Feeding Pregnant Goats
During gestation goats accumulate protein, fat, minerals, and vitamins beyond what is incorporated into fetuses and placenta. The magnitude of this net bw gain varies from less than 1 to 8 kg and is strongly influenced by the level of nutrition.
Protein, but not energy, is accumulated more efficiently during gestation than when the goat is not pregnant.Of the weight of the kid, 70% is acquired between the 100th day of gestation and parturition. The weight of kids at birth as a percent of the doe's weight at breeding is twice the corresponding ratio of calf to cow. Undernourishment during late pregnancy results in the birth of smaller kids that will in turn show increased mortality and slower growth rates (Bajhau and Kennedy 1990). Subsequent milk production will also be compromised (Sahlu et al. 1995). Particularly important is the potential adverse effect of an energy-deficient diet on colostrum in the udder at delivery, as demonstrated in ewes (Banchero et al. 2006). The kids may die of hypothermia or starvation before adequate colostrum is produced by the dam. A protein deficiency must also be avoided.
If the doe is carrying multiple kids, especially three or more, then it will have to mobilize its fat reserves just before parturition to meet its own energy needs. This is because appetite often drops off at this time and the volume of the gravid uterus and of internal fat stores limits the volume of feed that can be consumed. When propionate supplies are inadequate, the acetate coming from mobilization of fat will be transformed into ketone bodies. Pregnancy toxemia may result, as discussed below.
A high-quality, palatable hay should be fed during pregnancy. This permits limiting the grain to 200 g/day late in gestation. Goats that eat a lot of hay during gestation maintain that ability to ingest increased levels of roughage during lactation.
Also, high concentrate consumption in pregnancy has been associated with slow parturition and poor cervical dilation and with poor persistence of lactation (Morand-Fehr et al. 1974). More recent reports suggest that protein should be fed to dairy goats at approximately 11.5% of ration DM during late gestation for fetal well-being (Sahlu et al. 1992) and for subsequent milk production (Sahlu et al. 1995), and supplying 14% crude protein did not improve performance. A supplement rich in rumen bypass protein is desirable at this time (Morand-Fehr and Sauvant 1988).An experiment with a small number of late-pregnant goats showed that they were capable of increasing DMI and protein in the diet at this stage. In the last weeks before parturition, if allowed to choose from several hays and concentrates offered free choice, the goats increased their forage and protein intake by increasing consumption of alfalfa hay and chickpeas, while decreasing grass hay and barley consumption. In the same study, goats fed only alfalfa hay and flaked barley increased their DMI by the substitution effect of increasing consumption of the concentrate and protein consumption by eating only the more digestible portions of the hay (Fedele et al. 2002).
Abortion
Abortion as the result of inadequate nutrition has received the most attention in the Angora breed. Small, poorly grown animals or old does are most prone to abort. During inclement weather or after shearing, ad lib supplementation with whole grain treated with an alkali and ionophore prevents the spate of abortions that normally follows such stressful conditions, without causing rumen acidosis (Wentzel 1987). Lime, ionophore, and as much as 1.2% urea are mixed with molasses and water, then poured over whole grain and mixed in well. The final product contains 2% (by weight) slaked lime (calcium hydroxide, not calcium carbonate or field lime) and 20 mg/kg ionophore such as rumensin, salinomycin, or lasalocid. According to one recipe (Van der Westhuysen et al.
1988), 12.5 kg calcium hydroxide, 8 kg urea, 16 L molasses, and the appropriate amount of ionophore are mixed with 20 L of water, then poured over 560 kg of grain.Native breeds are often observed to be less apt to abort than imported animals, especially dairy breeds, with higher nutritional demands (Mellado et al. 2006). It is difficult to separate the adverse effects on the placenta and fetus of nutritional deficiencies in high-producing goats from lack of resistance to enzootic abortion diseases. However, within a herd in which feed or manger space is limited, the smaller, younger pregnant does whose nutritional needs cannot be met in the face of competition with mature, socially dominant adults are prone to abortion. Feeding these animals as a separate group alleviates the nutritional and social stresses.
Mineral and vitamin deficiencies and toxic plants that have been associated with abortion are reviewed in Chapter 13.
Pregnancy Toxemia
Goats are at risk of developing the metabolic condition termed “ketosis” at two stages: at the end of gestation (pregnancy toxemia) and during early lactation (i.e., lactational ketosis, as discussed later).
Etiology
Inadequate nutrition during late gestation is central to the development of pregnancy toxemia. Pregnancy toxemia is usually limited to the last six weeks of gestation, although one Indian study detected ketonuria in 3% of 120 inappe- tent lethargic does in the third month of pregnancy. By comparison, 24% of 160 does with a similar presentation in the fifth month of pregnancy were positive for acetoacetate in the urine (Lalitha et al. 2001). Its immediate causes can be crudely divided into undernutrition and overnutrition. In starvation ketosis, the animal has not been permitted access to enough nutrients, especially energy, to meet the demands of itself and its (usually) multiple fetuses. Low- quality roughage is a particular risk, because not enough can be consumed to meet requirements when the volume of the rumen is reduced by the presence in the abdomen of a large uterus (Bostedt and Hamadeh 1990).
Secondary ketosis is similar, except that some other disease temporarily interferes with feed consumption by an otherwise properly fed doe. In overnutrition (“estate”) ketosis, the goat has been overfed until its massive internal fat stores plus the full uterus occupy so much of the body cavity that DMI is severely curtailed at a time when increased energy consumption is required. Leptin, a hormone produced by adipose cells, may also contribute to a reduction in feed intake by decreasing the obese animal's appetite (Kolb and Kaskous 2004).Excessive grain feeding itself can lead to pregnancy toxemia, because the goat that eats inadequate roughage is apt to go off feed at this critical time. When goats are heavily fed on corn silage in late gestation they become obese. Their level of ingestion then decreases dramatically before parturition. Rumen acidosis from energy-rich silage may contribute to the development of pregnancy toxemia.
Figure 19.5 shows various determining factors for ketosis (Sauvant et al. 1984). Low energy intake in late gestation increases the risk of pregnancy toxemia. High energy intake at this time increases the risk of lactational ketosis, as does low energy intake at the beginning of lactation. Etiologic factors involved in the development of pregnancy toxemia have been reviewed (Sauvant et al. 1991a).
Pathogenesis
The central metabolic events are fat mobilization and the availability of glucose (Caple and McLean 1986; Herdt and Emery 1992). Pregnancy toxemia is typically more common than lactational ketosis and occurs predominantly in “improved” breeds with high prolificacy. It is not a disease expected to occur in native breeds carrying a single kid under extensive management conditions. With proper management and nutrition, even the doe carrying quadruplets can remain clinically healthy, although concentrations of ketone bodies in the blood can be expected to be higher in those goats carrying large litters. In a study of 514 native goats managed under a semi-intensive pasture and concentrate system in India, no clinical ketosis was observed, but about 10% of the animals had subclinical ketosis based on laboratory findings of hypoglycemia (4.5 mg/ dL ketones) (Gupta et al.
2007).The developing fetuses depend upon glucose (maternal hepatic gluconeogenesis) for their energy needs. Ketone bodies and free fatty acids do not cross the placenta in any substantial quantities (Reid 1968). Insulin resistance occurs and insulin levels in the late-pregnant doe are also decreased; this spares glucose for fetal needs while at the same time stimulating lipolysis and gluconeogenesis. Placental lactogen levels are greatly increased when multiple fetuses are present (Sardjana et al. 1988). Placental lactogen has growth hormone as well as prolactin activity, and is probably crucial to meeting the metabolic needs of the fetuses at the expense (if necessary) of the dam. Thus, the late-pregnant doe is often subclinically ketotic and decreased glycogen stores in the liver may lead to hypoglycemia.
Clinical Signs
The early signs of pregnancy toxemia are vague. They probably originate from decreased glucose utilization by the doe's brain. The goat may be slow to get up or may lie off in a corner. Increased lying time has been documented (Zobel et al. 2015). It eats less and its eyes are dull. There is often a noticeable subcutaneous edema of the lower limbs. Teeth grinding and generalized weakness progress to more apparent neurologic abnormalities (blindness, loss of menace response, star gazing, nystagmus, ataxia, tremors), then to coma. Bloat and frothy salivation have also been reported in some animals (Vasava et al. 2016). The fecal output is reduced to a few small, dry, mucus-coated pellets.
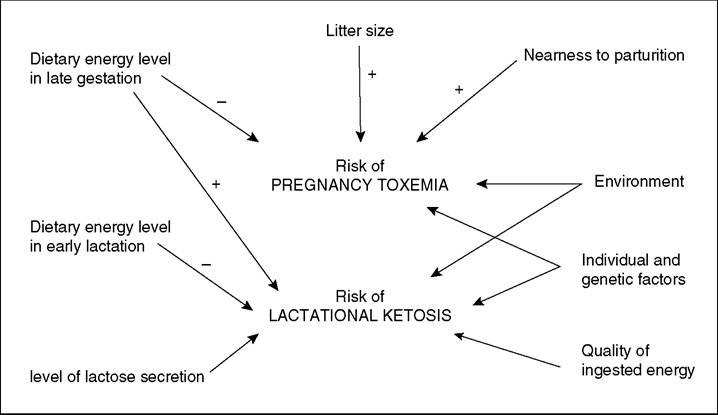
Figure 19.5 Factors determining the development of ketosis in dairy goats. Source: Sauvant 1984 / Institut National de la Recherche Agronomique.
As metabolic acidosis develops the animal may breathe more rapidly. Thus, advanced primary ketosis may be difficult to distinguish from a primary pneumonia that has caused the goat to go off feed and develop a secondary ketosis.
A careful physical examination is also necessary to identify other problems such as parasites, lameness, and bad teeth that might have contributed to the animal's present state.In the terminal stages of pregnancy toxemia, the doe becomes recumbent. Death of the fetuses at this stage releases toxins and hastens the demise of the doe. Pulse and respiratory rates increase. The course of the untreated disease varies from 12 hours to 1 week.
Laboratory Tests
There are three major ketone bodies produced in the course of this metabolic disease: beta-hydroxybutyrate (BHB), acetoacetate, and acetone. In the past, these were sometimes measured together in a poorly defined way and reported as total ketones. Currently BHB, which is the most stable ketone in blood and accounts for approximately 85% of the total ketones in sheep with pregnancy toxemia (Bostedt and Hamadeh 1990), receives the most attention in the laboratory.
Some people can detect an odor of ketones on the breath of ketotic animals. Others must depend on simple diagnostic reagents or laboratory tests. In the early stages of pregnancy toxemia, ketone bodies are easily detectable in the urine. The commonly used test strips and pills containing nitroprusside (Rothera reagent) turn purple in the presence of acetoacetate, but react minimally with acetone and BHB. If the doe has only a trace ketonuria (physiologic when late pregnant with multiple fetuses), some other cause for its illness should be sought, but supportive treatment to prevent worsening of the ketosis should be given. Late stages are usually accompanied by renal failure; marked proteinuria, epithelial casts, and ketonuria are present (Kaufman and Bergman 1978). The veterinarian should have a collection cup close at hand whenever examining a late-pregnant goat. A doe often urinates when it first stands up on the approach of a stranger, as part of preparing for flight. If urination has not yet occurred by the end of the examination, then occluding the nostrils while an assistant holds the cup under the goat's vulva may be tried. However, even healthy goats rarely urinate in response to this stimulus, and the toxemic animal is typically dehydrated. The attempt must be abandoned before the goat is asphyxiated.
When urine is not available, plasma or serum can be checked with the ketone pills, powders, or strips. Recently, with the advent of hand-held meters for testing human blood for BHB and glucose, precise BHB testing on farm has become possible. The test strips are inexpensive and the results determined rapidly. For conversion to other units, note that BHB in mmol/L ? 10.4 = BHB in mg/ dL. Initially reference values established for sheep (Clarkson 2000) were used, but now the hand-held meters have been validated for testing BHB in goats (Dore et al. 2013; Pichler et al. 2014). In a subsequent study (Dore et al. 2015), 1081 dairy goats in Quebec were sampled during the last five weeks of pregnancy using the Precision Xtra™ meter (Abbott, Columbus, OH, USA). At four and five weeks prepartum, the optimum BHB threshold for predicting clinical pregnancy toxemia (maximum sum of sensitivity and specificity) was ≥0.4 mmol/L, which is equivalent to 4.16 mg/dL. In the last week prepartum the optimum threshold was ≥0.9 mmol/L (9.36 mg/dL). The optimum thresholds for predicting mortality when sampled at four weeks and one week prepartum were ≥0.6 and ≥1.4 mmol/L (6.24 and 14.6 mg/dL). In general, and allowing for the low specificity of these thresholds, BHB values less than 1 mmol/L can be considered normal, values of 1.5-3 mmol/L can be considered indicative of severe undernutrition, and animals with pregnancy toxemia often show a BHB concentration greater than 3 mmol/L. Some authors use BHB values above 1.7 mmol/L as indicative of pregnancy toxemia (Zobel et al. 2015). Ear vein blood gives slightly lower values of BHB than jugular vein blood from the same animal, but is also suitable for testing (Pichler et al. 2014). If the animal is recently dead, aqueous humor or cerebrospinal fluid can be tested instead of blood (Scott et al. 1995), but the accuracy of the hand-held meters using these fluids has not been established.
Other laboratory tests are not commonly performed on field cases of pregnancy toxemia. Cortisol-induced changes in the hemogram (neutrophilia, lymphopenia, eosinope- nia) and evidence of dehydration (elevated hematocrit and total protein) can be expected, although the total protein may be reduced by parasitism or malnutrition. Calcium is commonly decreased and alanine aminotransferase (ALT or SGPT) and aspartate aminotransferase (AST or SGOT) are typically increased (Vasava et al. 2016). Blood glucose levels are variable; severe hypoglycemia or terminal marked hyperglycemia are both possible (normal range 50-75 mg/dL; see Chapter 11). Blood pH is typically low, averaging 7.1 in does with pregnancy toxemia compared with 7.4 in control does (Lima et al. 2012).
Prognosis
The prognosis for goats with clinical pregnancy toxemia is poor. Goats with recumbency or anorexia and absent gastrointestinal motility have a poor prognosis for survival (Lima et al. 2016b), although in another study recumbency was not associated with failure to survive in goats receiving intensive in-hospital treatment. In that case series of 56 mostly Boer does, 39 (70%) survived to discharge, and elevated BUN and low serum bicarbonate were associated with failure to survive (Simpson et al. 2019). A case fatality rate in dairy goats of 86% was reported by Lima et al. (2012) in a series of 22 does treated on farm. Low blood pH was a negative prognostic indicator, with a mortality of 100% in 11 does with a blood pH of 7.122 or lower in this study.
Goats with pregnancy toxemia that do not die tend to have dystocias and higher kid mortality. They do not come to milk well. Similar problems are noted in obese goats, even when clinical pregnancy toxemia does not occur; in addition, these animals are at high risk of developing lactational ketosis.
Necropsy Findings
The doe that dies of pregnancy toxemia usually has multiple fetuses in the uterus, unless these were removed just before death. The fetuses may be fresh or decomposed. The doe's liver is enlarged and yellow because of infiltration with fat (Tontis and Zwahlen 1987). The doe's adrenal glands are enlarged. The carcass appears dehydrated. If urine remains in the bladder, it shows a strong ketone reaction. There is typically poor rumen fill and often there is abundant mesenteric fat, in the animals where obesity was a contributing factor.
Treatment
The treatment and prognosis depend on the stage of the disease. In the earliest clinical form, the goat readily eats offered grain. Its diet should be improved to include betterquality roughage and increased concentrates. Propylene glycol is given orally by dosing syringe, at the rate of 60 mL two or three times daily as a glucose precursor. Although some authors suggest as much as 175-250 mL of propylene glycol two to four times a day (Bretzlaff et al. 1991a; LeValley 2010), this dosage seems excessive and likely to overwhelm the ability of the rumen flora of an already sick goat to digest it. Overdoses of propylene glycol can be fatal, creating plasma hyperosmolality that impairs neurologic function. A commercial product that contains niacin as well as propylene glycol has been recommended, or the goat can be injected with enough mixed B vitamins to supply 1 g of niacin/day (Bowen 1998). Calcium borogluco- nate (60 mL of a 23-25% solution) is given subcutaneously to counteract any concurrent hypocalcemia; approximately 20% of sheep with pregnancy toxemia are also hypocalcemic (Kolb and Kaskous 2004). Some authors have recommended 3-4 L of oral rehydration fluids containing dextrose and electrolytes (LeValley 2010; Brozos et al. 2011), or corn syrup in place of propylene glycol. Other authors recommend the use of insulin, up to 40 units of protamine zinc insulin twice daily subcutaneously (Matthews 1999), but this treatment is expensive and may compromise the fetuses.
If the animal is unwilling to eat or to rise, the prognosis is guarded and immediate euthanasia may be the best approach (Brozos et al. 2011; Lima et al. 2012). Intravenous glucose (25-50 g, preferably as a 5-10% solution), mixed B vitamins, and force feeding are often added to the regimen. One author has suggested giving 5-7 g glucose as a 50% solution six to eight times a day via an indwelling jugular catheter (Marteniuk and Herdt 1988). However, it has been shown that obese goats with pregnancy toxemia are not only insulin resistant, but also glucose intolerant (Lima et al. 2016a); intravenous glucose does not appear to help these animals and may even be detrimental. If the goat is breathing rapidly, acidosis is likely and intravenous therapy should be extended to 3-4 L of fluid including 15 g or more of sodium bicarbonate. It has been determined that the blood pH and the BHB concentration are poorly correlated in goats with pregnancy toxemia (Lima et al. 2016a), so the decision to give sodium bicarbonate is not based on the BHB test result. Antibiotic therapy is begun for primary or secondary pneumonia and flunixin meglumine is commonly administered. Flunixin meglumine has been reported to stimulate movement and appetite of sheep with pregnancy toxemia (Zamir et al. 2009).
If the goat is known to be within one week of its due date, hormonal induction of parturition (see Chapter 13) with 10 mg of prostaglandin F2 alpha will end the energy drain to the fetuses, as well as increase the likelihood that live kids will be obtained (Lima et al. 2016b). If the due date is uncertain and the owner desires to save doe and kids, 20-25 mg dexamethasone may be preferred for its gluconeogenic effects and beneficial stimulus to appetite. Late-gestation fetuses are born within approximately two days after corticosteroid administration, while more immature fetuses are not always aborted, but may instead be carried to term successfully if the doe responds to medical management. Daily administration of this dose of dexamethasone may eventually induce delivery of the immature fetuses if the doe lives long enough. If possible, transabdominal ultrasound examination of the uterus for evidence of fetal movement or heartbeat should be performed to verify that the fetuses are still alive. Dexamethasone induction requires a live fetus, and slaughter or euthanasia may be more appropriate in commercial situations if the kids are already dead.
If the valuable goat is down and very depressed or has failed to improve by the day after initiation of treatment, then a cesarean section should be performed immediately. This increases the chances for live kids, although the doe is still likely to die (Lima et al. 2016b). Severely toxemic animals do not kid rapidly or dependably after receiving hormones, but dexamethasone on the first visit may prepare the lungs of marginally immature kids and thereby increase their chances of surviving a cesarean operation that can be delayed for 24 hours. Even with surgery and extensive fluid therapy, the prognosis is poor for survival of the recumbent goat in the late stages of pregnancy toxemia. The kids from these does also frequently are delivered dead or die within a few hours of surgery. They will require colostrum administration, often by stomach tube (see Feeding Newborn Kids, below) and intensive care to survive, as will kids delivered vaginally from does with pregnancy toxemia (Weaver et al. 2021).
Prevention
Pregnant goats should ideally have a condition score of 3 to 3.5 out of 5. If goats are already obese when the last trimester is reached, it is too late to propose a weight-reducing diet. Instead, animals must be fed high-quality roughage and as much as 500 g of concentrate daily. Any conditions that disturb the comfort of the goat, such as lack of exercise, poor ventilation, or drafts, should be corrected. This means that the stall should be dry, well bedded, and uncrowded. The goats should be let loose for at least two to three hours per day. Timid does and slow eaters should be housed separate from dominant, aggressive animals that might drive them away from the feeder. If fetal numbers have been determined by real-time ultrasonography (see Chapter 13), the goats can be grouped and fed according to litter size. Goats carrying three or more fetuses should receive the best-quality roughage available in addition to adequate concentrate.
When one doe develops pregnancy toxemia, the diet of the rest of the herd must be evaluated and corrected as necessary. Concentrates should be introduced gradually and under strict control, to avoid indigestion. It is unrealistic to expect a large herd of commercial goats to be totally free of pregnancy toxemia. Routine monitoring of all late-pregnant does for urinary ketones is also unrealistic. Healthy does carrying large litters can be expected to excrete small quantities of ketones, yet do not need treatment. Drenching with prophylactic propylene glycol (60 mL orally twice a day) is in itself a stress to a goat and should be reserved for those showing abnormal behavior or diminished appetite. If parasite control measures in the herd have been deficient, anthelmintic treatment of other pregnant does may be needed, as described in Chapter 10.
Some authors have recommended supplementing ruminant diets with niacin to help protect against the development of a ketotic state. Niacin (nicotinic acid) is antilipolytic and causes blood glucose and insulin to increase (Herdt and Emery 1992). There are anecdotal reports that 500 mg niacin/454 g of grain fed works well for preventing pregnancy toxemia in goats (Bowen 1998). Published research documenting a beneficial effect of feeding niacin appears to be lacking in goats, but the practice does not appear to carry any risks.
Parturient Paresis (Milk Fever), Hypocalcemia
Although various authors, especially in lay publications, talk about the occurrence of milk fever in goats, this condition is apparently rare (Linzell 1965; Kessler 1981).
Pathogenesis
Parturient paresis is a failure of calcium homeostasis, which depends in turn on intestinal absorption and skeletal reserves. Intestinal absorption requires calcium-binding protein. The synthesis of this transport protein is controlled by vitamin D3 availability (Sauvant et al. 1991a).
There is a sudden increase in calcium and phosphorus requirements at the onset of lactation, and the capacity for intestinal absorption of calcium increases more slowly than the requirement. Normal parturition in goats is accompanied by mild hypocalcemia. For instance, six healthy Alpine goats had an average plasma calcium concentration of 6.6 mg/dL three days after parturition, compared with 8.4 mg/dL six days before and six days after kidding (Barlet et al. 1971). In another intensive study of healthy goats (six Saanens and one Alpine), plasma calcium concentrations as low as 6.7 mg/dL were encountered (Linzell 1965), but the timing of this sample relative to parturition was not reported. When the hypocalcemia is extreme, milk fever can be expected to occur.
High-producing dairy goats occasionally develop a severe hypocalcemic syndrome clinically similar to milk fever, except that the goat is one to three or more weeks after parturition (Barlet et al. 1971; 0verby and 0degaard 1980; 0degaard and 0verby 1993). The tendency of goats undergoing a high degree of lipid mobilization to have a significant increase in calcium and phosphorus content of their milk may be involved (Sauvant et al. 1991a).
Of 40 Norwegian goats with hypocalcemia, 7 were pre- partum (two more than a week before kidding), 10 were affected during kidding or the first day after kidding, 8 more were within three weeks after kidding, and 15 were more than three weeks into lactation. Older goats were affected; 34 of 40 were starting their fourth or later lactation (0degaard and 0verby 1993).
Clinical Signs
Signs include a decrease in appetite, mild bloat or constipation, unsteady gait, and weakened uterine contractions, then an inability to rise and a decreased body temperature (Guss 1977; 0verby and 0degaard 1980; 0degaard and 0verby 1993). Affected goats are often somnolent and lie in sternal recumbency with the head turned back along the side of the body. Occasional goats lie in lateral recumbency, showing muscle spasms and screaming. There may be mucus at the nostrils or signs suggestive of pulmonary edema.
In 40 Norwegian goats diagnosed as clinically hypocalcemic, the average plasma calcium concentration was 3.75 mg/ dL (range 2.9-5.1), compared with an average of 9.91 mg/dL in 36 normal goats (0verby and 0degaard 1980). In an Indian study of nine mature goats of various breeds, in which the clinical signs of hypocalcemia were not described but diagnosis was based at least in part on response to therapy, the average calcium concentration was 6.66 mg/dL (Vihan and Rai 1984). Uterine involution after parturition may be slowed in hypocalcemic does (Bayoumi et al. 2021).
Treatment
The recommended therapy for either periparturient or lactational hypocalcemia is slow intravenous infusion of 50-100 mL of 23% calcium borogluconate. Rapid response to calcium therapy confirms the diagnosis if laboratory testing is not available. Additional calcium is sometimes administered subcutaneously or oral milk fever preparations are given. Calcium chloride gels should be avoided because of the risk of severe mucosal damage. Owners sometimes feed flavored calcium carbonate antacid pills to their does as a further calcium supplement, although this form of calcium is poorly absorbed until it is dissociated by acid in the abomasum (Thilsing-Hansen et al. 2002).
Most authors agree that the best response is achieved with early treatment. On the other hand, periparturient goats with clinical signs of excitability, posterior paresis, and constipation may not respond to calcium infusions (Kessler 1981). Perhaps some of the goats diagnosed as having milk fever are in fact victims of rumen acidosis caused by inadequate roughage consumption in late pregnancy.
Prevention
In dairy cattle, the avoidance during late pregnancy of feeds rich in calcium, such as alfalfa hay, was long considered central to preventing milk fever. More recent work in both cattle (Oetzel et al. 1988; Thilsing-Hansen et al. 2002; Mann et al. 2019) and goats (Fredeen et al. 1988) has shown that adjusting the cationic/anionic balance - (Na + K)∕(Cl + S) - by acidifying the late-pregnancy diet with added anionic salts also prevents the condition. Dietary magnesium must be adequate for calcium mobilization from bone to occur. Feeding of anionic salts will reduce bone density in periparturient goats (Liesegang 2008), which could be undesirable if carried to an extreme.
Alfalfa has a cation excess, which may be associated with decreased calcium absorption from the diet prepartum. In regions where alfalfa is plentiful or indeed the only hay readily available, the prevalence of milk fever in goats does not seem to be increased. This may be because goats tend to come into milk production more gradually than do dairy cows. A very low-calcium diet is not needed in goats and in fact might lead to hypocalcemia, as it does in ewes. Feeds high in oxalates should be avoided, as oxalate interferes with calcium absorption and also makes calcium in the blood unavailable for metabolic functions.
Because the etiology of lactational hypocalcemia is poorly understood, prevention centers on avoiding anything that upsets feed intake or gastrointestinal function (0degaard and 0verby 1993).