Exocrine pancreatic neoplasia
Neoplastic diseases of the exocrine pancreas can be primary or secondary. Primary neoplastic diseases of the exocrine pancreas can be classified as benign or malignant. Pancreatic adenomas are benign tumors, which are usually singular and can be differentiated from pancreatic nodular hyperplasia (Figure 8.12) by the presence of a capsule.
Just as in human beings, pancreatic adenocarcinoma (Figure 8.13) is the most common malignant neoplastic condition of the exocrine pancreas in dogs and cats. But, in contrast to humans, where pancreatic adenocarcinoma is the fourth most common cause of cancer death, it occurs rather infrequently in dogs and cats.130 Adenocarcinomas are malignant and usually originate from the duct system, but can also originate from acinar tissue.131 A few cases of pancreatic sarcomas (i.e., spindle cell sarcoma and lymphosarcoma) have also been reported.131,132 However, it is questionable whether these tumors are primary neoplastic lesions of the exocrine pancreas, metastatic lesions of tumors of other organs, or a localized lesion of a multicentric neoplasia.Etiology and pathogenesis
As in humans, the etiology of neoplastic conditions of the exocrine pancreas is unknown in dogs and cats. Neoplastic lesions can lead to the transposition of the organs of the cranial abdomen. However, these changes are subclinical in most cases and the diagnosis is often made as an incidental finding on necropsy examination. In a small number of human patients, the neoplastic growth can actually obstruct the pancreatic duct and cause secondary atrophy of the remaining exocrine pancreas, leading to EPI. Even though such cases have not yet been reported in the cat and have only been anecdotally reported in a single dog, this possibility should be considered and patients presenting with clinical signs compatible with EPI should have their abdomen carefully palpated (Hill S, personal communication, 2007).
In addition to a transposition of abdominal organs, adenocarcinomas can also be associated with tumor necrosis when the tumor outgrows its vascular supply. Tumor necrosis in turn will cause a local inflammatory response, which can lead to the development of clinical signs of pancreatitis. Finally, exocrine pancreatic tumors can also spread to neighboring or distant organs.
Clinical signs and diagnosis
The presentation of canine and feline patients with exocrine pancreatic neoplasia is nonspecific. In a case series of 58 cats, the clinical signs most commonly reported were anorexia (46%), weight loss (37%), lethargy (28%), vomiting (23%), icterus (14%), constipation (9%), and diarrhea (3%).131 The clinical signs reported in other cases were polyuria, fever, de-
hydration, a distended cranial abdomen, and voluminous, pale, soft stools.132 Polyuria may be a clinical sign of concurrent diabetes mellitus. Obstructive jaundice has also been described in a cat with pancreatic adenocarcinoma.133 A small number of dogs with multifocal necrotizing steatitis have been described that were ultimately diagnosed with pancreatic adenocarcinoma.134 Finally, clinical signs related to metastatic lesions have also been reported in some cases of pancreatic adenocarcinoma and may present as lameness, bone pain, or dyspnea. Recently, several cases of paraneoplastic alopecia have been reported in cats with pancreatic adenocarcinoma.135,136 The reported alopecia consisted of a generalized alopecia of the ventrum, limbs, and face in most cases, with diffuse zones of alopecia in the remaining cats.135,136
Neutrophilia, anemia, hypokalemia, bilirubinemia, azotemia, hyperglycemia, and elevations of hepatic enzymes have all been reported in affected patients, but the results of routine blood tests may be unremarkable.131,132 Elevations of serum hepatic enzyme activities and serum bilirubin concentration are identified most commonly.137 Hyperglycemia, when present, is related to the concurrent destruction of pancreatic beta cells.
Serum activities of lipase and amylase have not been commonly reported in either dogs or cats with pancreatic adenocarcinoma. There are some anecdotal reports indicating that serum lipase activities may be extremely high in dogs with pancreatic adenocarcinoma, but this has not been substantiated in other studies. A single dog with a pancreatic adenocarcinoma and pseudohyperparathyroidism (leading to hypercalcemia) has been described in the literature.138Radiographic findings are also nonspecific in most cases and include a decreased contrast in the cranial abdomen, suggesting peritoneal effusion into this area, transposition of the spleen caudally, and shadowing in the pyloric region.132 However, in some cases abdominal radiographs can suggest the presence of a mass in the cranial abdomen.137 Ultrasonographic examination of the abdomen is very helpful and in most cases a soft tissue mass can be identified in the region of the pancreas;44,137,139 although in many cases, continuation of the mass with pancreatic tissue cannot be conclusively identified.137 Similarly, neoplastic lesions of the neighboring organs may be falsely presumed to be of pancreatic origin.44 Also, patients with severe pancreatitis may show an ultrasonographic mass effect in the area of the pancreas that must not be confused with a pancreatic adenocarcinoma.42,44
If peritoneal effusion is identified on abdominal ultrasound, a sample should be aspirated and evaluated cytologically. However, in most cases, neoplastic cells do not readily exfoliate into the peritoneal effusion and no neoplastic cells are identified on cytology. Fine needle aspiration or transcutaneous biopsy under ultrasound guidance can be attempted when suspicious masses are identified and has been reported to be successful in approximately 25% of all cases.137 The low success rate of fine needle aspiration is probably due to the lack of exfoliation of pancreatic adenocarcinoma cells.
In other cases, carcinoma cells can be identified but the origin of the cells cannot be determined conclusively.137 Ultrasound- guided biopsy with histopathological evaluation of biopsy samples has been reported infrequently, but in one study 2 of 2 cases where an ultrasound-guided biopsy of a pancreatic mass was performed a diagnosis of pancreatic adenocarcinoma was made.137 In 2 of 3 other cases, biopsy of the liver revealed metastatic carcinoma.137 However, in many cases the diagnosis is made at exploratory laparotomy or even on necropsy examination.Therapy and prognosis
Pancreatic adenomas are benign and theoretically do not need to be treated unless they cause clinical signs. However, since the final diagnosis of pancreatic adenocarcinoma is often made by way of a surgical biopsy, a partial pancreatectomy should be performed even in cases of suspected pancreatic adenoma. The prognosis in these cases is excellent.
Patients with a pancreatic adenocarcinoma often present at a late stage of the disease. Metastatic disease at the time of diagnosis is common in dogs with this disease and has been reported to occur in 81% of cats.131,1408 The most common sites of metastatic disease are the liver, abdominal and thoracic lymph nodes, mesentery, intestines, and the lungs; but various other metastatic sites have also been reported.137 In those few cases where gross metastatic lesions are not identified at the time of diagnosis, surgical resection of the tumor may be attempted, but owners should be forewarned that clean surgical margins are only rarely achieved. Total pancreatectomy and pancreaticoduodenectomy, though theoretically possible, have not been described in dogs and cats with spontaneous disease. However, one report has detailed the management of dogs after experimental total pancreatectomy.141 Also, extrapolation from human patients suggests a high morbidity and mortality for these procedures.
The complicated post-surgical lifelong management of EPI and diabetes mellitus, make total pancreatectomy less than desirable.142 In human patients, the use of pancreatic surgery for the treatment of pancreatic adenocarcinoma is highly controversial and some surgeons recommend that this procedure only be undertaken by teams that perform at least 50 of these procedures per year. Chemotherapy or radiation therapy have shown little success in human or veterinary patients with pancreatic adenocarcinomas.142 Overall, the prognosis for dogs and cats with pancreatic adenocarcinoma is grave.140,142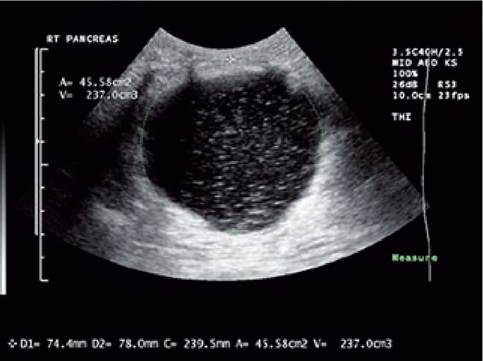
Figure 8.14.
Pancreatic pseudocyst. This image shows the ultrasonographic image of a pancreatic pseudocyst in a dog. The pseudocyst is characterized by a large almost completely anechoic structure that is associated with the pancreas. In this patient, the volume of the pseudocyst was estimated at 237 ml. (Image courtesy of Dr. Kathy Spaulding, Texas A&M University, USA.)

Figure 8.15.
Pancreatic abscess. This image shows the ultrasonographic image of a pancreatic abscess in a dog. The abscess is characterized by a large hypoechoic structure. In most cases, pancreatic abscesses are more echoic than pseudocysts. However, in some cases, an abscess and a pseudocyst cannot be differentiated ultrasonographically. In contrast to humans, pancreatic abscesses in dogs and cats are usually sterile. (Image courtesy of Dr. Kathy Spaulding, Texas A&M University, USA.)
8.2.3