Flexural Limb Deformities
Berkley Chesen
■ Definition Flexural limb deformities (FLDs) are defined as hyperflexion or hyperextension of a limb. Flexural deformities are described by the joint involved and occur in the sagittal plane, typically the distal interphalangeal joint, metacarpophalangeal/metatarsophalangeal joint, carpus, and rarely the tarsus.
Although commonly referred to as “contracted tendons,” the tendons themselves are not truly contracted but rather functionally short relative to the adjacent bone, as only the muscular component can truly contract. Flexural limb deformities can be classified as either congenital or acquired. Flexural deformities are very common in horses and cattle. Small ruminants and camelids are much less commonly affected.■ Pathogenesis Congenital flexural deformities (present at birth) are likely caused by a multitude of factors. Although intrauterine positioning has been suggested, it is likely only one cause of FLDs. Exposure of the mare during pregnancy to diseases and teratogenic agents is a possible cause of congenital FLDs. Evidence behind an absolute inciting cause is lacking, but the following have been implicated in contributing to FLds: deficiency in glycogen branching enzyme in Quarter Horse foals that is transient, ingestion of locoweed and hybrid Sudan grass, equine goiter, defective crosslinking of collagen and elastin formation from lathyrism, neuromuscular disorders, and viruses.1-5 It is common for foals with congenital flexural deformities to have other anatomic abnormalities, such as spinal

FIG. 38.34 Flexural deformity of the distal interphalangeal joint.
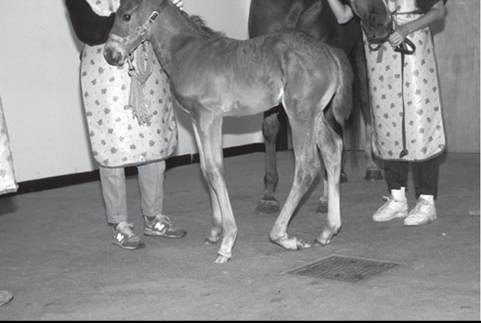
FIG. 38.35 Flexural deformity of the metatarsophalangeal joint.
deformities that may result in dystocia. In a recent study of Thoroughbred foals in New Zealand, it was found that of 203 foals, 67% had at least one FLD (58% laxity, 38% contracted). At follow-up, 93% had improved with conservative management. Male foals were more likely than female foals to have FLDs, and gestation length was 347 ± 9 days for all foals. Age of the mare was found to be a significant factor (62% of mares younger than 12 years had foals with FLDs versus 79% of mares 12 years and older).6
Acquired flexural deformities typically are seen from 4 weeks to 4 months of age, as well as in yearlings up to 2 years old. These deformities have been implicated as part of the developmental orthopedic disease complex. There are two general theories to explain how acquired flexural deformities occur. The first theory is that the tendon unit is unable to passively elongate relative to the bone.7 In the case of the distal interphalangeal joint, the rigid deep digital flexor tendon and its accessory ligament cause a palmar rotation of the foot (club-footed) (Fig. 38.34). Flexural deformities in the metacarpophalangeal joint often occur during rapid growth in the distal radius, leading to a functional shortening superficial digital flexor muscle-tendon unit. The second theory is that longitudinal bone growth cannot create a functional shortening of tendons and that increased tension within the tendon induces pain leading to the deformity.8 Acquired deformities are often noticed with a very acute onset (24 hours), which may add validity to the latter theory. Pain may initiate the deformity, but this can become a permanent condition if not addressed promptly, causing contracture to occur. Contracture results from fibrodesis of the joint capsule and periarticular structures.7
■ Diagnosis
CONGENITAL DEFORMITIES. Digital hyperextension deformities occur in neonates due to lack of tension in the flexor muscles. Typically these deformities correct without intervention within a few weeks.
In severe cases, the palmar or plantar surfaces of the foal's pastern and fetlock area may become ulcerated due to contact with the ground if not protected.Contractural deformities may involve one or a combination of the superficial digital flexor tendon, deep digital flexor tendon, or suspensory ligament. Congenital flexural deformities most commonly affect the carpus and metacarpophalangeal/ metatarsophalangeal joint (Fig. 38.35).9 Flexural deformities of the distal interphalangeal joint and the tarsus occur less frequently. In some pony breeds and miniature horses, lateral luxation of the patella results in the stifle showing a flexural deformity. This is usually due to a hypoplastic trochlear groove. Depending on the severity of the deformity, if the metacarpophalangeal joint is affected, the foal may or may not be able to stand.7 Although not truly a flexural deformity, rupture of the common digital extensor tendon results in a similar appearance. This can result secondary to flexural deformities. These foals have a characteristic swelling on the dorsolateral aspect of the carpus. Often these foals bow at the carpus due to the lack of support over the lateral aspect of the carpus.2,10 More importantly, foals with ruptured common digital extensor tendons should be checked for incomplete ossification of cuboidal bones, as these conditions often occur together.7
ACQUIRED DEFORMITIES. The most common acquired flexural deformity involves the distal interphalangeal joint and typically occurs within the first 4 months of life. The affected limb will have a more vertical hoof wall angle with a shorter toe than the unaffected limb; however, the condition is often bilateral. The heel will get longer on the affected limb, the metacarpophalangeal joint will concurrently begin to hyperextend, and the toe will undergo more wear, potentially causing issues with the white line. Two stages have been used to describe flexural deformities of the distal interphalangeal joint: stage I is defined as an angle of less than 90 degrees between the dorsal hoof wall and the sole; stage II is defined as a dorsal hoof wall that exceeds vertical.11
Early detection of flexural deformity of the metacarpophalangeal joint is characterized by a straight fetlock angle, or upright conformation.
More severe deformity of this joint is evident by buckling at the fetlock. By placing pressure in a dorsal-palmar direction on the fetlock, the flexor tendons are stretched, allowing the practitioner to determine which structure is tightest, which is important for selecting an appropriate treatment.7 It is also important to palpate the limb while not bearing weight to determine whether adhesions are present.Carpal flexural deformities tend to occur within the first 6 months of life. These foals tend to be fast-growing, heavier foals (Fig. 38.36). Although not as common, flexural deformities of the proximal interphalangeal joint occur and are usually bilateral, affecting the hind limbs.7 The exact mechanism is unknown, but it is thought that as the musculotendinous unit of the deep digital flexor complex shortens, the superficial digital flexor tendon becomes more lax.12 This can lead to a dorsal subluxation of the joint. Often a clicking sound is appreciated when the foal walks. This condition is most often seen in weanlings with a high growth rate.7
Flexural deformities also occur after foals or horses are non-weight-bearing for a period of time. These deformities
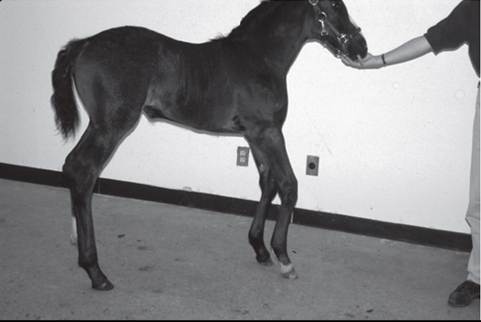
FIG. 38.36 Bilateral, mild carpal flexural deformity.
can be permanent if the joint undergoes “contracture” or fibrodesis (fixed without osseous ankylosis).7
■ Treatment
CONGENITAL DEFORMITIES. Hyperextension deformities require exercise to hasten recovery. Excessive exercise is contraindicated, as this leads to fatigue and possible injury. Treatments include swimming, corrective shoeing, and light bandaging when indicated. Swimming allows muscle tone to increase without bearing weight on the limbs. If the foal's toe lifts off the ground when weight bearing, glue-on shoes with a heel extension may be indicated. It is important not to leave glue-on shoes on a growing foal for an extended period since they may prevent the foot from expanding normally; changing them every 10 days is indicated.
Bandaging is necessary only in cases where the palmar or plantar surface of the pastern or fetlock is in contact with the ground to prevent ulcerations of the skin and should not be supportive of the structures. Excessive bandaging and support will only cause more laxity and should be avoided.Treatment for congenital flexural deformities should include pain management by judicious use of NSAIDs such as phenylbutazone at 1.1 mg/kg IV or PO daily or flunixin meglumine at 1.1 mg/kg IV or PO daily. The use of gastroprotectants such as omeprazole (4 mg/kg orally daily) is strongly suggested to help avoid the ulcerogenic effects of NSAIDs.
Oxytetracycline at a dose of 44 mg/kg diluted in physiologic saline given slowly intravenously has been used for many years in foals with flexural deformities.13 Renal function of the foal should be taken into consideration prior to administration of oxytetracycline. There are many proposed mechanisms for how oxytetracycline works to achieve a decrease in the angle of the metacarpophalangeal joint. One mechanism proposes the chelation of calcium resulting in muscle contraction.13 Oxytetracycline has been shown to be a neuromuscular blocking agent; however, this mechanism does not explain why other muscle groups are unaffected.13 An in vitro study showed that oxytetracycline also works through matrix metalloproteinase 1 mRNA expression to inhibit tractional organization of collagen fibrils by myofibroblasts (the primary cell type in the DDFT and accessory ligament of the DDFT); this interaction may cause relaxation of the musculotendinous unit.14 Regardless of the mechanism of action, foals treated with oxytetracycline should also undergo forced exercise to make the improvement permanent. Without exercise, the angle of the metacarpophalangeal joint tends to return to its previous value within 96 hours.15
A fairly new product on the market available to veterinarians is Leg Aide (Progressive Nutrition, Hopkins, Minn.), which has anecdotally positive results when used in conjunction with other therapies.
Toe extensions benefit the foal in two ways. First, they help protect the toe from being overworn; second, they lengthen the breakover of the foot, adding strain to the flexor tendons, potentially helping stretch them. Toe extensions may be made using acrylic hoof products or glue-on shoes with built-in extensions. In severe cases, the dorsal hoof wall should be incorporated into the shoe to prevent excessive strain at the toe and separation of the white line. Shoes and extensions should be removed within 2 weeks, as they can prevent the hoof from growing and expanding naturally in a young foal. Typically, 2 weeks is plenty of time to achieve correction. For foals with deformity of the distal interphalangeal joint, frequent rasping of the heels will help stretch the deep digital flexor tendon.
Splints and casts have been used to treat flexural deformities by giving support to the limb, thereby allowing the muscletendon unit to relax. When using splints, it is vital to use plenty of padding on the limb and to change the padding every time the splint is changed to ensure that pressure sores are not developing. Pressure sores can be very serious and even life threatening. Splints are made from a variety of materials but most commonly from polyvinyl chloride pipe that has been cut in an appropriate length and width; commercially made splints are also available. Splints are applied by placing the splint over the padding on the palmar or plantar surface of the limb. If the flexural deformity involves the distal interphalangeal joint, the splint should touch the ground. If the deformity is in the carpal region, the splint should end at the fetlock. Splints should be left in place for a period deemed adequate for the individual patient, ranging from several hours to 2 to 3 days.7,9 One major advantage of splints over casts is that they may be removed every few hours if desired. Casts used for the lower limb are typically half-limb casts, incorporating the foot. The exception to this is for the carpal region, where a tube cast is more appropriate, ending at the fetlock. Casts should never be left in place for longer than 2 weeks at a time due to the rapid growth rate of foals. Cast sores are a very serious complication and a legitimate disadvantage to using them.
A combination of conservative treatments should be considered when treating foals with flexural deformities. If nonsurgical management does not correct the problem, surgical intervention may be necessary; however, foals with severe congenital contractural deformities have a poor prognosis. Surgery is more often attempted for foals with carpal contracture. Other congenital contractural deformities usually respond to nonsurgical treatments. Surgical correction for contractural deformities in the carpal region involves transection of the tendons of the flexor carpi ulnaris and ulnaris lateralis as well as transection of the palmar carpal fascia.7,9 The prognosis for mild to moderate congenital flexural deformities is good for an athletic future if the foal improves over the first 2 weeks and is able to stand and nurse.9 Flexural deformities that can be straightened manually have a better prognosis than those that cannot be straightened.
Foals with ruptured common digital extensor tendons are best treated nonsurgically. Affected foals should be confined to stall rest with the application of a splint.10 As with any splint, it should be well padded to protect the limb. The splint will provide support to the limb and help protect immature cuboidal bones, which often accompany this condition.7
ACQUIRED DEFORMITIES. Conservative management for acquired flexural deformities is very similar to that for congenital flexural deformities. Other conservative therapies include dietary restrictions, including early weaning. Surgical management is selected for those cases that are unresponsive to nonsurgical treatments.
For flexural deformities of the distal interphalangeal joint, desmotomy of the accessory ligament of the deep digital flexor tendon (ALDDFT) is indicated. This surgery has an excellent prognosis for full athletic potential for stage I horses. For more severe flexural deformities of this joint (stage II), a tenotomy of the DDFT may be necessary.16 This procedure is not performed to promote an athletic career. It is acceptable for pasture soundness, breeding animals, and some light riding. Gradual rasping of the heels should be combined with any treatment for flexural deformities of the distal interphalangeal joint. Integrative therapy such as acupuncture may be considered to help achieve analgesia, muscle relaxation, and a level of sedation to help achieve physical therapy.17 A recent study evaluated desmotomy of the ALDDFT in 13 mature horses (2 years or older) suffering from lameness isolated to the foot with FLDs of the distal interphalangeal joint.18 Lameness was decreased in 9 of 13, with 10 of 13 performing at their level of intended use, indicating that this procedure should be considered in older horses.18
Acquired flexural deformities of the metacarpophalangeal joint are treated nonsurgically with a combination of NSAIDs, corrective shoeing (raising the heel with or without a vertical bar shoe with rubber dorsal tubing), and splints. Physical therapy has been used to help stretch the tendons by having the horse hop on one leg by holding the other up in a flexed position moving in a lateral direction toward the down limb.7 If surgical correction is needed, it is important to first determine which structure is creating the tension. Most commonly the superficial digital flexor tendon is involved; however, the deep digital flexor tendon and even the suspensory ligament may be involved. For treatment of contracture of the superficial digital flexor tendon, desmotomy of the accessory ligament of the superficial digital flexor tendon is performed. If the deep digital flexor tendon is the most taught, desmotomy of the accessory ligament of the deep digital flexor tendon is completed. Both accessory ligaments may be cut when indicated.17 In very severe cases, the suspensory branches may be transected, but this procedure is done for salvage, as it usually leads to subluxation of the proximal interphalangeal joint.7
Carpal flexural deformities are treated with splints and controlled exercise. Early weaning should be considered in these foals. If surgery is necessary, a tenotomy of the flexor carpi ulnaris and ulnaris lateralis in addition to splints may yield good results.
Flexural deformities of the proximal interphalangeal joint are not as common, but can be very serious to the future athletic potential of the horse. Over time, the soft tissues around the joint will fibrose and the proximal interphalangeal joint may undergo degenerative joint disease. At this stage, a pastern arthrodesis may be necessary to achieve a pain-free and potentially sound limb. Desmotomy of the ALDDFT, as well as the tendon of the medial head of the DDFT (level of the chestnut), may benefit affected horses early in the disease process.7,12