LAPAROSCOPY
Laparoscopy is an operative procedure, performed through a keyhole opening with a rigid endoscope, that allows visual inspection and biopsy of the peritoneal cavity and its organs.
Laparoscopy was first introduced in 1901 in human medicine, and it was quickly recognized in the early years as a valuable diagnostic procedure for diseases of the liver. With the laparoscopic instrumentation that is available today, bright, clear images of the peritoneal cavity are readily produced and laparoscopic photographs can be spectacular.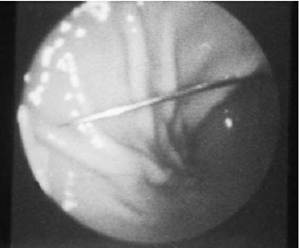
Figure 3-11 Needle foreign body in the stomach of a cat. Once grasped from either end, this foreign object can quickly and easily be removed via endoscopy.
(From Tams TR: Endoscopic removal of gastrointestinal foreign bodies. In Tams TR, ed: Small animal endoscopy, St. Louis, 1999, Mosby.)
Until fairly recently, the most common indications for laparoscopy in human clinical medicine included evaluation of liver disease, staging for cancer treatment (liver and peritoneal metastases), diagnosis of various peritoneal diseases (e.g.,ascites of unknown etiology, fever of unknown origin, abdominal pain of unknown etiology, endometriosis, portal hypertension), and diagnosis of pelvic soft tissue disease, diseases of the spleen, and pancreatic disease. Laparoscopy has also been used extensively in recent years in evaluation of the female reproductive organs and for in vitro fertilization techniques. The list continues to grow! There have also been tremendous advances in laparoscopic surgical techniques over the last 10 years in human medicine. For example, it is now routine for cholecystectomy procedures to be done entirely via laparoscopy (“keyhole surgery”). Advantages of laparoscopic cholecystectomy in humans include significantly less postoperative pain and discomfort, short periods of hospitalization (most patients are discharged on the first postoperative day), and earlier feeding when compared with standard surgical cholecystectomy.
Cholecystectomies done through a large abdominal incision (open cholecystectomy) have now become a rarity. Newer procedures that are now being done include laparoscopic removal of common bile duct stones through the cystic duct, management of hiatal hernias and recurrent or bilateral inguinal hernias, and left- or right-sided colectomies. Laparo-
Figure 3-12 Laparoscopic view of normal canine pancreas (right limb). The examination was performed with a 5mm-diameter telescope.
scopic surgery is clearly one of the most exciting areas of study and new technology in the field of human surgery today.
Laparoscopy has been used in veterinary medicine with any degree of frequency only for the last 25 to 30 years. Its early use centered around reproductive function studies in food animals and equine, nonhuman primate, and various zoo and exotic species. Laparoscopy is most commonly used now in small animal medicine to examine and perform biopsies of the liver, kidneys, pancreas, and prostate. It provides an excellent means for visualizing the surface of the liver. Even subtle color and texture changes can be readily detected. The pancreas can usually be thoroughly examined (Figure 3-12). Pancreatic biopsy samples can be safely obtained, thus making laparoscopy a useful diagnostic procedure in evaluating patients for pancreatitis (Figure 3-13). Also, laparoscopic instrumentation is now used extensively in avian patients for examination of the abdominal and thoracic cavities. Panoramic views of both areas can be achieved through a single puncture site.
Most veterinarians have had little or no exposure to laparoscopy during their training in veterinary school. Ultrasonography has become the dominant procedure for imaging abdominal organs and for obtaining biopsy samples in a minimally invasive way. Laparoscopy still plays a major role in clinical practice for many veterinary gastroenterologists, however, and many small animal practitioner s are now beginning to perfor m laparoscopy in their general practices.
To see an organ clearly during biopsy, to obtain biopsy samples readily from even a small liver, to observe
Figure 3-13 Pancreas biopsy site (left of center near the bottom of the field of view). The closed spoon biopsy instrument is seen in the upper right, being used to hold the pancreas in position. A pancreatic vessel is observed in the upper left.
directly the degree of hemorrhage associated with the biopsy, and to examine and obtain biopsy samples from the pancreas directly are major advantages of laparoscopy. Many veterinarians, once they observe the technique and see firsthand the sharp, clear views that can be achieved in the abdomen, express keen interest in learning more about laparoscopy and in purchasing equipment. Although the indications for laparoscopy may be far more extensive in human medicine, it still has many potential applications for use in veterinary medicine. It is a procedure that can be performed with a high degree of safety. Various minimally invasive surgical techniques (endosurgery) have now been developed for use in animals, and wet lab courses for training in these procedures are available. Although laparoscopy can be done in conjunction with local anesthesia and light sedation for minor procedures, I routinely do procedures under isoflurane general anesthesia while providing appropriate supportive care. This is well tolerated by a great majority of patients.
Instrumentation
The basic equipment needed to perform laparoscopy includes a telescope (laparoscope) and corresponding trocar-cannula unit (Figure 3-14), Veress (insufflation) needle, light source (Figure 3-15), gas insufflator unit, flexible fiberoptic light transmission cable, and tubing for transferring gas from the insufflation unit to theVeress cannula and the laparoscope cannula. A complete list of needed supplies appears in Box 3-1. If handled and cared for properly, laparoscopic instruments can last for
A
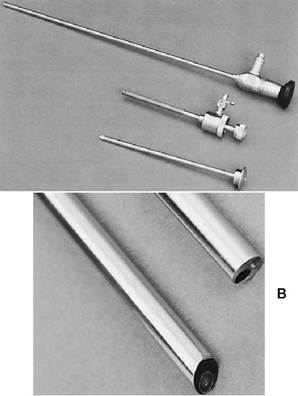
Figure 3-14 A, Laparoscopic instrumentation.
Shown (top to bottom) are telescope (5 mm ? 29 cm), insertion cannula (sleeve unit through which the telescope is passed to enter the abdomen), and trocar with pyramidal point. Abdominal puncture is made by advancing the trocar (placed inside the cannula unit) through a small incision, after a pneumoperitoneum has first been established. The insertion cannula is then advanced as the trocar unit is simultaneously backed out. B, Close-up view of laparoscope tips, with straight forward-viewing angle (0 degrees, top) and oblique forward-viewing angle (30 degrees, bottom).many years without need for repair. Many small animal practices could readily support the purchase of a set of instruments for performing laparoscopy.
It is beyond the scope of this chapter to provide a complete description of each instrument and technique for its use. One of the most important issues to discuss here involves which telescope diameter size is most suitable for use in cats and small dogs, as well as in large dogs. Laparoscopes applicable for use in small patients range from 1.7 to 10 mm in diameter. The 10-mm laparoscope requires a 2-cm incision for insertion of the cannula unit (the instrument through which the telescope is passed to enter the abdominal cavity). This size laparoscope is generally too large for use in cats and most small dogs. The smallest laparo-

FIGURE 3-15 Endoscopic light source with automatic light intensity (175-watt Xenon). A fiberoptic light guide cable is attached.The same light source can also be used for other endoscope instruments (e.g., flexible endoscopes, bronchoscopes).
BOX 3-1
Instrumentation for General Laparoscopy
Supplies for Local Anesthesia, Skin Incision, and Closure
Syringes for anesthetic solutions
Lidocaine or Carbocaine (if general anesthesia is not used)
Towel pack and fenestrated drape
Towel clamps
Scalpel blades (no.
10, no. 15)Thumb forceps Gauze sponges
Bowl and sterile saline
Curved mosquito forceps (two) Straight mosquito forceps (two)
Needle holder Suture scissors
2-0 or 3-0 catgut or polydioxanone (PDS)
2-0 or 3-0 nylon
Laparoscopic Instrumentation
Veress needle
Laparoscope (telescope) Fiberoptic light cable
Gas insufflation tubing Laparoscope cannula (sleeve) with trocar Second puncture cannula with trocar Tactile (palpating-measuring) probe Set of assorted rubber sealing caps Tru-Cut biopsy needle Biopsy forceps
Modified from Magne ML,Tams TR: Laparoscopy: instrumentation and technique. In Tams TR, ed: Small animal endoscopy, St. Louis, 1999, Mosby. scope is used with a 2.2-mm cannula that can be advanced through a very small incision, thus making it useful for even very small patients. A major disadvantage of the smaller laparoscopes, however, is that they provide a limited field of vision. Also, a more powerful light source is required for good image quality because the smaller scopes contain fewer light bundles. A 5mm-diameter laparoscope is versatile and is the ideal size for use in dogs and cats. Many veterinarians experienced in performing laparoscopy recommend a 5-mm unit if only one scope is to be purchased.
For a thorough laparoscopic examination, it is essential that a pneumoperitoneum be established. This provides abdominal distention sufficient to maintain a workspace for the laparoscope and allows for greater range of visualization of abdominal organs. Various methods have been used to establish a pneumoperitoneum, including insufflation of room air by a syringe, three-way stopcock, and micropore air filter system, bulb pumps, gas tanks, and carbon dioxide dispensers. Although any of these methods can be used satisfactorily, use of an automatic insufflator unit for nitrous oxide or carbon dioxide is greatly preferred (Figure 3-16). These units have a self-contained internal tank that must be filled from an external tank.
This provides for controlled insufflation and greater safety and convenience during the procedure.
Figure 3-16 Gas insufflation unit for laparoscopy. Gauges that measure gas supply, intra-abdominal pressure, gas flow rate, and amount of gas insufflated are located on the front of the unit. A Veress needle is shown connected to the gas insufflation tubing by a Luer-Lok attachment.
Various ancillary instruments are available for use during laparoscopy (Figure 3-17). The most commonly used biopsy instrument is a doublespoon forceps (Figures 3-18 and 3-19).Although operating laparoscopes with a channel for insertion of accessory instruments are available, most veterinary laparoscopists prefer to use a doublepuncture technique for biopsy. An accessory cannula is inserted to the abdomen through a second small incision. This technique allows greater mobility of accessory instruments (palpation probes, biopsy instruments). Alternatively, a biopsy needle can be inserted directly through the abdominal wall and then directed to the biopsy site under laparoscopic guidance.
Indications
The primary indications for laparoscopy in evaluation of diseases of the digestive system involve problems that necessitate examination and biopsy of the liver and/or pancreas.
Laparoscopy provides a superb view of the liver (Figure 3-20). Color, consistency, and contour of the liver are rapidly documented. A probe can be inserted through the second puncture cannula for the purpose of palpating the surfaces of the liver to evaluate for friability or excessive rigidity, to lift and separate the liver lobes in view so that the undersides can be examined, to palpate the gallbladder, and to displace omentum from a surface that must be examined (Figure 3-21). The liver is generally evaluated through a right lateral midabdominal approach. A significantly greater area of liver can be visualized from the right side compared with a ventral or left approach. The right lateral, right medial, and caudate lobes of the liver and the gallbladder and extrahepatic biliary tract can be thoroughly examined from the right side. A left approach is generally made only if disease
Figure 3-17 Assorted laparoscopic hand instruments. Included (top to bottom) are injection/aspiration needle, palpation probe, scissors, grasping forceps, biopsy forceps, and suction cannula.
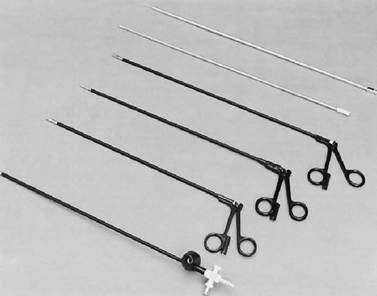
FIGURE 3-18 Close-up view of laparoscopic hand instrument tips. Shown (left to right) are double-spoon biopsy forceps, grasping forceps, scissors, suction cannula, palpation probe, and injection/aspiration needle.

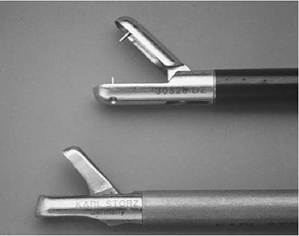
Figure 3-19 Close-up view of laparoscopic biopsy forceps: double-spoon grasping type of forceps (top) and cutting type of forceps (bottom).
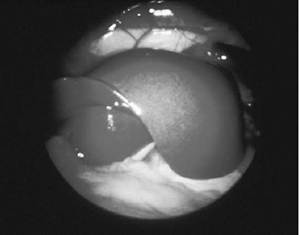
Figure 3-20 Normal canine liver viewed from a right lateral approach. The diaphragm is in the background.
involving the left lateral or medial lobe is suspected. Examination of the liver and surrounding structures usually takes only several minutes.
Abnormal gross liver changes that can be readily appreciated include hepatic lipidosis (the liver has a pale mustard color with friable texture), glycogen-laden liver, metastatic or multifocal neoplasia (raised and often discolored tumor nodules with central cavitations or depressions are seen), nodular hyperplasia (multiple raised nodules without central depressions, often with a yellow fatty appearance), cirrhosis, cholangiohepatitis, extrahepatic biliary tract obstruction, and others (Figure 3-22). Liver size and presence of any venous plexuses suggestive of acquired collateral shunting are readily appreciated.
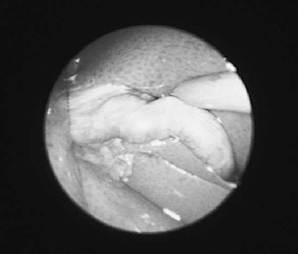
Figure 3-21 Normal gallbladder in a cat.
A palpation probe is being used to lift liver away so that the gallbladder can be seen. The liver is paler than normal. Liver biopsy confirmed a diagnosis of hepatic lipidosis.
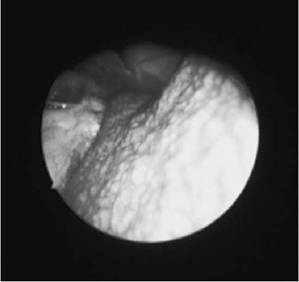
Figure 3-22 Marked diffuse granularity of the liver in a 4-year-old Maltese with chronic active hepatitis. This is an unusual appearance. The dog was clinically normal; however, screening laboratory tests done before a dental procedure suggested that the patient had a liver disorder, and both preprandial and postprandial serum bile acid levels were significantly elevated. Liver biopsies were obtained laparoscopically. (From Magne ML, Tams TR: Laparoscopy: instrumentation and technique. In Tams TR, ed: Small animal endoscopy, St. Louis, 1999, Mosby.)
A total of three to six or more liver biopsy samples, procured from any abnormal-appearing, as well as normal-appearing, areas, are usually obtained. Using grasping forceps advanced through the second puncture cannula, this can be done quickly and safely. One of the most significant advantages of laparoscopy-guided biopsy as compared with ultrasound-guided or blind percutaneous biopsy techniques is the direct visualization of the biopsy procedure itself. Once experience is gained, even biopsies of small livers can be rapidly performed (Figure 3-23). In cases in which extra tissue samples are needed for culture and/or quantitative copper analysis, the procedure can still be quickly completed. An additional advantage to direct visualization is that a gross description of the liver can be communicated to the pathologist. Finally, with use of spoon biopsy forceps sample size is somewhat larger than what is obtained with needle biopsy instruments, meaning that there is a greater certainty that representative liver tissue is being obtained for microscopic examination.
Indications for biopsy of the pancreas include ruling in or out acute pancreatitis when other tests have failed to establish clearly a diagnosis (i.e., obvious pancreatitis is not an indication for laparoscopy), identification of chronic recurring pancreatitis, and differentiation of pancreatic disease
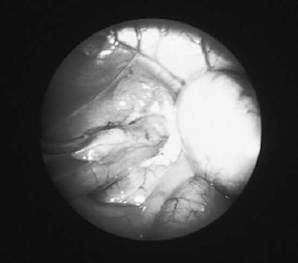
FlGURE 3-23 Microhepatia and cirrhosis in a 3-year- old cocker spaniel with a 3-week history of intermittent vomiting and anorexia. Liver enzyme levels were only mildly elevated, but both resting and postprandial bile acid values were markedly increased. Several small lobes of liver can be seen to the left of the gallbladder. The caudal vena cava is seen between two of the lobes (8 o’clock position). The oval window of the diaphragm is in the background (light area at the top of the field). The dog lived 15 months after the diagnosis of severe liver disease was made. NOTE: Laparoscopy is an ideal method for safely and quickly obtaining liver biopsies in patients with a small liver. from liver disease. It is not uncommon for cats with chronic cholangitis or cholangiohepatitis to have concurrent chronic fibrosing pancreatitis. Simultaneous biopsy of liver and pancreatic tissue during laparoscopy aids in establishing extent of involvement in this syndrome.
The pancreas can usually be visualized through a right abdominal approach. It may be necessary to displace omentum from the pancreas in order to visualize it clearly. The right wing of the pancreas is found adjacent to the duodenum. Usually only a small portion of the left pancreatic lobe can be seen. In some obese patients it is difficult to find the pancreas. Biopsy samples of the pancreas are generally obtained only if the organ is grossly abnormal. The safest technique is to use grasping forceps to procure a small piece of the right pancreatic wing. The central duct area must be avoided. Parapancreatic fat nodules that represent either calcification, fibrosis, or necrotic tissue may be found. Great care in trocar placement must be exercised when performing laparoscopy in any patient that is likely to have acute pancreatitis.
Contraindications
Because laparoscopic procedures are generally short in duration (10 to 30 minutes when done by an experienced operator) and not considered significantly invasive, the risks are not as great as those that can be associated with exploratory laparotomy. By the time a decision to recommend laparoscopy is made, there has been ample opportunity for the clinician to evaluate the patient thoroughly through history, serial physical examinations, selected laboratory tests, and radiography. There are several absolute contraindications for performing laparoscopy. These include acute or unstable cardiopulmonary conditions, presence of an uncor- rectable or severe coagulopathy, cases in which extensive intraabdominal adhesions could have developed, bowel obstruction, abdominal herniation (diaphragmatic or inguinal), and septic peritonitis.
A relative contraindication must be balanced against the need for diagnosis and risks of alternative methods of diagnosis. The latter options usually include either ultrasound-guided biopsy (sedation is still required) or general anesthesia and laparotomy. With administration of proper patient support and use of the safest possible sedation and anesthetic protocols (e.g., ketamine and diazepam or propofol and the general anesthetic agent isoflu- rane or sevoflurane), many elderly or compromised patients can tolerate laparoscopy with minimal or no problems. Ascites can complicate laparoscopy. The main problem involves clouding of the field of view. When ascites is present, it is usually best to remove as much of the fluid as possible before the procedure. This is best accomplished using either diuretics, if the ascites is mild and the procedure is not scheduled to be done for several days to a week, or centesis, on the day before or the day of the procedure if the ascites is moderate to severe.
Complications
The complication rate associated with laparoscopy depends on operator experience, accurate patient assessment and recognition by the clinician of appropriate indications and any possible contraindications, and quality of the laparoscopic equipment used. As an invasive procedure, laparoscopy is remarkably safe. Most surveys in human and veterinary medicine indicate that, as is the case with most procedures, errors and complications of laparoscopy are more common when the technique is still being learned. Complications during laparoscopy can be avoided with a high degree of success when the operator uses a systematic approach and careful attention to detail. Potential major complications that can occur include air embolism (related to abdominal insufflation), cardiopulmonary arrest, pneumothorax (from diaphragmatic puncture by a misguided instrument), damage to internal organs, bleeding, and infection. Because laceration of a major vessel can occur when attempting to obtain biopsy samples from a small liver with a needle instrument, it is recommended that grasping forceps be used instead in this situation (see Figure 3-19). In fact, this is the instrument that I routinely use to obtain liver samples in almost all liver biopsy cases. Patients with end-stage liver disease are at risk of decompensating at any time and in association with even minor procedures. Owners should be warned that this possibility exists before any type of procedure in a patient with severe liver disease. Minor complications include subcutaneous emphysema and subcutaneous leakage of ascites fluid around the puncture site. These are usually transient problems.
References
Brady PG: Endoscopic removal of foreign bodies. In Silvis SE, ed: Therapeutic gastrointestinal endoscopy, New York, 1985, Igaku-Shoin.
Freeman LJ, Kolata RJ,Trostle S: Minimally invasive surgery of the gastrointestinal system. In Freeman LJ, ed: Veterinary endosurgery. St. Louis, 1999, Mosby.
Lightdale CJ: Indications, contraindications, and complications of laparoscopy. In Sivak MV, ed: Gastroentero- logic endoscopy. Philadelphia, 1987,WB Saunders.
Magne ML,Tams TR: Laparoscopy: instrumentation and technique. In Tams TR, ed: Small animal endoscopy. St. Louis, 1999, Mosby, pp 397-408.
Morgenstern L: A new era of keyhole surgery, Gastrointest Endosc Clin North Am 3:183, 1993.
Nord HJ: Technique of laparoscopy. In Sivak MV, ed: Gastroenterologic endoscopy, Philadelphia, 1987, WB Saunders.
Quilici PJ: Laparoscopic cholecystectomy, Gastrointest Endosc Clin North Am 3:221,1993.
Tams TR: Endoscopic examination of the small intestine. In Tams TR, ed: Small animal endoscopy, St. Louis, 1999, Mosby.
Tams TR: Endoscopic removal of gastrointestinal foreign bodies. In Tams TR, ed: Small animal endoscopy, St. Louis, 1999, Mosby.
Tams TR: Endoscopy, In Kirk RW, Bonagura JD, eds: Current veterinary therapy X. Philadelphia, 1989, WB Saunders.
Twedt DC: Laparoscopy of the liver and pancreas. In Tams TR, ed: Small animal endoscopy. St. Louis, 1999, Mosby.
Willard MD: Colonoscopy. In Tams TR, ed: Small animal endoscopy. St. Louis, 1999, Mosby, pp 217-245.