily feeding an anorectic or debilitated patient.
In patients with chronic upper GI disorders, gastroscopy should be performed in conjunction with esophagoscopy and duodenoscopy. Important diagnostic clues may be evident in any or all of these areas during the course of an examination. Follow-up gastroscopy is a valuable aid in monitoring response to therapy in chronic gastritis and ulcer patients. Follow-up biopsies are especially important in patients with chronic severe histiocytic and granulomatous gastritis, chronic fibrosing gastritis, and gastric lymphoma. Important information that is useful in determining treatment protocol adjustments can often be obtained.
In evaluating a patient with signs suggestive of a gastric disorder, gastric mucosal biopsy samples should be obtained even if gross lesions are not present. It is common for a patient with chronic gastritis to have lesions identifiable only on microscopic examination. Different classifications of gastritis (e.g., lymphocytic-plasmacytic, eosinophilic, histiocytic) and degrees of involvement (e.g., mild, moderate, severe) can be determined from mucosal biopsy samples; these findings are extremely important in determining specific therapeutic regimens. If gross lesions are identified (e.g., localized hyperemic changes, nodules, or masses), forceps biopsies should be obtained from these areas, as well as from several normal areas. Six to eight biopsy samples are obtained from different areas of the gastric body and fundus if the stomach is grossly normal. Biopsy samples are best obtained from the surface of a gastric fold. The size of the tissue samples obtained may be inadequate if the stomach is too distended with air because the folds become too flattened. When the endoscope is first advanced to the stomach during the course of an examination, air is insufflated to distend the gastric walls so that thorough mucosal evaluation is enhanced. Suctioning some of the air out just before taking biopsy samples greatly increases the gastric fold surface area from which samples can be obtained. It is more difficult to obtain a tissue sample of adequate size from the gastric antrum than it is from other parts of the body unless there is hypertrophy or discrete raised or cratered lesions.
Clues that a gastric motility disorder may be present include pooling of bile or gastric fluid or finding undigested food in the stomach of a patient
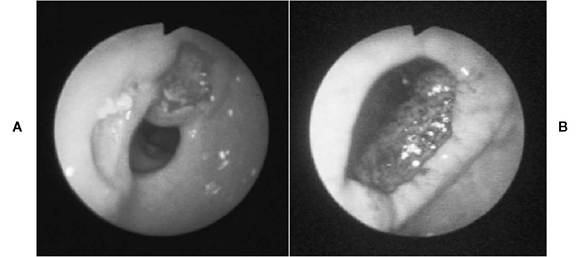
Figure 3-4 Gastric ulcers. A, Two peripyloric ulcers in a 14-year-old dog that was receiving nonsteroidal antiinflammatory drug (NSAID) therapy for severe osteoarthritis. The pyloric orifice (center) is open, and ulcers are seen to the left and above the pylorus. The dog had intermittent vomiting and inappetence. B, Large perforated gastric ulcer in an 8-year-old chow that had received naproxen (an NSAID) once daily for 7 days. On the sixth day vomiting and inappetence were first noted by the owner. Naproxen was discontinued on the seventh day, but the clinical signs persisted. Nine days after naproxen was discontinued, the dog was presented for endoscopy. The dog was bright and alert. The complete blood count (CBC) and biochemical profile were normal (packed cell volume [PCV] = 48%). On advancement into the gastric antrum the endoscope revealed a very deep ulcer with a thick rim (entire upper left quadrant). The pyloric orifice is at the lower left (7 o’clock position). The meshlike tissue seen through the ulcer crater is omentum (there was a complete omental seal). The ulcer area was subsequently resected surgically. (From Tams TR: Gastroscopy. In Tams TR, ed: Small animal endoscopy, St. Louis, 1999, Mosby.)
that has been fasted 8 to 10 hours or more. The stomach normally empties within 7 to 10 hours after a meal. There is often mucosal hyperemia caused by superficial irritation from bile, but, despite this gross abnormality, gastric biopsies in idiopathic gastric motility disorders are usually normal.
Because biopsy samples obtained from some masses with standard biopsy forceps are relatively small, sufficient tissue for definitive diagnosis is sometimes not obtained. Several biopsy samples from the same site of a mass should be taken, each time extending the biopsy forceps more deeply into the tissue (Figure 3-5). If tissue from only the surface of a neoplastic mass is obtained, a mistaken diagnosis of granulomatous or fibrous disease may be made. Samples from ulcerative lesions are best taken by grasping the wall or the junction of the wall and the gastric mucosa. Gastric polyps are reliably diagnosed on endoscopic biopsy in dogs and cats.
A major shortcoming of gastroscopy is that neoplastic diseases involving only the serosa or deep layers of the gastric wall cannot be identified or definitively diagnosed on mucosal biopsy. This pattern of tissue involvement is not commonly encountered, however. If endoscopic findings do not correlate with clinical signs, or if there is a poor response to therapy, exploratory surgery should be recommended.
Diagnosis of Duodenal Abnormalities
With a flexible pediatric endoscope (9-mm diameter or less), the duodenum can be directly examined in most cats and dogs. An endoscope with a diameter of 8.5 to 9 mm can consistently be advanced to the duodenum in cats and dogs weighing as little as 3 to 4 lb by an experienced endoscopist. The distal duodenum or proximal jejunum can often be reached in cats and small dogs (Figure 3-6). Certain portions of the duodenum, including the area immediately beyond the pylorus and the medial wall of the descending segment, are sometimes difficult to view other than tangentially, especially as the endoscope is initially advanced through this area. In small patients (especially cats) care must be taken not to be too forceful in advancing the endoscope through areas where there is increased resistance. It is possible to perforate the duodenum if too much force is applied in tight areas.
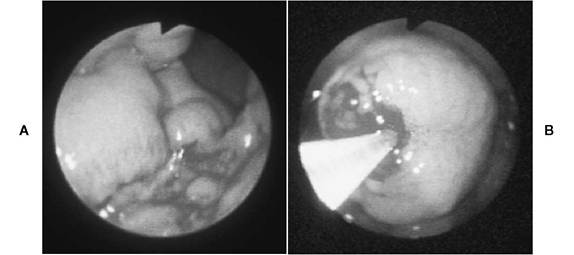
Figure 3-5 Gastric adenocarcinoma in a dog with chronic vomiting, weight loss, and recent anorexia. A, Marked proliferative changes in the lower gastric body, with complete loss of the normal rugal architecture. B, Close-up view of a mass in the midgastric body. The mass was rigid and had a very dense wall (suggestive of neoplasia). Masses such as this one should be biopsied as deeply as possible. If only superficial tissue is obtained, the endoscopist may fail to retrieve neoplastic cells. The first four attempts to biopsy the mass yielded only very small tissue samples, but on the fifth attempt the biopsy instrument advanced inside the mass. A number of large tissue samples were then obtained. (From Tams TR: Gastroscopy. In Tams TR, ed: Small animal endoscopy, St. Louis, 1999, Mosby.)

Figure 3-6 A, Grossly normal duodenum in a dog. B, Small intestine biopsy technique. Endoscopic forceps have been advanced into the duodenal mucosa.
Clinical signs of small intestinal disease include vomiting, diarrhea, melena, change in appetite, and weight loss. By far the greatest value of duo- denoscopy is its capability of definitively diagnosing inflammatory small bowel disorders via biopsy. In fact, recognition that inflammatory bowel disease commonly occurs in dogs and cats became increasingly apparent as patients with various patterns of GI symptomatology began to be evaluated more thoroughly with endoscopic examination and biopsy. Frequently the only major sign in patients with inflammatory bowel disease is vomiting. If only gastric biopsies are performed in these patients, the diagnosis may be missed. In inflammatory disease the small bowel mucosa may appear normal or it may have varying degrees of irregularity, fissures, or follicular-like changes.
Endoscopy offers an alternative approach to obtaining small bowel biopsy samples in cases of protein-losing enteropathy when there is concern that full-thickness surgical biopsy sites may heal slowly. This is an especially important consideration in patients with a total protein level less than 3.5 g/dl. Multiple biopsy samples can be safely obtained using endoscopic biopsy forceps. In addition, the hospital stay is significantly shortened when endoscopy rather than surgery is performed, making this procedure more cost effective. The most common causes of protein-losing enteropathy in dogs are inflammatory bowel disease (by far the most common), lymphoma, and lymphangiectasia. Lymphangiectasia, a disorder of the intestinal lymphatics that results in malabsorption, has a characteristic histologic appearance, and in some cases pronounced gross changes can be seen at endoscopic examination. Often there is a characteristic patchy milky white appearance of the mucosa. In some patients, however, gross changes may be noted only at exploratory laparotomy. Occasionally the diagnosis will be missed if only the descending duodenum is examined and sampled. I have found this to be more of a problem in rottweilers than in other breeds.
Frequently biopsies reveal only mild lymphocytic-plasmacytic enteritis. In dogs that are markedly hypoproteinemic, as is often the case in those with lymphangiectasia, this degree of histologic change is not significant enough to substantiate a diagnosis of inflammatory bowel disease as the primary cause of the hypoproteinemia. Also, lymphangiectasia is often associated with mild lymphocytic-plasmacytic infiltrates in addition to its characteristic lesion of dilated lacteals. Therefore the clinician needs to be aware that enteroscopy limited to the upper small bowel may not establish the definitive diagnosis in some patients with lymphangiectasia. It is strongly recommended that both duodenoscopy and ileoscopy be performed in patients with chronic small bowel diarrhea, especially when hypoproteinemia is present. This approach provides the greatest opportunity for making the correct diagnosis when endoscopy rather than surgery is done to obtain biopsy samples.
Intestinal parasites (generally ascarids) are occasionally encountered on direct examination of the upper small intestine. These parasites can easily be snared with biopsy forceps or foreign body graspers and pulled up through the accessory channel. As is always done during endoscopy procedures, biopsy samples are still obtained even if parasites are observed because the parasites could either represent an additional and unrelated problem regarding the primary disorder or might be a primary causative factor of the clinical signs. During duodenoscopy, saline lavage can be performed through polyethylene tubing advanced through the accessory channel of the endoscope in an effort to retrieve Giardia trophozoites. Direct smears of the aspirates should be examined within 20 minutes of collection with light microscopy at ?100 and ?400.Although endoscopy-guided duodenal lavage has been considered a very good test for diagnosing occult giardiasis, the availability of the fecal enzyme-linked immunosorbent assay (ELISA) for detecting Giardia-specific antigen, a very sensitive and practical test, now precludes the need for duodenal lavage in most diagnostically elusive cases of giardiasis.
Neoplasms that involve the small bowel mucosa can be reliably diagnosed on biopsy if a large enough sample of representative tissue is obtained. Any masses that are found should be sampled as deeply as possible. Lymphoma is the most common type of intestinal neoplasia in dogs and cats. GI lymphomas are believed to be less common in dogs than in cats. The diffuse type of lymphoma is the most amenable to diagnosis by endoscopy. Focal areas of lymphoma in the jejunum or proximal ileum may be missed because of insufficient endoscope length (most cases of GI lymphoma in dogs and cats involve diffuse rather than focal neoplastic infiltrates). Also, if lymphoma involvement is primarily in deeper muscle layers of the intestinal wall, mucosal biopsy samples as obtained with endoscopy forceps may not be deep enough to procure representative tissue. However, this problem is minimized by using proper instrumentation and technique and by routinely obtaining multiple samples (8 to 12) from the duodenum and, whenever possible, the ileum.
When lymphoma is present but not definitively diagnosed on the tissue submitted for examination, the mucosal tissue that is obtained is rarely normal. Usually moderate to severe lymphocytic- plasmacytic inflammatory infiltrates are present over or adjacent to neoplastic foci. A positive biopsy finding such as this may give the clinician false assurance that a definitive diagnosis has been reached. Poor or an only temporarily positive response to treatment that is initiated on the basis of biopsy results may then be an indication that some other, more significant disorder is present. Further biopsy samples should then be obtained, via either endoscopy or surgery. Surgery is generally the recommended procedure at this point because a much more extensive evaluation of the GI tract can be accomplished. It should be emphasized that with proper instrumentation and technique, in conjunction with tissue examination by a pathologist experienced in evaluating the typically small tissue samples procured using endoscopic instrumentation, the correct diagnosis will be made in a great majority of animals that undergo endoscopy.
Diagnosis of Abnormalities of the Ileum
As previously stated, examination and biopsy of the ileum are important in patients with chronic diarrhea or weight loss that is clinically consistent with a small intestinal disorder. Although it is not always possible to enter the ileum in dogs and is rarely accomplished in cats because of the narrow diameter of the ileocolic orifice, the ileocolic valve can be readily identified during complete colonoscopy as long as the ascending colon and ileoceco- colic junction area are relatively clean (Figure 3-7).Biopsy samples can be blindly obtained from the ileum if the endoscope tip can be aligned with the ileocolic orifice so that the biopsy forceps can be passed through it and into the ileum. In dogs weighing more than 8 to 10 lb, I strongly prefer to obtain biopsy samples with the endoscope positioned in the ileum, whenever possible, so that any grossly abnormal areas can be pinpointed with the biopsy forceps.
The only disadvantage of ileoscopy compared with duodenoscopy is that the patient must be prepared for complete colonoscopy with a combination of fasting and colonic lavage. Ileoscopy done in conjunction with duodenoscopy also requires more anesthesia time and is therefore more expensive than if only one or the other is done. However, the great advantage of examining both the upper and the lower small bowel in patients with signs of chronic small intestinal disease is that a number of tissue samples can be obtained from a greater area of the intestinal tract.Histologic characteristics of the small intestine can then be more thoroughly evaluated. The large intestine is also routinely examined, and samples from it are obtained at the same time, even if there are no symptoms of colonic disease, because it has to be traversed to reach the ileum anyway. The thorough nature of this approach usually provides representative tissue for making an accurate diagnosis.
My experience to date has shown that in a majority of patients with inflammatory bowel disease, intestinal involvement is diffuse. Duodenal and jejunal changes are often similar in type and degree to those in the ileum. Sometimes a different cell type predominates in the ileum as compared with the duodenum, but usually no alteration in the treatment protocol is necessary. Occasionally, however, there are significant changes in the ileum when duodenal samples from the same patient are either normal or only mildly abnormal. I have examined several dogs with chronic diarrhea in which lymphoma was diagnosed on biopsies of the ileum, whereas duodenal samples revealed presence of only mildly abnormal inflammatory infiltrates. If ileoscopy had not been done in these patients, the diagnosis would have been missed! Also, the degree of inflammatory infiltrates is occasionally significantly more intense in the ileum than in the colon. Table 3-3 lists hematologic and histopathologic findings from a dog in which this was the case. I have also observed a patient with panhypoproteinemia that had mild lymphocytic-plasmacytic duodenitis. This degree of inflammatory disease is rarely significant enough to cause a protein-losing enteropathy. The patient did not respond to conventional therapy for inflammatory bowel disease. Subsequently, exploratory surgery identified adenocarcinoma in the terminal ileum, at a site where the diagnosis might have been made earlier if ileoscopy had been done.
These examples highlight the need to consider doing ileoscopy in patients with GI disorders characterized mostly by chronic diarrhea and weight loss. It is my impression that it is more important to recommend ileoscopy in dogs than in cats. Finally, if only colonoscopy is being done on a patient, using a flexible endoscope, it is wise to obtain ileum biopsy samples during the course of the procedure if access to the ileum can be gained. In this way, at least some information about the small intestine can be obtained. In my experience, most but not all patients with signs limited to large bowel diarrhea have normal ileum biopsies. If the ileum is abnormal, the treatment protocol might have to be altered.
Diagnosis of Large Intestinal Disorders
Flexible colonoscopy provides a means of thoroughly examining the entire colon to the level
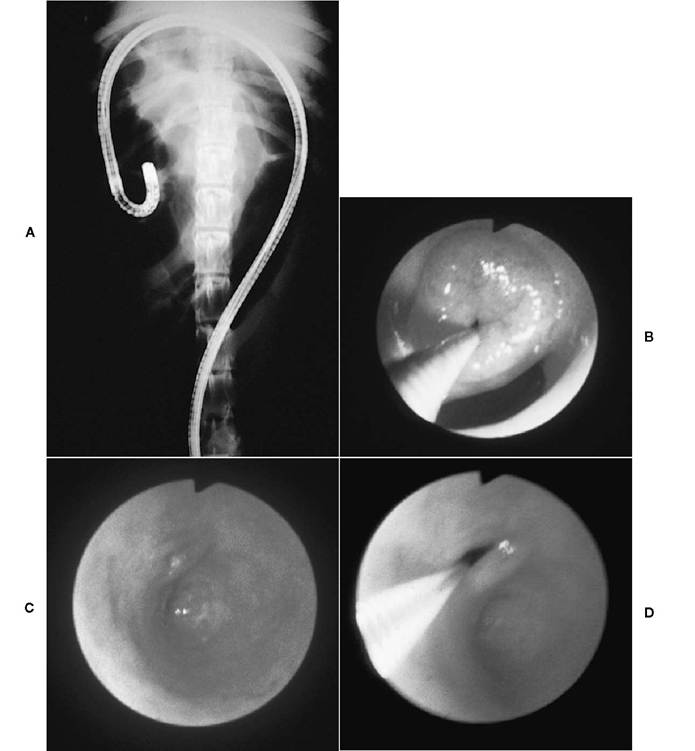
Figure 3-7 A, Radiograph showing the position of a flexible endoscope with the tip located close to the ileocecocolic area of a dog. With a flexible endoscope complete colonoscopy can be done, and in most dogs over 8 to 10 lb (and even in some smaller dogs when a pediatric endoscope is used) the endoscope can be passed into the ileum. B, Endoscopic view of the ileocolic orifice area in a dog. The ileocolic orifice in dogs usually appears as a broad, slightly raised papillary form. The cecal orifice is immediately below and is usually open. A biopsy forceps instrument has been advanced through the ileocolic orifice. C and D, Normal ileocolic orifice area of a cat. C, The ileocolic orifice appears as a very small opening (see D), and the cecum in the cat is simply a small blind pouch.
D, An endoscopic biopsy instrument has been advanced through the ileocolic orifice. Since it is not usually possible to pass an endoscope into the ileum of most domestic cats, ileum biopsies are frequently obtained by passing a biopsy forceps into the ileum under endoscopic guidance.
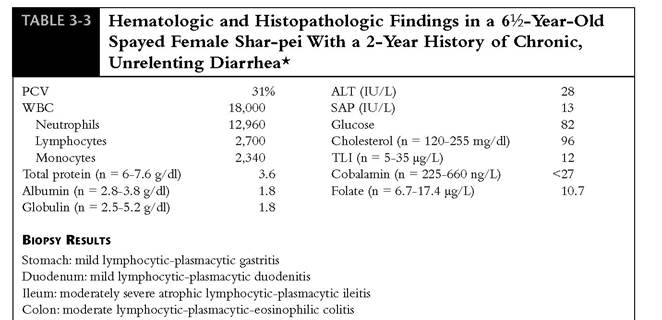
PCI, Packed cell volume; WBC, white blood cell count; ALT, alanine aminotransferase; SAPr serum alkaline phosphatase; TLIr trypsin-like immunoreactivity.
[*]Clinical signs were most consistent with a small bowel disorder. The dog had lost 18 lb in the last 3 months. Note the marked degree of panhypoproteinemia. The cobalamin level was quite low, whereas the folate level was normal. The subnormal cobalamin level was considered to be most consistent with intestinal bacterial overgrowth, which is common in shar-peis. It could also indicate significant disease in the ileum, although many dogs with ileal disease have a normal cobalamin level. Biopsies identified the most significant degree of disease to be in the ileum and colon. If only duodenal small bowel biopsies had been done, the true degree of small intestinal disease would have been misinterpreted, and treatment, especially drug doses prescribed, would most likely not have been aggressive enough. Also note the degree of histologic abnormality in the large intestine. This case example highlights the importance of doing ileoscopy and colonoscopy, as well as duodenoscopy, in dogs with chronic diarrhea.
of the ileocolic junction. The cecum in dogs can also be entered and examined. Indications for colonoscopy include signs of inflammatory disease (e.g., hematochezia, tenesmus, increased frequency of defecation), chronic diarrhea, constipation, fecal incontinence, and evaluation of a rectal or colonic mass. A second colonoscopy with follow-up biopsy is also useful as a means of monitoring response to therapy and in making decisions regarding treatment protocol adjustments in patients with inflammatory and neoplastic disorders. Colonoscopy is generally done only after dietary trials, therapeutic deworming either to treat known parasitism or to rule out the possibility of occult parasitism (especially whipworms), and empirical treatment for colitis have been tried and have proven ineffective in resolving symptoms. Colonoscopy should be done early in the course of symptoms that include hematochezia occurring with formed stools. The most common cause of this problem in dogs is rectal polyps. Abrasive material passing through the colon and chronic colitis are the two most common causes of this problem in cats.
The most commonly diagnosed disorders include a variety of mucosal inflammatory disorders (lymphocytic-plasmacytic colitis is the most common) and rectal polyps. Colonic strictures, histoplasmosis, parasitic typhlitis, inverted cecum, ileocolic intussusception, and neoplasia are seen less commonly but can be reliably diagnosed by colonoscopy. Colonoscopy is much more accurate than contrast radiography in obtaining a definitive diagnosis of large intestinal disorders.
A majority of patients with idiopathic colitis have grossly normal mucosa. Confirmation of the diagnosis requires that the colon be properly prepared so that high-quality biopsy samples can be obtained from various levels of the colon. If the ileocolic area can be reached, an attempt should be made to obtain biopsy samples from the ileum as well. In patients with chronic diarrhea that is not clearly limited to large bowel signs, it is best to obtain biopsy samples from both the small and the large intestine.
Endoscopic Removal of Gastrointestinal Foreign Bodies
Many foreign objects can be successfully removed from the esophagus, stomach, and colon using endoscopic instrumentation. Rigid esophagoscopy under general anesthesia was the procedure of choice for removal of esophageal foreign bodies until the late 1970s. Even now it is occasionally used preferentially over flexible equipment in the retrieval of difficult-to-remove esophageal bone foreign bodies. Surgical removal via gastrotomy, enterotomy, and colotomy has long been the standard method of management for foreign bodies of the stomach, small intestine, and large intestine, respectively. Improvements in the optics and maneuverability of flexible fiberoptic endoscopes and development of foreign body grasping forceps, retrieval baskets, and polypectomy snares for use with endoscopes, however, have clearly made endoscopic retrieval the current procedure of choice for dealing with retained esophageal and gastric foreign bodies. The first reports of removal of GI foreign bodies with a flexible fiberoptic endoscope appeared in 1972. Since then physicians and veterinarians have become adept at retrieving objects of various sizes and shapes, and it is currently a very uncommon occurrence for a patient with a foreign body in the esophagus, stomach, or colon to have to undergo surgical removal. A majority of gastric foreign bodies can be successfully removed via endoscopy (85% success rate in my series in which endoscopy was attempted for foreign body retrieval). Case selection in regard to gastric foreign bodies is important; that is, a gastrotomy would be done without any attempt to do endoscopy if radiographs confirm the presence of a very large gastric foreign body.
There are numerous advantages to endoscopic foreign body removal when compared with other means of treatment. The procedure is minimally invasive and not appreciably time-consuming (average time in my series once anesthesia is induced is 5 to 15 minutes). Especially troublesome objects may require up to an hour, but endoscopy is still less expensive and less invasive than surgery. Patients are often discharged within 4 hours to 2 days of the procedure. Endoscopy allows for rapid intervention when sharp objects or valuable prized possessions such as jewelry or coins are ingested. Rather than rely on observation and radiographic surveillance in such clinical situations, endoscopic equipment can be used to quickly retrieve the object in question. The main limiting factor when considering endoscopy versus observation is the necessity for using general anesthesia for endoscopy.
Foreign objects that can be removed with a high rate of success include needles, coins, bottle caps, fruit pits, pieces of toys, cloth material, bone chips, rocks, food wrappers, narrow hairballs, and many others. The success rate for removal of fishhooks is variable (55% to 70%) and depends on how deeply the hook is imbedded in the mucosa before endoscopy. Frequently bones can be retrieved from the esophagus. If it is not possible to remove a bone through the mouth, attempts are made to advance it to the stomach. A decision is then made either to remove the bone via gas- trotomy or, alternatively, to leave it in the stomach for digestion by gastric acid. Bones are usually decalcified by gastric juices, and the remaining fragments pass through the intestinal tract without incident. Foreign bodies that are not likely to be removed endoscopically include corn cobs, large rocks, and large hard rubber balls. Problems with retrieval of these objects are related to their size in relation to the width of the grasping range of pronged foreign body retrieval instruments and the likelihood that they can be positioned at an angle that will facilitate passage through the lower and upper esophageal sphincters. The weight and surface texture of the foreign body also must be taken into consideration. Smooth objects are sometimes difficult to grasp firmly enough for retrieval through the narrow areas of the lower and upper esophageal sphincters, especially when the object is heavily coated with gastric mucus.
A variety of instruments are available for foreign body retrieval. A laryngoscope and forceps (e.g., Kelly clamp, sponge forceps) are used for pharyngeal foreign bodies and for retrieval of any object that is difficult to pull through the upper esophageal sphincter with standard prong type of endoscopic grasping instruments.Two-, three-, and four-pronged grasping instruments are most commonly used with flexible endoscopes. The diameter of the working channel of the endoscope limits to some degree the type and size of grasping instruments that can be used. Larger, sturdier instruments made by some manufacturers require a 2.8-mm or larger working channel. Pediatric endoscopes that are less than 9 mm in diameter have a working channel diameter range of 2 to 2.5 mm,

Figure 3-8 Two-pronged grasping forceps.Width between grasping teeth when fully separated is approximately 1.4 cm.
depending on the manufacturer. In my experience, a majority of gastric and esophageal foreign bodies can be successfully retrieved with instrumentation that can be used through a 2-mm channel. A sturdy two-pronged instrument (Figure 3-8) is adequate for most foreign objects and can be used with pediatric endoscopes with a narrow working channel. Sheathed four-pronged graspers can be purchased for use through small working channels, but these instruments do not tend to be durable.
Polypectomy snares (Figure 3-9) are the most versatile instruments for removal of foreign objects. The snare loop can be extended around an object to provide a much stronger grasp than can sometimes be achieved by the single-end grasp applied by a pronged instrument. Basket retrievers can also be used for this purpose, but I have found snare instruments to be more versatile. The two instruments that I have used for virtually all of my foreign body cases are the two-pronged instrument and a polypectomy snare. Both of these instruments should be a part of standard instrumentation armamentarium since there are instances where each of the instruments will be superior to the other. Examples of successfully retrieved objects are shown in Figures 3-10 and 3-11.
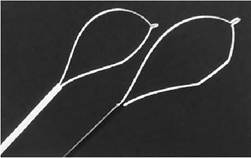
Figure 3-9 Oval (left) and crescent (right) grasping snares. Snares are the most versatile instruments for removal of foreign objects.

Figure 3-10 Two rocks retrieved with a two-pronged grasper (shown in Figure 3-8) from a golden retriever with a 6-day history of anorexia but no vomiting. A snare loop could also have been used. It is possible to retrieve fairly sizeable foreign objects with endoscopic instrumentation. (From Tams TR: Endoscopic removal of gastrointestinal foreign bodies. In Tams TR, ed: Small animal endoscopy, St. Louis, 1999, Mosby.)