Esophageal foreign bodies
Esophageal foreign bodies occur relatively frequently in the dog, but less so in the cat. The most commonly encountered esophageal foreign bodies in dogs are bones, fishhooks, and food or compressed chew treats.30-34 In cats, fishhooks, needles, and trichobezoars are most commonly encountered.30,35 Foreign bodies generally lodge in those areas of the esophagus that are least distensible, namely the thoracic inlet, the heart base, and the cardia.16,30-32 The severity of damage produced by the foreign body depends on the duration of the obstruction and the size and angularity of the foreign body.17 Pressure necrosis of the esophageal wall can occur, and tends to be more severe with larger foreign bodies and those that have been present for a longer duration.
Full thickness damage can occur resulting in esophageal perforation, mediastinitis, pleu- ritis, and on occasion fatal hemorrhage.33 The clinical signs are those of esophageal obstruction. Most commonly regurgitation, odynophagia, ptyalism, avoidance of food, dysphagia, halitosis, retching, and gagging are seen.30,32,34 In some cases, the owner may have seen the animal eat the offending object. The physical examination may be normal, but typically will reveal signs of esophageal pain including multiple attempts to swallow with extension of the head and neck, ptyalism, and possibly a hunched appearance.Diagnosis is often made by historical information and survey thoracic radiographs (Figure 3.4). Occasionally, a contrast study may be needed to detect radiolucent objects. Evidence of esophageal perforation may be present and includes pneumomediastinum, pneumothorax, and mediastinal or pleural fluid, but these findings may be unreliable.36
Removal of the foreign body should be immediate or as soon as the patient has been stabilized.
Endoscopy is the preferred method of removal if the esophagus has not been perforated (Figure 3.5).30,32,34,35,37 The foreign object may be removed via the mouth or gently pushed into the stomach and removed via gastrotomy or allowed to be digested (e.g., bones or food). Extreme care must be exercised when attempting to remove an esophageal foreign body via endoscopy. Perforation during endoscopic removal may occur. Once the foreign body has
a
Figure 3.4 a,b:
Esophageal foreign body. Lateral and VD radiographs of a 3-year-old spayed female American Staffordshire Terrier with regurgitation and anorexia for 3 days. The bone esophageal foreign body can be seen on the lateral radiograph at the level of the 3rd and 4th ribs just ventral to the trachea and on the VD radiograph at the level of the 3rd rib to the left of midline.

b
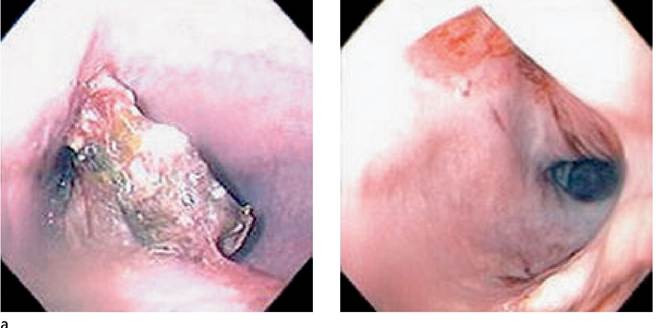
Figure 3.5 a,b:
Esophageal foreign body. Endoscopic views of the bone esophageal foreign body in the same dog shown in Figure 3.4 before and after endoscopic removal of the bone.
b
been removed, the esophageal mucosa should be fully evaluated for any potential damage (Figure 3.5b). An erythematous mucosa and mild erosions are common. Thoracic radiography should be repeated after endoscopic removal of a foreign body if a perforation is suspected. Fluoroscope-guided removal has also been used successfully in some patients.31 Surgical removal may be needed in cases where endoscopic removal is unsuccessful or when a perforation has occurred.32,34,36,37 Following removal of the foreign body, animals with no to minimal esophageal damage may not need any medical therapy. Animals with moderate to severe damage should be treated for esophagitis.17 In addition, broad spectrum antibiotics may also be used preventatively as esophageal mucosal barrier function has been lost.
Some clinicians have recommended the use of anti-inflammatory doses of corticosteroids in an attempt to prevent esophageal stricture formation, but this therapy is as of yet unproven. If esophageal damage is severe, the clinician may wish to rest the esophagus and feed the animal through a gastrostomy tube. The prognosis is generally good;
Figure 3.6:
Esophageal stricture. Lateral thoracic radiograph of a 2-year-old castrated male Miniature Pinscher with regurgitation, dysphagia, and anorexia. The dog had been seen to eat a foreign body approximately 2 weeks prior to presentation. A small amount of air can be seen in the mid esophagus.
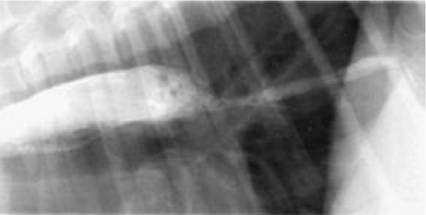
Figure 3.7:
Esophageal stricture. Barium esophagram of the same dog as shown in Figure 3.6. An esophageal stricture can be seen in the mid to distal esophagus.
however, some animals may develop complications, the most common of which is esophageal stricture formation.18,23,32
3.3.5