Exocrine pancreatic insufficiency
Introduction and definition
Exocrine pancreatic insufficiency (EPI), as the name suggests, is a syndrome that is caused by the insufficient synthesis and secretion of pancreatic enzymes.
The most common cause of EPI is an absolute lack of pancreatic acinar cells that is due to pancreatic acinar atrophy or chronic pancreatitis (Figure 8.10). In this situation, all the pancreatic digestive enzymes are lacking. In rare cases, a single enzyme may be lacking, but the lack of a single enzyme, even if complete, most likely does not lead to clinical signs. Pancreatic lipase seems to be an exception as pancreatic lipase deficiency has been reported as a cause of clinical signs of EPI in humans and in one dog.99,100Another infrequent cause of EPI is an obstruction of the pancreatic duct by a tumor (Hill S, personal communication, 2007). Such an obstruction, if complete, can lead to a lack of digestive enzymes in the small intestinal lumen, despite normal production of these enzymes. Long-term, an obstructed pancreatic duct can lead to either pancreatitis, pancreatic atrophy, or both, which then can lead to clinical signs of EPI. The most likely cause of an obstruction of the pancreatic duct is a pancreatic adenocarcinoma or another neoplastic condition of the pancreas. Obstructions of the pancreatic duct have been described in humans but have never been conclusively demonstrated in dogs. In cats, there have been reports of pancreatic flukes, Eurytrema procyonis, causing pancreatic atrophy.101
Pancreatic aplasia and hypoplasia could, in theory, also cause clinical signs of EPI and these conditions are sometimes suspected when EPI is diagnosed at a very early age, but to date no case has been conclusively demonstrated in a puppy or kitten. The definitive diagnosis of this condition would require a diagnosis of EPI at a very young age and the demonstration of a lack of an inflammatory infiltrate and fibrosis upon pancreatic biopsy.
Etiology
The most common cause of EPI in the classical sense, that is the lack of exocrine pancreatic tissue, is pancreatic acinar atrophy (PAA), which is almost exclusively seen in German Shepherd dogs, Rough-coated Collies, and Eurasians.102,103 Several studies have suggested that PAA is inherited as an autosomal recessive trait in the German Shepherd dog and also the Eurasian.102,103 However, the search for a genetic marker for this disease has been unsuccessful despite the fact that the entire canine genome has been scanned using a set of microsatellite markers, as no mutations could be identified in several candidate genes.102 Thus, this condition may not be due to a single gene defect but may instead be multifactorial. While PAA is a hereditary disease, the associated pancreatic atrophy does not appear to be a direct consequence of this genetic disease. Instead, there have been studies to suggest that PAA is ultimately a result of immune- mediated destruction of pancreatic acinar cells.104,105
The most common cause of EPI in cats and the second most common cause in dogs is chronic pancreatitis.106 As with other organs, chronic inflammation can lead to atrophy and fibrosis, which ultimately can lead to the destruction of enough exocrine pancreatic tissue to cause clinical signs of EPI. As previously described, obstruction of the pancreatic duct can also lead to atrophy of the pancreas, but this has only been anecdotally reported in dogs and cats.
Pathogenesis
Pancreatic secretory products, and most importantly, pancreatic enzymes are crucial for the digestion and absorption of food. When pancreatic acinar cells are lacking, regardless of the cause, maldigestion occurs. It is important to note that the GI tract is a highly redundant system and for most pancreatic digestive enzymes there are other enzymes with the same function that are synthesized and secreted by other organs. For example, pancreatic lipase is crucial for fat digestion, but the stomach also synthesizes and secretes a lipase, gastric lipase, which is responsible for a significant portion of normal fat digestion in dogs.4 Also, the exocrine pancreas has a huge reserve capacity.
In humans, it has been estimated that clinical signs of EPI only ensue when more than 90% of exocrine pancreatic function have been lost.107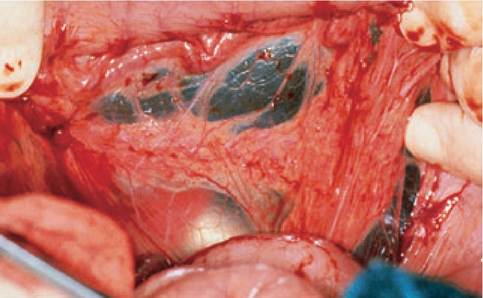
Figure 8.10:
Exocrine pancreatic insufficiency. This picture shows a pancreas in a dog with exocrine pancreatic insufficiency. There is very little pancreatic tissue left and the remaining tissue looks more fibrous than glandular in appearance.
Maldigestion leads to undigested food components in the intestinal lumen, which can lead to diarrhea, proliferation of the small intestinal microflora, and weight loss. It is important to note that these clinical signs are not solely due to maldigestion, but that the lack of functions other than the digestive functions of the exocrine pancreas may also play a role. For example, the pancreas secretes large quantities of bicarbonate, which are necessary to buffer gastric acid. A lack of bicarbonate leads to a decrease in the pH in the duodenum, which can have an effect on brush border and pancreatic enzyme activity or the intestinal microflora. In addition, the pancreas is believed to synthesize and secrete trophic factors that help maintain a normal GI mucosa and a lack of these factors may lead to malabsorption in addition to maldigestion. The exocrine pancreas also is the major source of intrinsic factor in dogs and cats.3 In sharp contrast to humans, where intrinsic factor is mainly secreted by the gastric mucosa, intrinsic factor in dogs and cats is mainly of exocrine pancreatic origin.3 In a recent study, 82% of dogs with EPI were shown to have a decreased serum cobalamin concentration with 36% having marked hypocobala- minemia.108 In another study, 65% of 20 cats with EPI were cobalamin deficient.109
Clinical presentation
EPI can be subclinical.110 In two large series of German Shepherd dogs, severely decreased serum TLI concentrations were identified in several dogs without any clinical signs.110 Some of these dogs underwent exploratory laparotomy and their pancreatic mass was found to be severely decreased.110 This once again underscores the overall high degree of redundancy of the GI tract.
The most consistent clinical sign in dogs and cats with EPI is weight loss.109-111 Loose stools are also commonly observed, but watery diarrhea is rather uncommon.109,111 Often, affected patients have a poor hair coat and dogs with EPI are commonly reported to have borborygmus and increased flatulence.111 Many dogs and cats with EPI show an increased appetite and many dogs also show coprophagia, or even pica.111 In cats, a greasy soiling of the hair coat in the perineal region can be observed (Figure 8.11A).
However, in a recent study, only 1 of 20 cats was reported to have such greasy soiling of the haircoat.109Diagnosis
A diagnosis of EPI is made based on the demonstration of a lack of exocrine pancreatic function. Various function tests have been described, including the plasma turbidity test, the PABA (para-aminobenzoic acid) test, the fecal test for undigested starch and muscle fibers, or the fecal proteolytic activity (FPA) test.112 With the exception of the FPA test, all of these tests are only indirect measures of exocrine pancreatic function, estimating the digestive capacity of the entire GI tract rather than just the function of the exocrine pancreas. The FPA test is slightly different in that the major proteolytic activity of the feces should in fact be based on the presence of two pancreatic enzymes, namely trypsin and chymotrypsin. However, false positive and false negative test results have been observed. Also, there are different methods for testing FPA.112 The most simple one is the use of a piece of undeveloped radiographic film. In theory, the digestive enzymes in the fecal sample digest the starch in the radiographic film creating a halo. Unfortunately, this method is extremely unreliable and should not be used. Other methods to determine the FPA are more reliable, but are still flawed by many false test results. Thus, FPA can only be recommended for those species in which other, more reliable, diagnostic modalities are not available.
Another approach to estimating exocrine pancreatic function is to measure the amount of pancreatic enzymes or zymogens in the blood or feces. Serum lipase activity was not significantly different between dogs with EPI and healthy dogs.55 This is most likely due to the fact that many cells from different cellular origins synthesize and secrete lipases, and a lipase activity assay cannot differentiate between these lipases. Serum trypsin-like immunoreactivity (TLI) is the gold standard for the diagnosis of EPI in both dogs and cats.109,113 The TLI assay is highly species-specific and measures the mass concentration of cationic trypsinogen, cationic trypsin, and some cationic trypsin molecules bound to proteinase inhibitor molecules.
Under physiological conditions, only a small amount of the trypsinogen synthesized by pancreatic acinar cells is released into the vascular space. Trypsinogen and trypsin are rather small molecules and thus get quickly excreted by the kidney. Therefore, only if the pancreas is functioning normally can a small amount of trypsinogen be detected in the serum. In contrast, in patients with EPI, regardless of the cause, the amount of trypsinogen released into the serum, and in turn serum TLI is severely decreased to undetectable. In general, serum TLI is highly sensitive and specific for the diagnosis of EPI in both dogs and cats. There are two special scenarios, however, where serum TLI can be normal despite the patient having EPI. The first scenario is isolated pancreatic lipase deficiency. It has long been recognized that the rate-limiting enzyme of pancreatic digestion is pancreatic lipase. Thus, patients with an isolated lipase deficiency may have clinical signs of EPI but still have a normal serum TLI concentration. Recently, the first dog with such an isolated lipase deficiency has been reported, but such cases are believed to be extremely rare.100 Another scenario where serum TLI concentration could be normal in a patient with EPI is a patient with an obstructed pancreatic duct. Such cases have not yet been described in the literature, but recently a single dog with this condition has been identified (Hill S, personal communication, 2007). Again, this scenario is believed to be extremely rare.Recently, assays for the measurement of serum pancreatic lipase immunoreactivity (PLI) in dogs and cats have been developed and validated. The PLI assay is highly species-specific and measures the mass concentration of pancreatic lipase in the serum. Pancreatic lipase is much larger than trypsinogen and is also positively charged. Pancreatic lipase is, thus, repelled from the glomerular membrane and is only very slowly excreted by the kidneys. As a consequence, a larger residual amount of pancreatic lipase remains in the vascular space and the assay is thus less sensitive for EPI.
This has recently been demonstrated in a study with 25 dogs with EPI, as the serum cPLI concentrations showed a larger overlap with healthy control dogs than did serum cTLI concentrations.55 Because PLI assays have been shown to be the superior test for pancreatitis, PLI assays have now been optimized for measurement of normal and increased concentrations and are no longer suited for the measurement of decreased concentrations, as would be seen in patients with EPI.A fecal assay for the measurement of pancreatic elastase has been developed and is now marketed in Europe. The initial studies showed an acceptable sensitivity and specificity of the assay.114 However, the estimated positive predictive value was less than 60%.115 In another study, fecal elastase concentration was shown to be associated with a high number of false positive test results.116 In this latter study, 6 of 26 dogs with a severely decreased fecal pancreatic elastase concentration were shown to have a normal serum cTLI concentration.116 It is interesting to note that the dogs with a false positive test result for EPI had a significantly lower serum CCK concentration than did dogs with a true positive test result.117 This may suggest that patients with chronic small intestinal disease may have fewer neuroendocrine cells in their intestinal mucosa,
leading to a decreased stimulation of pancreatic secretion, which may in turn be associated with false positive fecal pancreatic elastase concentrations. A high rate of false positive test results of fecal elastase concentration has also been observed in human patients. Thus, if fecal pancreatic elastase concentration is to be used for the diagnosis of EPI, any positive result must be verified by measurement of a serum cTLI concentration.
Therapy
Digestive enzyme replacement therapy is the mainstay of therapy for EPI.106,118 Pancreatic enzymes can be replaced by a variety of different options.119 Dried pancreatic extract from beef or pork pancreas is by far the most common and effective means of pancreatic enzyme replacement. Therapy is started with 1 teaspoon of dried extract per 10 kg body weight and meal. After the patient has responded completely to the therapy, the dose can be slowly decreased until a minimally effective dose has been reached. It is important to note that the content of enzyme activity in the product used may vary from container to container and thus the minimally effective dose may vary slightly over time. Pancreatic enzymes are also available as tablets and capsules but studies in humans and dogs have shown that powder is preferable to other formula- tions.119-122 In a recent study, 3 of 25 dogs treated with pancreatic enzyme supplement developed oral bleeding.123 When this occurs, a coagulation profile should be evaluated to exclude a vitamin K-responsive coagulopathy, which has been reported in a single cat with EPI.124 In the case of a normal coagulation profile, the dose of pancreatic enzymes should be lowered. Two dogs in the study cited above continued to do well on the lower dose, but in one of the three dogs the clinical signs did return.123 If a patient refuses to consume the pancreatic powder mixed into their food or in the rare case of a food allergy to the pancreatic powder, fresh raw pancreas from various species can also be used.119 Beef, pork, sheep, or game pancreas have all been used. Thirty to 90 g (approximately 1-3 ounces) of raw pancreas replace 1 teaspoon of dried pancreatic extract. The pancreas should be divided into portions for one meal each and frozen. The frozen pancreatic tissue maintains its enzymatic activity for long periods of time. Concerns have been raised about the potential threat of infectious contamination of raw frozen pancreas. Theoretically, raw bovine and ovine pancreas carries the risk of BSE transmission and raw porcine pancreas carries the risk of transmission of Aujeszkys disease. However, this risk is more or less academic as dried pancreatic powder would carry exactly the same risk. Game and ovine pancreas can be infested by Echinococcus spp. and infestation with this parasite could potentially cause significant disease and even death. These risks should thus be discussed with the owner before initiating therapy. Pre-incu- bation of the food with the pancreatic extract does not appear to be necessary to achieve a therapeutic response.120
Feeding of a low fat diet to EPI patients has been recommended by some authors. However, experimental studies have shown that in dogs treated with pancreatic supplements, fat digestibility does not return to normal, suggesting that fat restriction would increase the risk of deficiencies of fat-soluble vitamins and essential fatty acids.120 One study did not show any benefit of a fat-restricted diet in dogs with EPI.108 In addition, two other studies on dogs with EPI did not reveal any significant effect of diet on treatment success.125,126 As a consequence, the author believes that a high-quality maintenance diet should be used. However, diets with a high fiber content should be avoided as dietary fiber may interfere with fat absorption.
As mentioned above, many patients with EPI are cobalamin deficient and thus every dog and cat with EPI should be evaluated for possible cobalamin deficiency. If cobalamin deficiency is identified, cobalamin supplementation should be added to the management of the patient. Cobalamin is a water-soluble vitamin that must be administered parenterally in deficient patients. The exact dose requirements for dogs and cats are unknown, but over-supplementation with cobalamin is not associated with side effects; thus, relatively high doses of cobalamin are chosen. In cats, a dose of 150-250 μg is given per subcutaneous injection based on the size of the animal. In dogs, a dose of 250-1200 μg SC is given based on the size of the animal. Doses are given weekly for 6 weeks, then every other week for 6 weeks, followed by one more dose after a month and a recheck of serum cobalamin concentration a month later. Most EPI patients that have been treated appropriately will have a normal or even supranormal serum cobalamin concentration at the time of re-evaluation and the cobalamin supplementation can be discontinued.
Serum concentrations of most fat-soluble vitamins have been shown to be decreased in dogs with EPI and can also be assumed to be decreased in cats.125 However, systematic vitamin supplementation of fat-soluble vitamins has not been investigated in these patients and over-supplementation with these types of vitamins may cause side effects. Anecdotal reports of vitamin E supplementation (400-500IU PO q 24 h for 1 month) are available, but the beneficial effect of such therapy has not been evaluated.
Many patients with EPI will respond well to enzyme replacement therapy and cobalamin supplementation if indicated. However, a small group of patients does not respond adequately to standard therapy. The potential causes of treatment failure should be evaluated. The type, formulation, and dose of the enzyme supplement should be reviewed and if there is any suspicion that the enzyme replacement may be insufficient, the protocol should be adjusted accordingly. Also, patients should be evaluated for concurrent conditions, such as IBD, diabetes mellitus, or SIBO. Diabetes mellitus can be observed in patients with an underlying chronic pancreatitis as the re-
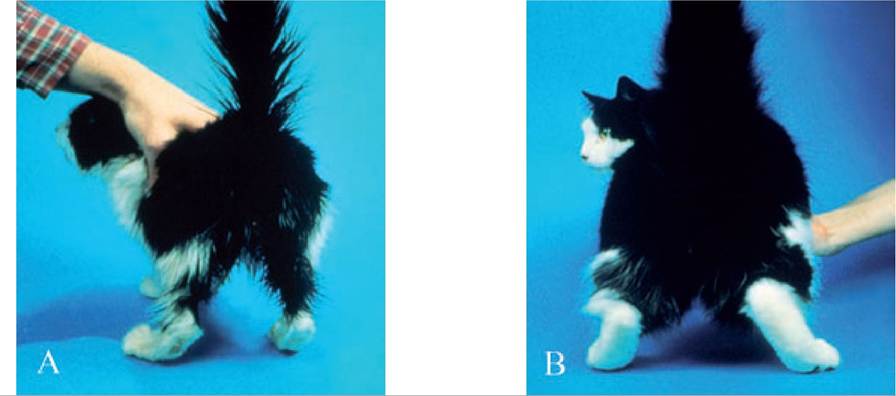
Figure 8.11:
Exocrine pancreatic insufficiency. This picture shows a cat with exocrine pancreatic insufficiency. Panel (A) shows the cat before initiation of therapy. The cat has lost a significant amount of weight and has a poor hair coat. In addition, there is greasy soiling of its hair coat in the perineal region. Panel (B) shows the same cat after treatment with pancreatic enzyme supplementation. (Images courtesy of Dr. David A. Williams, University of Illinois, USA.)
suiting atrophy does not spare the pancreatic islet cells. Therapy of the concomitant diabetes mellitus is necessary in such patients.
If there is no evidence of any concurrent disease, a therapeutic trial with an antimicrobial agent can be attempted. It has previously been reported that dogs with EPI commonly also have SIBO and treatment for SIBO is benign.127 The treatment of choice is tylosin (Tylan powder at 25 mg/kg PO q 12 h for 6 weeks), but other antibiotic agents, such as metronidazole or oxytetracycline can also be used.
If patients still do not respond, antacid therapy can be attempted. A large portion of the orally-administered pancreatic lipase is destroyed by the low pH in the stomach.128 By increasing the pH in the stomach, this portion may be decreased and the therapeutic response may be improved. However, it also needs to be noted that while an increase in gastric pH will decrease the amount of pancreatic lipase being destroyed during its passage of the stomach, it also will increase the amount of gastric lipase being destroyed and the final result may not lead to a significant change in lipid digestibility. A trial with antacids can be attempted to overcome this problem. H2 antagonists can initially be tried, but human EPI patients treated with omeprazole showed a superior response over patients treated with H2 antagonists.129
If none of these measures lead to control of the clinical signs, a decrease in the dietary fat may be effective. However, as mentioned above, feeding a low fat diet may be associated with complications and should only be viewed as a last resort.
Prognosis
EPI is usually a life-long condition as pancreatic acinar cells can generally not regenerate. Having said this, there are anecdotal reports of isolated cases of resolving EPI.
Most dogs and cats with EPI can be successfully managed and will have a normal quality of life and a normal life expectancy (Figure 8.11B). A recent study has evaluated the prognostic factors for dogs with EPI.108 The only factor associated with a poor outcome in this study was the presence of concurrent cobalamin deficiency.108 As a consequence, the author strongly believes that serum cobalamin concentration should be determined in small animal patients with EPI.
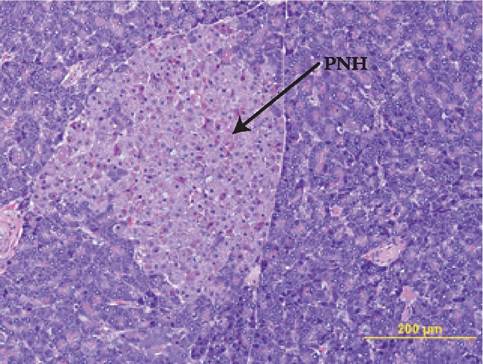
Figure 8.12:
Pancreatic nodular hyperplasia. This figure shows the histopathological appearance of pancreatic nodular hyperplasia (PNH) in a dog. This finding of a proliferation of well-differentiated pancreatic epithelial cells is very common in dogs and cats. In dogs, the presence of pancreatic hyperplastic nodules has been associated with age. (H&E, 20?; image courtesy of Dr. Shelley Newman, University of Tennessee, USA.)
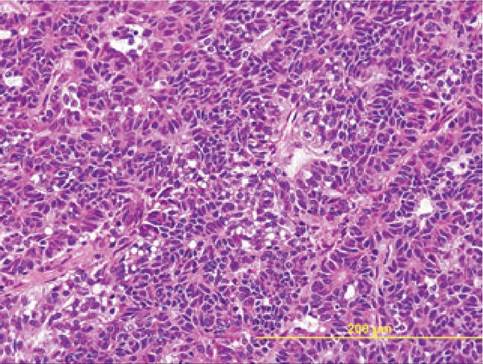
Figure 8.13:
Pancreatic adenocarcinoma. This image shows the histopathological characteristics of an adenocarcinoma in a cat. Please note the disorganized clusters of acinar cells that are characterized by variation in nuclear and cytoplasmic size, prominent nucleoli and occasional mitotic figures. (H&E, 40?; image courtesy of Dr. Shelley Newman, University of Tennessee, USA.)
8.2.2
More on the topic Exocrine pancreatic insufficiency:
- exocrine PANCREATIC INSUFFICIENCY
- Exocrine pancreatic insufficiency
- Laboratory tests for the diagnosis of exocrine pancreatic disorders
- References
- german shepherd DOG ENTEROPATHY
- Contents
- Preface
- Index
- History of specific gastrointestinal signs
- Abbreviations